Adrenal insufficiency is a condition that occurs when the adrenal glands become damaged. Due to this, they are unable to produce the required amounts of several important hormones. These include cortisol and aldosterone. People with adrenal insufficiency, which by the way is often confused with “fatigued adrenal syndrome,” have lower levels of the hormones cortisol and aldosterone than healthy people. In this article we will look at what adrenal insufficiency is, the symptoms and causes of this condition.
The adrenal glands are truly amazing in that they produce dozens of different vital hormones every day. Some of these are so-called “stress hormones,” such as cortisol, which have many important roles in the body:
- regulate electrolyte balance,
- regulate fluid retention and body weight,
- help you sleep well at night and concentrate during the day,
- give you sexual desire
- and much more.
This is why adrenal insufficiency and hormonal imbalance are usually noticeable and affect every area of your life.
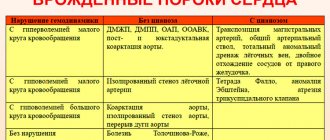
There are two main classifications of adrenal diseases. One type, called Addison's disease, is caused by diseases of the adrenal glands themselves, including adrenal cancer, infection, or bleeding (called "primary adrenal insufficiency"). This type is less common and usually causes physical damage to the adrenal glands that can be detected.
The second group of adrenal gland disorders is much more common and develops despite the absence of physical diseases in the adrenal glands, but rather related to stress or autoimmune reactions. It's called "secondary adrenal insufficiency." It leads to severe hormonal imbalances and symptoms.
Symptoms of adrenal insufficiency
Stages
There are 3 main stages of the onset of this disease:
- Addison's disease (primary type) , the development factors of which are a decrease in the functioning of the immune system, tuberculosis, human immunodeficiency virus, venereal disease and fungal viruses. Due to weakened immunity, the layer of the adrenal cortex is rejected;
- Secondary adrenal insufficiency develops with brain tumors, after surgery or head injuries, and heavy bleeding. Long-term therapy with glucocorticoids can also cause;
- The tertiary type manifests itself in connection with radiation, operations, intoxication and anorexia nervosa.
The adrenal glands are one of the organs that are most supplied with blood in the body, as well as the thyroid gland. For this reason, when the tasks performed by the adrenal cortex are disrupted, metastasis occurs in the presence of oncology in the lungs.
Classification of the disease
In the international classification of diseases, the disease code according to ICD 10 is E27. The cortical layer of the organ produces various hormonal substances, male and female sex hormones. With the primary pathology of adrenal insufficiency, a deficiency of cortisol and aldosterone develops in the body.
If the pathology occurs due to a disorder of the functions of the hypothalamus and pituitary gland, a secondary stage of pathology is diagnosed - more pronounced adrenal insufficiency. The pathology is accompanied by various clinical symptoms.
To determine the stage of the disease, it is important to perform tests for hormone levels. It is also necessary to undergo a complete examination of the body and check the blood. In the tertiary pathology of adrenal insufficiency, the hypothalamus produces a small amount of the substance corticoliberin.
Iatrogenic adrenal insufficiency can also occur when the receptors are blocked and there is no sensitivity to aldosterone and cortisol. Primary insufficiency is the most severe; in this pathology, the adrenal glands do not produce the necessary substances.
Symptoms of adrenal insufficiency
Photos of symptoms of the disease Acute adrenal insufficiency
Any type of disease has early manifestations; with NN, the following symptoms can be distinguished:
- fatigue and drowsiness;
- high level of sensitivity to sunlight;
- reducing the body's resistance to infections;
- loss of appetite;
Laboratory studies of the disease revealed a number of associated symptoms, such as:
- change in skin color at the bends of the limbs, etc.;
- modification of the color of the mucous membrane from golden to gray;
- a sharp drop in blood pressure (BP);
- increased heart rate and shortness of breath due to the development of tachycardia;
- digestive tract disorder;
- spasms in the gastrointestinal tract;
- weight loss;
- rapid muscle fatigue and difficulty moving.
The manifestation of the chronic stage in adolescents occurs with the following symptoms: brown pigmentation of scars, skin folds and gums . Also fatigue, vomiting for no reason and increased salt intake, low blood sugar . With the development of the acute form of the disease, children experience diarrhea, vomiting and pain in the abdominal area. Also, when fluid is lost in large volumes, the skin acquires a bluish color and cold body temperature. You may experience fainting, drowsiness, and seizures.
Manifestation of the disease at various stages
Primary adrenal insufficiency reduces or increases hormonal levels, and inflammation of the endocrine gland and type 1 diabetes mellitus appear. The disease develops in 85-90 percent of cases, due to the destruction of adrenal tissue.
In the second and third forms of adrenal insufficiency, symptoms appear to a much lesser extent.
Causes of pathology
Adrenal hypoplasia can cause a decrease in the synthesis of hormonal substances. The disease occurs from damage to certain centers in the body that regulate the functions of the endocrine system.
Autoimmune adrenal pathology develops with various immune responses and its disorders. The human immune system perceives various reactions as foreign. Many autoimmune pathologies and damage to healthy tissues develop. Such disorders require careful diagnosis and treatment.
The causes of the disease are:
- autoimmune disorders;
- congenital anomaly of the cortex;
- pathology of the hypothalamus;
- tuberculosis;
- hemorrhage caused by infection;
- Smith-Opitz syndrome;
- accumulation of protein compounds in organ tissues.
Secondary hypocortisolism is caused by various infections that occur due to injuries, hemorrhage, and tumors. Disorders appear due to organ destruction and are sometimes associated with long-term use of synthetic glucocorticoids.
A lack of ACTH and pituitary substances is observed with congenital decrease in body weight. The pituitary gland can be affected by its own antibodies, which also inevitably leads to disruption of the adrenal glands.
In children, congenital adrenal cortex pathology is possible; its insufficiency manifests itself in different ways. Symptoms include skin pigmentation, weakness and tremors of the limbs, poor functioning of the heart and blood vessels. A crisis may develop.
Complications of adrenal insufficiency
A complication, also called an adrenal crisis, can occur when the functions of the adrenal cortex are disrupted; problems in the functioning of one of the organs or the whole organism may arise. Possible development into a comatose state.
The complication is characterized by:
- severe decrease in blood pressure, possible fainting;
- severe weakness, loss of space;
- frequent vomiting and unstable stools;
- dehydration of the body;
- heart failure;
- cramping and severe pigmentation.
Also, the acute form is often closely related to chronic manifestations. Exacerbation may occur due to the following factors:
- previous viral infection during illness;
- stopping taking medications prescribed for treatment;
- suffered stress and other negative emotions;
- sudden change in climate zone;
- increased physical activity;
- trauma or surgery in the abdominal cavity.
When sick, women often experience disruptions to their menstrual cycle, and men's potency.
Diagnosis of the disease.
Diagnosis first begins with asking the patient or adult relatives about the general condition, what are the manifestations and symptoms involved in the deterioration of the condition. They find out the reasons why this problem could arise and take into account the patient’s complaints.
Complications
The most serious complication of hypocortisolism is considered to be adrenal crisis, which often leads to a coma. In this case, there is an increase in panic, a drop in blood pressure, uncontrollable vomiting with subsequent dehydration, and heart rhythm disturbances.
Diagnostic methods.
The initial step in identifying pathology is to prescribe an ultrasound examination (ultrasound). Such an examination should show the following origins of the disease:
- the presence of tuberculosis infection and excess of calcium salts indicates that the cause of insufficiency is tuberculosis;
- the detection of an autoantibody to the 21-hydroxylase antigen is the reason for the diagnosis of an autoimmune manifestation of hypocortisolism.
The next stages of examination are diagnostics using magnetic resonance imaging (MRI) and computed tomography (CT) . In the secondary stage, the same procedures are performed, including MRI of the brain.
If the doctor doubts the diagnostic results, he may conduct a stimulation test, in the form of hormones produced by the pituitary gland and hypothalamus. This will allow you to find out the content of a biologically active hormone in the blood; it is also called the “stress hormone” (cortisol).
A general blood test is required for donation. Which will show sodium ion concentration, high potassium content, increased lymphocyte count, decreased or increased eosinophil count, decreased white blood cell count.
Prevention and prognosis of the course of the disease
With timely and rational treatment of adrenal insufficiency, the quality of life of patients with this disease improves significantly. The prognosis for the course of the disease is very favorable - the patient’s life expectancy is the same as that of a practically healthy person.
There is no special prevention of the disease in modern medicine; the course of chronic hypocortisolism depends on the prevention and relief of adrenal crises.
The main method of preventive measures for congenital underdevelopment of the adrenal glands, and subsequently acute adrenal insufficiency, is to avoid the harmful effects of nicotine and alcohol
First of all, patients with hypofunction of the adrenal cortex and people at risk (those with a hereditary predisposition, taking corticosteroid drugs for a long time) need to register with a qualified endocrinologist.
Any form of adrenal insufficiency is a formidable and unpredictable pathological process. That is why every person should know the main signs of the disease, because only an accurate and timely diagnosis will help you choose the right treatment tactics, allowing you to lead your usual lifestyle.
Treatment
Modern medicine can provide treatments for this disease, and this depends on the cause and factors that projected the disease. Treatment methods are primarily aimed at eliminating adrenal insufficiency and restoring the hormone.
Treatment is carried out by taking medications for tuberculosis, fungal diseases, syphilis, getting rid of tumors, due to radiation therapy. If the treatment was carried out correctly, but did not have a sufficient effect, or contributed to other processes in the course of the disease, it is possible to support the patient with hormonal therapy for life.
Drug treatment
Prescribing and taking drugs of the glucocorticoid and mineralocorticoid groups begins. Most often, doctors prescribe Cortisone and Cortef for mild pathology. If the form is more severe, prednisolone is prescribed, in compounds in the form of “Cortisone acetate” or “Cortef with mineralocorticoids” .
Often, the onset and progression of a disease cannot occur without stress. If the patient has such manifestations, the dose of corticosteroids is increased 3-5 times. During pregnancy, higher doses are allowed only in the 2nd trimester.
Anabolic steroids are used to correct muscle mass, tone it and renew cell parts. The prescription occurs to any group of people, regardless of gender, often these are patients with a chronic course of the disease. Take 3 times a year at short intervals.
It is possible to use replacement therapy. It also provides for a gradual reduction in the use of drugs, i.e. used for subsequent cancellation. The main thing in replacement therapy is compensation of the clinical hormonal type, as well as its maintenance and preservation. In this case, the indicators will be considered:
- baseline plasma cortisol level is more than 350 mmol/l;
- Potassium within 4.0-4.5 mmol/l;
- Sodium from 135 to 140 mmol/l;
- Glucose 4.5-9.0 mmol/l per day.
If the cause of the disease is infection, antibiotic therapy is administered.
Determining improvement with medication
Improvement in condition can be determined by factors such as:
- normalization of blood pressure;
- decline in pigmentation;
- weight gain within normal limits;
- improvement of general condition;
- eradication of problems with the gastrointestinal tract;
- exclusion of anorexia;
- restoration of muscle function and more.
Often the drugs offered by specialists are classified according to duration of action and quantity, as follows:
- Short-acting: Hydrocortisone – 20 mg;
- Cortisone – 25 mg;
- Prednisone – 5 mg;
- Prednisolone – 5 mg;
- Methylprednisolone – 4 mg.
- Triamcinolone – 4 mg;
- Dexamethasone – 0.75 mg;
In case of mild deficiency, only Cortisone , but if the degree of damage is higher, Prednisolone and Fludrocortisone .
Fludrocortisone is an analogue of the mineralocorticoid aldosterone. It is always used regardless of the degree of deficiency. For example, if a child takes only glucocorticosteroids, weight gain will be very small. There will also be other problems: delayed psychomotor development, dehydration . The latter is most dangerous because the body can be filled with a lethal dose of potassium. Whether adult or child, treatment with corticosteroids alone may worsen the condition but also increase the chance of developing salt-wasting crises.
You can understand that the dose of Fludcortisone has been prescribed correctly by the following signs:
- drop in sodium levels;
- increase in potassium substances;
- increase in renin activity.
An overdose of this drug will show its properties as follows: if during treatment swelling in the face and other areas appears, blood pressure rises, migraines and insomnia appear, and laboratory indicators show that there is a minimal amount of potassium in the blood and an increased level of sodium. Thus, you should reduce the amount consumed, but there is no need to cancel it at all.
Important! The dosage is increased only if the patient lives in hot climate zones, since sodium substances are excreted through sweat; during pregnancy, an increase is made from the second trimester.
If, in addition to the disease, an infectious disease with fever appears, if it is necessary to perform a traumatic operation, in order to avoid a subsequent Addisonian-type crisis, increase the dosage of the glucocorticoid drug by 3-5 times. Mineralocorticoids remain at the same dosage.
The effectiveness of treatment is checked every 30 days by testing the activity of hormones and electrolytes in the blood. Subsequent checks, when a person takes medications for a long time, take place every 2-3 months.
In case of diseases of the adrenal glands, it is possible to exceed the norm for taking glucocorticoids by 1-2 days in order to avoid the formation of an acute form of insufficiency.
Surgical operations
Surgical actions aimed at surgical intervention to restore the adrenal cortex are a complex process that can only be performed by highly qualified specialists. The recommended removal of the adrenal gland or its tissues or tumor is prescribed according to the doctor’s indications.
When removing a tumor, the quality factor (malignant and benign category) and the ability to produce hormones should be taken into account. Hormone levels are determined by taking blood and urine tests, and such types of examinations as:
- blood test for chromogranin A, renin, aldosterone, cortisol, ACTH hormone, calcitonin, blood ions and parahormone (parathyroid);
- urine test readings for metanephrines (adrenaline metabolite) and cortisol.
They are sent to the surgical table when the hormone production exceeds the established norm, or treatment of a malignant tumor is impossible, as prescribed by the doctor, based on the tests performed.
Features of treatment
If you notice symptoms that indicate adrenal insufficiency, you should consult a doctor. You will need to take a general and biochemical blood test (including hormone tests), undergo an ultrasound, MRI and other types of examinations.
Adrenal insufficiency , which is accompanied by symptoms such as weakness, nausea and vomiting, must be treated urgently to prevent adrenal crisis and possible death . If the disease develops gradually, the doctor directs measures to treat the cause that provoked the problem, as well as restore the hormonal balance in the body by taking hormonal drugs or medications that reduce the production of hormones. Particular attention should be paid to diet.
Depending on the situation, the doctor may prescribe immunomodulators, immunosuppressants, physiotherapy, and herbal infusions. Sometimes surgery is necessary, and in the case of cancer, chemotherapy.
Alternative home treatments
You can start using folk remedies only after a diagnosis has been made. The use of herbs and mixtures is considered to be quite effective methods, but this should only be done with a doctor’s testimony, not on your own, as it is life-threatening.
The main goal of herbal treatment is to restore hormonal levels, both to suppress and to raise levels. The quantity, type and methods of use are prescribed by the attending physician. To treat disorders of the adrenal glands, it is recommended to take the following infusions:
- Horsetail – promotes the production of hormones, cleanses the body of toxic substances, and promotes the functioning of water salt balance. Take with caution to people with diseases of the blood systems;
- Geranium – containing radium molecules, promotes the production of hormones;
- Currant leaves and vitamin C – have preventive properties, warn the immune system against various types of diseases;
- The sequence – promotes the enrichment of minerals, restores the gastrointestinal tract, stimulates the adrenal glands.
There are herbal infusions that should be taken strictly according to the instructions and only under the supervision of a specialist; such folk remedies include licorice root. It has the properties of blocking hormone destruction.
Also, nettle ensures good metabolism and restores adrenal function, increases the number of red blood cells in the blood, reduces sugar, and mulberry leaves relieve inflammation in the kidneys.
Diet and prohibited foods to take when sick
If you have adrenal insufficiency syndrome, you should not eat foods high in sugar, as it can trigger the release of insulin, which is a big problem for the body.
Products that should be limited, or better yet completely excluded from the diet: chips, mayonnaise, sausages, coffee, instant noodles, alcoholic, carbonated and energy drinks and salt . It is also worth carefully monitoring the composition of products to ensure that they do not contain harmful additives and dyes.
Preference should be given to fruits and vegetables, especially with the onset of the sales season, as they contain many useful vitamins that the body needs.
To normalize the condition during the day, you should follow these instructions:
- a good breakfast is the key to normal blood sugar levels; you can only eat before 8 o’clock;
- an hour after breakfast you need a light snack, this also applies to the time before afternoon tea and lunch;
- you should have lunch before 3 o’clock in the afternoon;
- have dinner in small, light portions up to 6 o’clock; heavy and filling foods are consumed during the day;
Vitamin complex recommended for pathology that should be taken: vitamins B5, C, Omega 3, 6, 9, magnesium, pantethine, L - Tyrosine.
Complications of adrenal insufficiency
In patients with impaired production of glucocorticoid hormones, the development of an adrenal insufficiency crisis is observed, which is characterized by an exacerbation of:
- cardiovascular failure - a sharp drop in blood pressure, tachycardia, weakening of the heart rate;
- gastrointestinal manifestations - the patient may experience uncontrollable vomiting and repeated diarrhea;
- sudden oliguria – decreased amount of urine excreted;
- neuropsychic form - the patient may experience hallucinations, loss of the body’s adaptive abilities to stressful situations.
Patients with Addison's disease should monitor the condition of the heart and blood vessels
Addisonian crisis is an acute comatose state that develops as a result of:
- already existing chronic hypofunction of the adrenal cortex;
- adrenalectomy - removal of one or both adrenal glands in Nelson syndrome (pituitary adenoma);
- abrupt withdrawal of glucocorticoid hormones;
- Schmidt's syndrome - autoimmune thyroiditis;
- Waterhouse-Friderichsen syndrome in a newborn due to birth trauma or intrauterine infection;
- hemorrhages in the adrenal glands during severe and protracted labor, with injuries to the chest and abdomen, burns, acute inflammation in the peritoneum (peritonitis), purulent inflammation of soft tissues (sepsis).
If signs of acute adrenal insufficiency appear, the patient must seek the help of a qualified specialist who will conduct a comprehensive examination and prescribe effective treatment for the acute pathological condition. Otherwise, Addisonian crisis may result in death.
Disease prevention
If a person has any suspicions, he should immediately go to the hospital, since timely diagnosis and treatment of this disease is in itself the basis for prevention.
Maintenance therapy should be intermittent. If the daily dose of the drug does not exceed 20 mg, it is best to take it in the morning. For large volumes, take as prescribed by the doctor or in the morning. To prevent withdrawal symptoms from affecting your body, it is best to gradually reduce your medication intake and only then stop taking it.
Also, people with such syndromes and problems of a similar nature need to register with an endocrinologist. If you are pregnant, limit access to tobacco places. Taking tobacco, alcohol, medications, and limiting these substances is in itself a prevention of adrenal insufficiency.
Methods for effective treatment of adrenal hypofunction
In the arsenal of modern clinical endocrinology there are many different effective methods of rational treatment of such a disease as adrenal insufficiency. When choosing them, practitioners strive to achieve:
- Eliminating the main causes of the disease.
- Replacement of hormone deficiency.
Elimination of the root cause may include:
- drug therapy for fungal diseases, tuberculosis infection, syphilis;
- surgical removal of tumors;
- antitumor radiation treatment.
Irreversible pathological processes in the adrenal glands require lifelong hormone replacement therapy
Primary hypofunction is treated with synthetic preparations of mineralo- and glucocorticoids. If the patient has mild manifestations of the disease, Cortef or Cortisone is prescribed; more pronounced manifestations require the use of hormonal combinations - Deoxycorticosterone trimethyl acetate or acetate.
With secondary hypofunction of the glands, the production of aldosterone is preserved, which is why patients are prescribed only glucocorticoid drugs.
In case of chronic adrenal insufficiency, both men and women are advised to use pharmacological analogues of male sex hormones - anabolic steroids (Retabolil, Nerabolil).
The effectiveness of drug therapy tactics is assessed by:
- blood pressure parameters;
- gradual return to normal skin color;
- weight gain;
- disappearance of dyspepsia symptoms;
- improving the general well-being of the patient.
To provide emergency care for adrenal crisis, you need:
- rapid replenishment of water balance in the body - the patient is intravenously injected with an isotonic saline solution with 20% glucose;
- hormone replacement therapy - intravenous administration of Prednisolone or Hydrocortisone, the doses of drugs are gradually reduced as the symptoms of the crisis subside;
- symptomatic treatment of pathological conditions that cause acute adrenal insufficiency.
Various stress factors for the human body (infectious diseases, injuries, surgical interventions, pregnancy) require a 3-fold increase in doses of corticosteroids. However, during the period of bearing a child, the dose of synthetic hormones can be increased only slightly.
Patients need to follow a special diet - the diet should be enriched with carbohydrates, sodium salts, proteins, fats, vitamins C and B. However, it is necessary to limit the consumption of potassium salts, which are found in large quantities in seeds, nuts, legumes, and greens.
Forecast
Removing symptoms and effective rapid treatment is quite difficult and can result in death. In the case of the chronic stage, emergency care is not required, since this form very rarely leads to death; it is enough to contact the clinic in a timely manner for a detailed analysis and subsequent treatment.
For adrenal tumors, a favorable prognosis is possible based on the removal of a benign tumor. After 1-2 months, blood pressure recovers and metabolic processes return to normal.
In the presence of malignant tumors, it is difficult to give a good prognosis; it all depends on the timing of both the visit to the hospital and the treatment process.
It is unlikely that even one specialist will be able to give an accurate forecast, since it depends on many factors. Timely treatment and treatment as prescribed will lead to improvement of the condition. Ignoring adrenal insufficiency will naturally lead to death sooner or later.
Adrenal crisis
Acute adrenal insufficiency (AAI) or adrenal crisis is characterized by a sudden and dramatic worsening of adrenal insufficiency. If the patient has the primary form, this deterioration is called Addison's crisis.
Signs of adrenal crisis include:
- Unexpected and sharp pain in the abdomen, lower back, legs.
- Diarrhea, nausea, vomiting.
- Dehydration of body tissues.
- Low blood pressure.
- Loss of consciousness.
Acute adrenal insufficiency often warns of its appearance. Therefore, if you notice the above symptoms, you should immediately call an ambulance. But sometimes signs of a crisis appear immediately, without preliminary symptoms of adrenal insufficiency. If the patient does not receive medical assistance during an attack, this can lead to his death.
It must be remembered that one timely injection of the artificial hormone glycocorticoid (corticosteroid) can save a person’s life. Therefore, patients should have ready-made corticosteroid injections with them at all times. Friends and family should be informed about this and be able to administer this injection to the patient in an emergency.
Diagnostics
Anamnesis
Primary adrenal insufficiency is characterized by an imperceptible onset and a slow increase in fatigue, muscle weakness, loss of appetite, weight loss, hyperpigmentation of the skin and mucous membranes, and hypotension.
The first symptoms of adrenal insufficiency - weakness and fatigue - are nonspecific, so it is very important to clarify the time of their occurrence, the rate of development and combination with other signs of adrenal insufficiency.
Physical examination
Hyperpigmentation is noted in the form of diffuse brown, red or bronze darkening on both open and closed parts of the body, especially in places of friction of clothing, on the palmar lines, in postoperative scars, on the mucous membranes of the oral cavity, in the area of the areolas of the nipples, anus, external genitals.
Some patients have dark freckles and areas of depigmentation - vitiligo , which suggests an autoimmune process. Vitiligo is usually found in patients who have antibodies to adrenal cells.
In women, a decrease and complete disappearance of axillary and pubic hair is noted, since their adrenal glands are the main source of androgens. Cessation of the secretion of adrenal androgens in men has little effect on the state of sexual functions and hair growth, since the main synthesis of these hormones occurs in the interstitium of the testes.
Laboratory and instrumental studies
Measuring adrenal hormone levels. Read our article physiology of the adrenal glands.
Differential diagnosis
Clinical diagnosis of the early stage of adrenal insufficiency is difficult, complaints of weakness and fatigue are very common and nonspecific.
Muscle weakness, especially when combined with irritability and mood instability, is more characteristic of neurotic syndromes. With neurocirculatory dystonia of the hypotensive type, muscle weakness is usually unstable and intensifies under the influence of psycho-emotional factors, as well as during the day. Such symptoms are not accompanied by electrolyte disorders.
Arterial hypotension requires differential diagnosis with essential hypertension.
The combination of arterial hypotension with weight loss occurs in gastric ulcers, chronic enterocolitis and pancreatitis, anorexia nervosa, and cancer. With anorexia nervosa, despite a sharp decrease in body weight, patients usually maintain good health and performance.
In septic conditions, a clinical picture resembling adrenal insufficiency (weakness, hypotension, anorexia, hypoglycemia) is observed. Primary adrenal insufficiency can be caused by sepsis (meningococcemia).
Loss of body weight and severe weakness are observed with the development of thyrotoxicosis and diabetes, however, in these cases, appetite is normal.
In case of hyperpigmentation, differential diagnosis is carried out with pellagra, dermatomyositis, scleroderma, melanoma metastases, liver cirrhosis, hemochromatosis, pigment-papillary skin dystrophy (acantosis nigricans), poisoning with heavy metal salts.
Useful video
Watch the video about chronic adrenal insufficiency:
Similar articles
- Adrenal insufficiency
Unfortunately, diseases of the adrenal glands are not always detected in a timely manner. More often they are found as congenital in children. The reasons may also be due to hyperfunction of the organ. Symptoms in women and men are generally similar. Tests will help identify diseases. Read more - Itsenko Cushing's disease and syndrome: causes, symptoms...
Many people confuse the disease and Itsenko-Cushing syndrome, but their causes are different, and so is their treatment. Symptoms manifest themselves externally, with interruptions in the functioning of all organs. Diagnosis is complex, the prognosis is not always favorable, even in children. Read more
- Endemic goiter: main causes, etiology...
One of the most common problems with the thyroid gland is endemic goiter. The etiology of the disease is based on iodine deficiency and area of residence; the symptoms of the lesion change depending on the degree of progression. The causes of diffuse goiter are one of the forms of manifestation. The complications are extremely severe. Read more
- Subclinical thyrotoxicosis: main symptoms...
Subclinical toxicosis occurs mainly in areas unfavorable for the amount of iodine. Symptoms in women, including during pregnancy, are vague. Only irregular periods can indicate the problem of nodular goiter. Read more
- Toxic goiter in children: signs, treatment...
Mostly toxic goiter in children occurs as a hereditary factor. Signs are manifested primarily by moodiness, poor sleep, and others. What is the possible treatment for diffuse toxic goiter? Read more
Pathogenesis
Primary adrenal insufficiency in autoimmune damage : antibodies target key enzymes of steroidogenesis, most often CYP21A2 (P450c21 or 21-hydroxylase). Antibodies to 21-hydroxylase are detected in 64–86% of patients with NN.
The antibody titer is highest at the onset of the disease. At the onset of the disease, there is a compensatory increase in plasma renin activity to maintain normal aldosterone concentrations, but aldosterone secretion progressively decreases.
Subsequently (after months or even years), the secretion of cortisol gradually fades away. The activity of cortisol secretion gradually decreases in response to ACTH stimulation, then basal ACTH concentrations steadily increase, then the concentration of cortisol in the blood decreases, which is accompanied by the development of corresponding clinical symptoms.
Primary adrenal insufficiency in active tuberculosis is a consequence of hematogenous dissemination of the infection. Foci of tuberculosis of extra-adrenal localization are usually detected, but clinical signs of the disease may be absent.
Adrenoleukodystrophy is a disease caused by deletion of the ALD gene (22q28), manifested by a deficiency of lignoceroyl-CoA ligase, which leads to impaired β-oxidation of saturated long-chain fatty acids in peroxisomes and their subsequent accumulation together with cholesterol esters in the cells of the nervous system and adrenal cortex in in the form of layered, trilaminar intracellular inclusions.
Metastatic destruction of the adrenal glands is most often observed in non-Hodgkin's large cell lymphoma and rheumatic fever; less often, cancer of the kidney, bladder, prostate, and colon metastasizes to the adrenal glands.
Fungal infection (coccidomycosis, paracoccidomycosis, blastomycosis) as a cause of primary CNN is rare. Subclinical NN is detected in 8–14% of HIV-infected patients. Overt clinical manifestations of ND are extremely rare and usually occur in the later stages of AIDS. Often, primary CNN in HIV infection develops as a result of damage to the adrenal cortex by an infiltrative process (cytomegalovirus and fungal infection, Kaposi's sarcoma, lymphoma, etc.).
Urgent measures
Acute adrenal insufficiency is an absolute indication for hospitalization. Treatment is carried out in a specialized ICU. At the beginning of treatment, especially if the patient is unconscious, it is necessary to install a urinary catheter and a gastric tube.
Rehydration
Without waiting for the results of hormonal studies, intravenous administration of 2–3 liters of 0.9% sodium chloride solution is started as early as possible. The infusion rate should be 500 ml/h (in a collaptoid state - in a stream). Subsequently, a 5–10% glucose solution is added to an isotonic sodium chloride solution. During the first day, at least 4 liters of liquid are administered. The administration of potassium-containing, hypotonic solutions and diuretics is contraindicated.
For repeated vomiting, intravenous administration of 10–20 ml of 10% sodium chloride solution is recommended at the beginning of treatment and repeated administration in case of severe hypotension. In addition to an isotonic solution of sodium chloride and glucose, if necessary, polyglucin in a dose of 400 ml and blood plasma are prescribed.
Glucocorticoid replacement therapy
The drug of choice is hydrocortisone. In large doses, it provides both gluco- and mineralocorticoid effects.
Hydrocortisone hemisuccinate (solu-cortef) is administered both intravenously and intramuscularly. Hydrocortisone acetate suspension must be administered intramuscularly only. Hydrocortisone acetate acts slightly longer than hemisuccinate.
At the same time, hydrocortisone is administered intravenously in a bolus at a dose of 100 mg. Then, during the first day, 100 mg of the drug is administered intravenously or intramuscularly every 6-8 hours. During the first day, the total dose of hydrocortisone is 400-600 mg, less often (in severe cases) - 800-1000 mg, sometimes more.
In the absence of hydrocortisone, intravenous administration of 4–8 mg of dexamethasone is possible, followed by transition to hydrocortisone therapy.
Intravenous administration of hydrocortisone is continued until the patient recovers from collapse and systolic blood pressure increases by more than 100 mm Hg. On the 2nd–3rd day, when the patient’s condition has stabilized, the dose of hydrocortisone is gradually reduced to 150–200 mg/day, then its intramuscular administration is continued 4–6 times a day at a dose of 50–75 mg.
When the dose of hydrocortisone becomes less than 100 mg/day, fludrocortisone (Cortineff) is added to therapy at a dose of 0.1 mg/day. When the daily dose of hydrocortisone is more than 100 mg, there is no need to prescribe mineralocorticoids.
It usually takes up to five days to reach a maintenance dose of hydrocortisone. Treatment with hormonal drugs should be carried out in adequate quantities under the control of sodium, potassium and blood sugar levels, as well as blood pressure. The insufficient effectiveness of treatment for Addisonian crisis may be associated with a small dose of hormonal drugs or salt solutions, or a rapid reduction in the dosage of drugs.
Antibiotic therapy
In cases of fever (except those arising from severe dehydration), antibiotics should be prescribed even in the absence of an obvious focus of infection.
Symptomatic therapy
If it is impossible to stabilize hemodynamics with glucocorticoids alone, additional administration of catecholamines and analeptics is indicated.
Further management
After stabilizing the patient's condition and reducing the daily dose of hydrocortisone to less than 100 mg/day, the patient is transferred to continuous replacement therapy with hydrocortisone tablets.
Etiology
Primary adrenal insufficiency can develop due to several reasons:
- Autoimmune damage to the adrenal cortex - often combined with other autoimmune endocrinopathies - the so-called autoimmune polyglandular syndrome .
- Tuberculosis.
- Bacterial/infectious damage to the adrenal glands (HIV infection, fungal infections, syphilis, amyloidosis);
- Metastases of primary tumors of extra-adrenal localization;
- Adrenoleukodystrophy (Simmerling-Creutzfeld disease, melasma leukodystrophy) is a genetic disease with an X-linked recessive type of inheritance, occurring with predominant damage to the white matter of the nervous system and the adrenal cortex;
- Total removal of the adrenal glands (for example, in Itsenko-Cushing's disease);
- Bilateral hemorrhage into the adrenal glands during anticoagulant therapy;
- The use of blockers of steroidogenesis in the adrenal glands (aminoglutethimide, mitotane, ketoconazole, barbiturates, spironolactone).
Clinical picture
Primary adrenal insufficiency manifests itself most often - severe general and muscle weakness - at the onset of the disease it can occur periodically, during stress. Then their intensity increases towards the end of the day and goes away after a night's rest; later, with the progress of the disease, weakness increases and becomes constant, acquiring the character of adynamia. Along with physical adynamia, neuropsychic asthenia develops up to the development of stupor or psychosis.
Weight loss is a mandatory symptom of adrenal insufficiency and is associated with decreased appetite, impaired intestinal absorption, and dehydration.
Hypotension , a characteristic symptom of primary adrenal insufficiency, is often noted in the early stages of the disease. Dizziness and fainting are caused by a decrease in blood pressure. Hypotension is characterized by a systolic blood pressure level of 80–90 mm Hg, diastolic blood pressure below 60 mm Hg. Blood pressure in patients with concomitant hypertension is normal or moderately elevated.
Hyperpigmentation of the skin and mucous membranes is a common and early sign of primary adrenal insufficiency. At the onset of the disease, patients note long-term preservation of the tan after sun exposure.
Gastrointestinal disorders (loss of appetite, nausea, vomiting) are sometimes observed at the onset of the disease and always with increasing adrenal insufficiency. Less common are stool disorders (diarrhea or constipation). Some patients feel a constant need for salty food.
Hypoglycemic conditions occur both on an empty stomach and 2–3 hours after eating a meal rich in carbohydrates. Attacks are accompanied by weakness, a feeling of hunger, and increased sweating.
More than half of the patients experience dysfunction of the central nervous system in the form of decreased mental activity and memory, apathy, and irritability.
Nocturia is often noted against the background of decreased glomerular filtration and renal blood flow.
Prevention
Main preventive areas:
- early diagnosis and proper management of patients with CNN;
- training patients with congenital insufficiency in the rules for changing the dose of replacement therapy drugs during intercurrent illnesses, injuries and other stressful situations;
- preventive administration of glucocorticoids in high-risk situations (for example, tooth extraction in a patient with severe thyrotoxicosis, stress or surgical interventions in persons receiving glucocorticoids for non-endocrine diseases, etc.);
- timely diagnosis and treatment of diseases leading to the development of ONN.
Patients themselves, as well as doctors of various specialties (primarily surgeons, obstetricians-gynecologists and anesthesiologists) should be trained in the rules for increasing doses of glucocorticoids in the event of concomitant diseases in patients with congenital incontinence.
For mild colds not accompanied by fever, or conditions of similar severity, the dose of glucocorticoids taken by the patient should be increased by 2–3 times. For minor and short-term interventions (EGD, tooth extraction), a single intramuscular injection of 50 mg of hydrocortisone is indicated 15–30 minutes before the procedure.
For severe somatic diseases (flu, pneumonia), it is recommended to switch to intramuscular injections of 150–200 mg of hydrocortisone per day.
During childbirth and operations
For large-scale interventions and childbirth, the following patient management regimen is recommended: before surgery (the onset of labor), 75–100 mg of hydrocortisone is administered intramuscularly; during surgery (childbirth), 100–300 mg of hydrocortisone hemisuccinate is administered intravenously in a 5–10% glucose solution (in depending on the duration of the intervention). If the course of the postoperative period is smooth, 100–150 mg of hydrocortisone per day is administered intramuscularly in the first three days, then 75–100 mg/day for 3–5 days, after which the patient is transferred to tablet drugs according to the usual regimen.
Previously treated with glucocorticoids
A special group of patients potentially susceptible to AUI are patients previously treated with glucocorticoids for non-endocrine diseases. Long-term (>1.5 months) use of glucocorticoid drugs (15 mg prednisolone or its equivalent) reduces the activity of the hypothalamic-pituitary-adrenal system. Withdrawal syndrome, which occurs as acute insomnia, occurs in patients with a rapid reduction in the dose of hormones, so the abolition of glucocorticoids must be done gradually. If the dosage exceeded 15 mg of prednisolone (or its equivalent), then you can reduce the dose quickly enough (by 2.5–5.0 mg of prednisolone every 2–3 days) to 15 mg, then withdraw more slowly, by 1/4 tablet prednisolone (or equivalent) every 7–10 days.
After complete withdrawal of glucocorticoids for a year, in such patients, due to surgical, infectious or other stress, failure of the adrenal cortex function may develop, requiring drug correction.
Causes of the disease
Each form of hypocortisolism has its own factors that cause it, they can overlap with each other. Causes of primary form of deficiency:
- Pathology of the cortex and the organ itself, developing in utero, is congenital.
- The autoimmune origin of the disease is associated with disorders of other organs of the endocrine system. This is the main cause of hypocortisolism. With this pathology, the adrenal glands' own protective antibodies attack their tissues. In up to 50% of cases, this is associated with diseases of the thyroid gland, in particular thyroiditis.
- Pulmonary tuberculosis in a widespread form, affecting other organs.
- Genetic disorder - adrenoleukodystrophy. Associated with a lack of enzymes that break down lipids (fats). In this case, unprocessed fatty acids accumulate in the tissues of the adrenal glands and cause pathological abnormalities in their work.
- The cause may also be oncological diseases and their metastases.
- Trauma and surgical procedures.
- Necrotic changes in tissues associated with infectious diseases of the genital organs, HIV, syphilis, etc.
- Taking medications that have side effects that damage the adrenal glands.
- Aggravating factors may include diseases of the cardiovascular system and fungal diseases.
(The picture is clickable, click to enlarge)
Causes of secondary and tertiary forms:
- Hypocortisolism can develop as a complication after infectious diseases.
- Congenital pathologies of brain regions. Dysfunction of the hypothalamus and pituitary gland.
- Injury to adrenal tissue, for example, rupture of the organ. Other causes may include surgery or radiation therapy.
- Autoimmune brain disorders.
- Benign and malignant neoplasms in the hypothalamus and pituitary gland. Hemorrhages in these areas.
- Long-term use of drugs that inhibit the functions of brain and adrenal activity.
How to get rid of adrenal insufficiency?
The entire process of treating such a constant and sluggish disease should be aimed at artificially replacing missing hormones and eliminating the pathological agent that led to organ damage (improving foci of inflammation, surgical intervention to eliminate tumors).
A diet with a high content of proteins, vitamins, calories and table salt up to 10 g/day is recommended, and alcohol intake is completely limited. Patients should try to avoid heavy physical and nervous stress as much as possible and get more rest. Patients should mentally prepare for the need for lifelong use of synthetic hormonal drugs (prednisolone, hydrocortisone and others) and the possibility of side effects.
Artificial hormones are drugs with a very complex prescription regimen; increasing and decreasing the dose depends on many factors and cannot be used randomly! Self-treatment for adrenal insufficiency often does more harm than good.
At the same time, with timely diagnosis and an adequate course of therapy, normalization of the patients’ lifestyle is observed. Women with this pathology can easily become pregnant and give birth on their own.
Purpose of the adrenal glands in women
In women, all hormonal changes are especially noticeable, because they quickly appear on the face and body. Disturbances in the endocrine system most often affect the female gender.
The main function of organs is to produce hormones, such as:
- Cortisol and corticosterone. Destroys proteins, promotes obesity, and also increases blood glucose levels. Participate in the body's adaptation after stress.
- Adrenaline and norepinephrine. Affects the heart rate. Increases blood pressure. Accelerates carbohydrate metabolism.
- Aldosterone and dehydroxycorticosterone.
- Estrogens, androgens and progesterone. Affect the formation of secondary sexual characteristics.
- Hormones of protein, lipid and carbohydrate metabolism.
- Reaction to stress.
During pregnancy, a woman experiences enormous hormonal changes in her body, some levels soar several thousand times. This restructuring forces the adrenal glands to work much more intensely, like other organs of the female body.
Progesterone is considered the main female hormone produced during pregnancy; if it is lacking, there can be a risk of pregnancy, so often in the early stages, after receiving laboratory tests, women are prescribed additional progesterone. By the second trimester, the placenta takes over the work of the adrenal glands, and additional hormonal support is no longer required.
If a woman does not have hidden pathologies, after the birth of a child the body independently returns to its normal state.
The female body undergoes hormonal changes not only during pregnancy, but also after the end of childbearing and the onset of menopause. The function of producing estradiol from the ovaries is transferred to the adrenal cortex.
Hormonal disorders
All diseases can be divided into two groups: in which there are not enough hormones or they are not produced, and in which they are in excess.
A lack of hormones in the body or failure to produce hormones is called adrenal insufficiency. There are three degrees of deficiency classified.
Primary failure is characterized by low production of adrenal hormones or the absence of this function, which is inherent in Addison's disease. Addison's disease develops as a consequence of destruction of the adrenal cortex, leading to a decrease in hormone production.
Secondary deficiency occurs when an abnormality already exists in the body. Appears most often due to dysfunction of the pituitary gland and hypothalamus. The disease manifests itself as a primary deficiency, but there is no definite hyperpigmentation. The cause may be head injuries or the presence of brain tumors.
And there is an acute form of failure or Addisonian crisis. This is an extremely dangerous disease and requires urgent hospitalization. Characteristic signs are a sharp decrease in blood pressure, abdominal cramps, diarrhea, loss of consciousness and rare acts of urination.
When excessive production of hormones by the adrenal cortex occurs, the following diseases appear:
- Hyperplasia of the cortex.
- Kohn's syndrome, or hyperaldosteronism.
- Secondary degree of hyperaldosteronism.
- Pheochromocytoma.
Each disease has its own symptoms and causes.
Addison's disease
When the disease occurs, insufficient production of androgens, aldosterone and cortisol occurs; the main distinguishing sign of the disease is changes in the color of the skin; in some places the skin takes on a bronze, tanned color.
With a lack of androgens, hair growth in the bikini area and armpits slows down, and perhaps there will be no hair at all. Lack of androgens disrupts menstruation and leads to infertility.
A lack of cortisol leads to a deterioration in overall health, loss of appetite, and decreased blood pressure. With a lack of aldosterone, the potassium-sodium balance is disrupted, and sodium is washed out of the body. This threatens disruption of the cardiovascular and urinary systems.
Cortical hyperplasia
Cortical hyperplasia can be congenital or acquired; the first type is most common. Hyperplasia also causes enlargement of the adrenal glands, as the tissue of the cortical layer increases.
Symptoms are characterized by an excess of any hormone:
- Hair growth in the groin and armpits, much earlier than peers.
- Height inappropriate for age.
- Body formation in girls according to the male type.
- Acquisition of girls' genitals, outlines of male genitalia.
- Late arrival of menstruation or its absence and infertility.
- Pressure surges.
- Acne on the chest and back.
Conn's syndrome or hyperaldosteronism
Excessive production of aldosterone – hyperaldosteronism, the cause of which may be a benign neoplasm (adenoma). Location of adenoma: zona glomerulosa cortex, Kohn syndrome. The tumor produces the hormone aldosterone, which is responsible for the sodium-potassium balance in the body.
Symptoms that appear with Conn's syndrome:
- Hypokalemia, as a result of which dystrophy of the tubular apparatus of the kidney occurs.
- Changes in the cardiovascular system, constant headaches.
- Decreases in potassium levels in the body, which leads to cramps, anemia, and muscle weakness.
Itsenko-Cushing's disease
Itsenko-Cushing's disease is a disease manifested as a result of disruption of the pituitary gland and hypothalamus, but unlike secondary failure, it manifests itself in the form of an excess of the hormone corticotropin produced by the adrenal cortex. The disease most often affects women of childbearing age.
Symptoms in women are:
- Moon-shaped face.
- Red stretch marks in the abdomen and thighs.
- Rapid obesity.
- Hair loss on the head, but excess hair on the face and body.
- Aches and pains in the bones. Muscle cramps.
In addition to cosmetic signs, disruption of the adrenal glands is manifested in changes in the functioning of the cardiovascular, urinary, reproductive, respiratory and digestive systems. As you can see, the disease affects the entire body, so it is so important to start treatment as early as possible.
Hypercortisolism syndrome
The syndrome is a complex of anomalies caused by a long and constant excess of glucocorticoid hormones. The symptoms are similar to Itsenko-Cushing's disease, but the cause lies not in the pituitary gland, but in the excessive use of hormonal drugs.
Hypercortisolism is classified into primary and secondary. The cause of primary hyperfunction is a neoplasm in the adrenal glands - corticosteroma. Secondary occurs as a consequence of malfunction of the pituitary gland and hypothalamus.
There are 3 clinical pictures of hypercortisolism:
- Subclinical form. The presence of hidden inactive neoplasms.
- Iatrogenic hypercortisolism. Occurs with long-term use of drugs containing corticosteroids.
- Functional. Occurs when aggravated by obesity, diabetes and liver diseases.
In general cases, the syndrome is manifested by symptoms: an increased amount of fat mass in the shoulder girdle and on the face, a hanging pelvis and abdomen (muscle dystrophy), dark purple stretch marks on the body.
Tumors of the adrenal cortex
Most neoplasms of the adrenal cortex are benign tumors. Experts tend to believe that the appearance of tumors is hereditary.
There are several types of tumors:
- aldosteroma;
- glucoadrosteroma;
- corticoestroma;
- pheochromacetoma.
Of all, pheochromacetoma stands out; it is a tumor of the adrenal medulla, which is hormonally active. Pheochromatacetoma produces excess adrenaline, dopamine and norepinephrine, which are responsible for heart rate and blood pressure. The tumor produces hormones spasmodically, and heart rhythm and blood pressure behave accordingly.
There are three types of pheochromacetoma:
- Paroxysmal. Presence of adrenaline crises.
- Constant. Constant high blood pressure. No crises.
- Mixed. Constant pressure and adrenaline crises.
A crisis is a sudden release of one or another hormone into the blood.
Symptoms of pheochromacetoma are:
- Hot flashes, dizziness, sweating, anxiety, panic attacks.
- The skin color is either too pale or too red.
- Sudden jumps in blood pressure.
- Visual impairment.
- Increased outflow of urine.
Diseases of the adrenal glands in women also include a cyst; this is an anechoic formation (not shown on ultrasound, only a white spot is visible) filled with a liquid substance. The main goal is to determine its nature, whether it will eventually develop into a malignant tumor. It is almost impossible to diagnose its appearance if it does not grow, only by chance during a full body scan. If the cyst has begun to grow, then this is not a good sign and surgical intervention will be required.
The main symptoms of a cyst are: increased blood pressure, compression in the abdominal cavity, pain in the waist (anywhere), difficulty urinating.
Adrenal depletion
Modern man lives at a frantic pace, which increases every year, and the entire endocrine system, including the renal gland, has to work at the same dynamics. Constant stress, depression, lack of sleep, malnutrition, all this leads to depletion of the adrenal glands.
Symptoms of such a process will be: chronic fatigue, discomfort in joints and bones, pressure surges, problems in the oral cavity, dry skin and severe hair loss.