Klimova Oksana Yurievna
Endocrinologist, 18 years of practical experience, participant in conferences and congresses on endocrinology. I have more than 10 publications in scientific journals in the field of endocrinology and clinical pharmacology. General medical experience over 20 years.
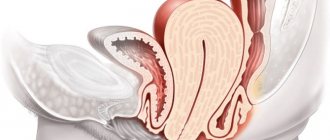
Diffuse toxic goiter (DTZ, Graves-Bazedow disease) is an autoimmune disease characterized by persistent pathological hypersecretion of thyroid hormones and, as a rule, a diffusely enlarged thyroid gland. Goiter is a pathological enlargement of the thyroid gland, without specifying its functional state. The normal volume of the thyroid gland, determined by ultrasound, is 9 - 25 ml in men, 9 - 18 ml in women. Palpation of the thyroid gland, being the main method of clinical examination of the thyroid gland, does not allow determining its volume and has no independent significance for the diagnosis of goiter.
One of the complications of diffuse toxic goiter is thyrotoxicosis, a clinical syndrome caused by persistent pathological hypersecretion of thyroid hormones. The term hyperthyroidism means an increase in the functional activity of the thyroid gland, which can be pathological (thyrotoxicosis) and physiological (for example, during pregnancy).
The severity of thyrotoxicosis is assessed by the clinical picture and the presence of complications associated with the disease (atrial fibrillation, dystrophic changes in internal organs, thyrotoxic psychosis, etc.).
Causes of diffuse toxic goiter
Graves' disease is an autoimmune disease that most often affects women. The risk group includes people aged 30 to 55 years. Diffuse toxic goiter is very rare in children. There are cases of the disease developing in adolescents during puberty. This is due to the fact that the nervous and endocrine systems are being rebuilt, therefore the susceptibility of tissues to thyroid hormones increases.
One of the possible causes is heredity. To date, the pathogenesis of diffuse toxic goiter has not been fully studied, but it has certain causes and provoking factors for the onset of the disease. There are the following reasons for the development of the disease:
- genetic predisposition;
- diseases of the nose and paranasal sinuses. They are divided into: congenital pathologies - dysmorphogenesis, persistence, dystopia;
- diseases of a traumatic nature - closed, open and combined injuries, displacement, deformation of the external parts of the nose;
- infectious diseases – rhinitis, sinusitis (ethmoiditis, sinusitis, sphenoiditis, frontal sinusitis), polyposis;
- penetration of harmful microorganisms through the placenta to the fetus - placentitis;
- diseases of the thyroid gland - nodular goiter, hyperthyroidism, thyrotoxic adenoma, subacute thyroiditis, thyroid cancer;
Graves' disease occurs when antibodies to the TSH (thyroid-stimulating hormone) receptor are produced. Next, the antibodies bind to the receptor, thereby activating it and triggering a number of physiological processes. As a result, thyroid cells begin to actively absorb iodine, secrete and release thyroxine and triiodothyronine into the blood. The cells also multiply quickly. Diffuse toxic goiter in children can develop against the background of diabetes mellitus , Addison's disease, vitiligo, etc.
Provoking factors for the development of the disease
There are some putative provoking factors that can lead to the development of diffuse toxic goiter code E05.0 according to ICD-10 . These include:
- smoking. This bad habit has a negative impact on the entire human body. Smoking increases the likelihood of developing diffuse toxic goiter several times;
- traumatic brain injuries - brain contusion, hematoma, concussion, compression of the brain;
- psycho-emotional stress can be informational and emotional. Typically, these types of stress appear due to strong feelings or information overload;
- heavy physical activity. This may be associated with both sports exercises and professional activities that require the use of physical force;
- hyperthermia – hypothermia of the body. This condition is dangerous because at low body temperature various processes are inhibited: metabolism, blood circulation, heartbeat, oxygen starvation of tissues, etc.
Causes
The main reasons leading to the occurrence of diffuse toxic goiter are the following:
- Autoimmune thyroiditis, which results in immune cells destroying the thyroid gland.
- Genetic predisposition: Most often, the tendency to thyroid diseases is inherited.
- The accumulation of a large number of toxic compounds in the body, and as a result, disruption of the functioning of the endocrine system.
- Stress and psycho-emotional stress.
- Brain damage, traumatic brain injury.
Symptoms of diffuse toxic goiter
The symptoms and causes of diffuse toxic goiter are unique and cannot be compared with any other manifestations. The pathology is characterized by a classic and stable triad of signs:
- hyperthyroidism – excessive production of thyroid hormones;
- Goiter – enlargement in the neck area (see photo above);
- exophthalmos (bulging eyes) – displacement of the eyeballs forward, sometimes to the side.
Since thyroid hormone affects the functioning of various body systems, their excess leads to severe disturbances. Symptoms from the cardiovascular system include:
- arrhythmias - disturbances in the frequency, rhythm and contractions of the heart;
- tachycardia - an increase in heart rate (more than 90 beats per minute). Most typical for grade 2 diffuse toxic goiter;
- arterial hypertension (hypertension) – high blood pressure;
- Extrasystoles are one of the types of arrhythmias. Manifested by untimely contraction and depolarization of the heart or individual chambers;
- significant differences between diastolic and systolic blood pressure;
- chronic heart failure.
Diffuse toxic goiter is characterized by symptoms of endocrine disorders:
- intensive weight loss;
- poor tolerance to high temperature;
- increasing the level of metabolism;
- disruption of the menstrual cycle in women. The occurrence of amenorrhea - the absence of menstruation for a long time - cannot be excluded;
- Men may develop erectile dysfunction (impotence) and decreased libido.
On the skin side, the symptoms are:
- excessive sweating (hyperhidrosis);
- alopecia – baldness and impaired hair growth;
- erythema - severe redness of the skin caused by dilation of capillaries;
- nail damage - dystrophy of the nail plate. The causes may be dermatoses, congenital pathologies, intoxication, etc.;
- pretibial myxedema (swelling of the lower extremities). The cause is a disruption in the production of thyroid hormones.
Clinical symptoms of a neurological nature include:
- severe headaches turning into migraines;
- general malaise;
- tremor of the limbs;
- insomnia or, conversely, severe drowsiness;
- deep tendon reflexes;
- unreasonable anxiety states;
- myopathy is a neuromuscular disease caused by primary muscle lesions.
Symptoms of gastrointestinal disorders:
- rare occurrence of nausea and vomiting;
- constipation;
- diarrhea – frequent bowel movements.
Dental symptoms:
- alveolitis – inflammatory disease of the alveolus of an extracted tooth;
- gingivitis - inflammation of the gums that does not violate the integrity of the connection between the teeth and gums;
- Oral candidiasis (candidal stomatitis) is an infectious disease of the oral cavity that occurs due to the presence of yeast-like fungi of the genus Candida;
- periodontal disease (alveolar pyorrhea) is a pathological condition accompanied by gum damage and atrophy of the alveolar jaw processes. The result is loosening and loss of teeth;
- pericoronitis is an inflammatory process in the soft tissues of the gums that surround erupted teeth.
Ophthalmic symptoms include:
- pain and pain in the eyes;
- involuntary lacrimation;
- ptosis of the upper and lower eyelids - drooping eyelids can partially or completely close the eye;
- lagophthalmos – incomplete closure of the eyelids;
- exophthalmos - bulging eyeballs;
- swelling and proliferation of eye socket tissue;
- visual impairments leading to complete blindness - cataracts, endophthalmitis, glaucoma, keratitis, neuritis, etc.
In severe cases of diffuse toxic goiter, fatty depletion of the liver may develop, which can lead to cirrhosis.
Symptoms
The symptoms that accompany diffuse toxic goiter are observed in all systems of the body, but the greatest threat to the patient’s life comes from disruption of the heart and blood vessels, which leads to heart failure and myocardiostrophy.
In medical practice, the following signs of the disease are distinguished:
- high blood pressure and rapid heartbeat;
- increased sweating;
- nervous excitability, anxiety;
- ophthalmopathy;
- hair loss;
- stomach upsets – diarrhea, constipation, flatulence, light-colored feces;
- increased appetite and, at the same time, rapid weight loss;
- trembling of fingers;
- weakness, fatigue;
- sleep disturbance;
- menstrual irregularities in women;
- decreased libido;
- feeling of squeezing in the neck;
- regular dry cough for no reason;
- difficulty swallowing.
In advanced forms of diffuse toxic goiter, manifestations of ophthalmopathy are possible. In clinical practice, the following symptoms are distinguished:
| Name | Symptom manifestations |
| Kocher | If, when looking down, there is a white stripe of sclera between the iris and the eyelid. |
| Graefe | If, when looking up, the sclera is visible between the iris and the upper eyelid. |
| Stellvaga | The person rarely blinks. |
| Moebius | It is difficult or impossible to fix your gaze on an object that is close to your eyes. |
| Rosenbach | Trembling of the eyelids with closed eyes. |
Classification of diffuse toxic goiter
Diffuse toxic goiter can be divided into forms and degrees. Graves' disease manifests itself in certain forms of thyrotoxicosis, regardless of the size of the thyroid gland:
- light form. Complaints of a neurotic nature predominate, but the heart rhythm is not disturbed. Tachycardia is possible with a heart rate (HR) of no more than 100 beats per minute. There are no pathological disturbances in the functioning of other glands of the endocrine system;
- medium shape. Weight loss of up to 9 kg per month occurs, tachycardia appears with a heart rate of more than 100 beats per minute;
- severe form. There is a loss of body weight, leading to exhaustion of the body, functional disorders of the heart, liver and kidneys appear. More often it occurs due to the lack of treatment of diffuse toxic goiter of the thyroid gland.
In addition to the forms, there are degrees of Basedow’s disease:
- First degree . Diffuse toxic goiter of the 1st degree is characterized by low physical activity, weight loss within 17%. Hyperhidrosis (sweating) and pronounced pigmentation of the skin are noted. There is no enlargement of the thyroid gland;
- Second degree . With diffuse toxic goiter of grade 2, the patient’s nervous excitability increases, symptoms of heart rhythm disturbances increase, and physical activity decreases. Signs of impaired functioning of the circulatory system may appear - circulatory failure. An enlarged thyroid gland is not noticeable externally, but can be detected by palpation. In the evening, swelling of the lower extremities may appear;
- Third degree . It is considered the most severe, since the symptoms of hyperthyroidism increase and a person’s ability to work decreases. Atrial fibrillation and heart failure occur. The muscular system also weakens and motor functions are impaired. An enlarged goiter is very noticeable in appearance. Visual impairment, even blindness, cannot be ruled out.
There are also 5 stages of thyroid enlargement:
- It is impossible to visually determine the thyroid gland (the shape of the neck is not deformed), but palpation can reveal one or two-sided enlargement of its lobes;
- The gland is visually highlighted when swallowing and enlarged lobes are easily palpable;
- An enlarged gland can change the structure of the anterior region of the neck (the neck thickens);
- A greatly enlarged thyroid gland protrudes on the front surface of the neck, thereby deforming it;
- The gland grows to a gigantic size - several tens of centimeters in diameter.
Features in children and the elderly
If Graves' disease develops in a child under 4 years of age, the growth of his skeleton and psychomotor development are disrupted. The child is increasingly noticeably behind his peers in intelligence and precision of movements, which is especially noticeable during small work such as drawing.
More often, the disease is observed in children over 10 years of age, and then the symptoms correspond to those in adults. However, children almost never develop heart attacks and strokes, unless, of course, there is concomitant pathology. There are often cases when nervousness in Graves' disease is mistaken for “adulthood”, and hand tremors are mistaken for malingering. In this case, an enlarged thyroid gland becomes a symptom of paramount importance. A timely test for thyroid hormones and antibodies will allow an earlier diagnosis.
By the way, we recommend reading the article The main causes and symptoms of myxedema
Graves' disease is also dangerous in the elderly: heart problems are common at this age, and hypothyroidism only aggravates them. Elderly people are also characterized by a very moderate enlargement of the thyroid gland; its size may not change at all.
Sometimes the disease instead of excitement manifests itself as apathy. The combination of this symptom with progressive weight loss up to cachexia, lethargy and emotional inhibition threatens rapid death.
Diagnostics
To make an accurate diagnosis, the doctor does not need the patient’s complaints alone. To confirm the presence of pathology, laboratory blood tests are performed. With obvious symptoms of endocrine ophthalmopathy, the diagnosis of diffuse toxic goiter is almost obvious.
If Bazedova's thyroid disease is suspected, the level of thyroid hormones - T3, T4, pituitary thyroid-stimulating hormone and free fractions of hormones in the blood - must be determined . It is necessary to distinguish diffuse toxic goiter from other diseases that are also accompanied by thyrotoxicosis.
Diagnosis of diffuse toxic goiter involves the following methods:
- Enzyme-linked immunosorbent assay (ELISA) helps determine circulating antibodies to thyroglobulin, thyroid-stimulating hormone receptors and thyroid peroxidase;
- Ultrasound examination of the thyroid gland helps to determine the enlargement of the gland and the presence of a hypoechoic formation, which is characteristic of autoimmune pathologies;
- Scintigraphy of the thyroid gland makes it possible to identify functionally active gland tissue, see the volume, shape and presence of nodular neoplasms. If the patient has symptoms of endocrine ophthalmopathy and thyrotoxicosis, then scintigraphy is not mandatory;
- reflexometry is an indirect method for determining the functioning of the thyroid gland. The basis is the measurement of the strength of the stimulus, which is necessary for the appearance of reflexes.
Only after all studies have been completed, treatment is prescribed.
Treatment with radioactive iodine
Radioactive iodine treatment is a way to remove the thyroid gland without surgery. The procedure uses iodine-131, which is consumed once and destroys gland cells over a period of 8 days to 2 months.
Who is prescribed radioactive iodine therapy:
- Patients with relapse of thyrotoxicosis after treatment with tyrosol.
- People diagnosed with thyroid cancer after surgery to remove the organ. Radioactive treatment is used to eliminate remnants of the gland.
There are contraindications to radioactive treatment. This procedure cannot be performed during pregnancy or breastfeeding, since radioactive iodine can harm the fetus and also pass into breast milk.
The advantages of using radioactive iodine for diffuse toxic goiter are obvious: no anesthesia or medical intervention is required, there is no need to undergo rehabilitation after the procedure, and there are no scars on the neck.
Although the use of radioactive iodine-131 is an effective treatment, there are serious consequences of the procedure:
- You cannot plan a pregnancy earlier than six months after the procedure, since radioactive iodine accumulates in the ovaries and mammary gland in women, and in the testicles in men;
- after the procedure, the patient is in complete isolation for 3 days, since his body emits harmful radioactive waves during this time;
- subsequently the patient develops hypothyroidism - a lack of hormones that requires constant treatment;
- the possibility of developing malignant tumors increases, in particular, tumors can appear in the small intestine;
- autoimmune ophthalmopathy may develop;
- in the first time after the procedure, chronic diseases worsen;
- rapid weight gain is possible;
- sialadenitis is a painful inflammation of the salivary glands.
Treatment of diffuse toxic goiter
Conservative methods of treating toxic goiter of the thyroid gland involve taking antithyroid medications. The drugs can accumulate in the gland and have a suppressive effect on the production of thyroid hormones.
Radioactive iodine therapy (radiiodine therapy) is one of the methods of treating thyrotoxicosis and diffuse toxic goiter. The isotope (I 131) accumulates in the cells of the thyroid gland, after which it disintegrates, locally irradiating and destroying thyrocytes. This method is considered quite effective, non-invasive and affordable. The therapy does not cause any complications, unlike surgery on the gland. The only contraindications for radioiodine therapy are breastfeeding and pregnancy. Radioactive iodine therapy requires mandatory hospitalization.
If diffuse toxic goiter is detected in a pregnant woman, then not only a gynecologist, but also an endocrinologist should monitor the entire period of gestation. Treatment involves taking propylthiouracil in a small dose, which is necessary to maintain the concentration of free thyroxine. This drug does not penetrate the placenta well, so it is considered safe in the early stages.
Over time, the need for thyreostatics decreases, and many women do not take the drug after the 25th week of pregnancy. 6 months after birth, a relapse of thyrotoxicosis may develop.
As for the treatment of thyrotoxic crisis, intensive treatment is used using large doses of thyreostatics. If self-administration of certain medications is not possible, they are administered using a nasogastric tube. Thanks to combination therapy, the patient's condition improves.
Drug treatment
Conservative treatment uses a large number of drugs of various types and groups. Drugs for the treatment of diffuse toxic goiter and thyrotoxicosis are as follows:
- antithyroid drugs - Thiamazole, Iodine, Potassium iodide, Metizol, Propicil. For the treatment of diffuse toxic goiter in children, Iodine Vitrum is used, in the form of chewable tablets;
- glucocorticoids - Lemod, Medrol, Polcortolon, Dexazone, Kenacort, Prednisolone;
- beta-blockers - Atenolol, Pindolol, Bisoprolol, Esmolol, Sotalol, Betaxolol;
- detoxification drugs - Agri, Milife, Metadoxil, Ringer Lactate, Ringer.
Surgical intervention
Surgical treatment involves almost complete removal of the thyroid gland (thyroidectomy), after which postoperative hypothyroidism begins. You can compensate for the lack of thyroid hormones with the help of medications that can prevent relapses of the disease. The main clinical recommendations for the operation are:
- severe allergic reactions to certain medications;
- persistently low level of leukocytes in the blood during conservative treatment;
- diffuse nodular toxic goiter is too large in size;
- disorders of the cardiovascular system;
- pronounced endemic effect.
Surgery is possible only after diagnostics and hormonal compensation with the help of medications. Thyroidectomy is performed under general anesthesia. Local anesthesia is used to avoid damage to the recurrent nerves.
Drug treatment
Drug treatment of the disease is the most common way to combat diffuse toxic goiter, which uses thyreostatics, beta-blockers and, if necessary, clucocorticosteroids.
Thyreostatics
Thyreostatics are drugs that inhibit the enzyme iodide peroxidase, which is involved in the production of thyroid hormones. There are several groups of thyreostatic drugs: tyrosol, propicil, mercazolil, thiamazole.
The first phase of treatment lasts a month. At this stage, using a large dosage of the drug, a normal amount of T4 and T3 in the blood is achieved.
The second stage of treatment with thyreostatics lasts up to a year, while the dose is reduced in order to maintain the achieved result.
Beta blockers
Beta blockers (adrenergic blockers) are drugs that eliminate symptoms of the cardiovascular system: reduce heartbeat, increased anxiety, lower blood pressure and eliminate tachycardia.
Beta blockers are prescribed only at the first stage of treatment. After normalization of hormone levels, the need for adrenergic blockers disappears.
Glucocorticosteroids
Glucocorticosteroids are prescribed only in the presence of autoimmune ophthalmopathy, which may accompany diffuse toxic goiter.
Side effects during the treatment of diffuse toxic goiter can manifest themselves as follows:
- allergic reactions to drugs and their components;
- disruption of the gastrointestinal tract, which is accompanied by diarrhea, constipation, flatulence, abdominal pain;
- women experience menstrual irregularities;
- liver function is impaired.
After the end of drug therapy, a high percentage of relapse and the appearance of thyrotoxicosis is approximately 75%.
Alternative home treatments
Treatment for Graves' thyroid disease at home is acceptable, but self-medication may be ineffective and even life-threatening. Before starting treatment at home, in any case, it is necessary to undergo a full range of examinations and strictly follow the clinical recommendations of the attending physician.
Nutrition
Due to diffuse toxic goiter, the human body very quickly loses the necessary reserves of phosphorus, carbohydrates, potassium, adipose tissue, calcium and other essential components. With this disease, there is a clear change in metabolism, so the body requires the supply of nutrients. The diet of patients should be enhanced. The diet is prepared individually by a nutritionist. A balanced increase in all the main nutrients - proteins, carbohydrates and fats - is necessary.
The list of the most useful foods for diffuse toxic goiter includes: sea fish, dairy products, liver, seafood, vegetables and fruits. It is also necessary to take a special complex of vitamins. Due to the pathology, a person experiences excessive excitability of the central nervous system, so it is necessary to avoid strong broths, tea, coffee, etc. Products that can be eaten by patients include:
- rice, buckwheat and oatmeal;
- vegetables: boiled potatoes, carrots, tomatoes, onions, garlic;
- Meat and fish are best consumed boiled or stewed. It is necessary to choose low-fat varieties of meat: chicken, rabbit, nutria, veal;
- chicken egg yolks;
- berries and fruits: strawberries, citrus fruits, wild strawberries, apples, pineapples, bananas.
These products will help strengthen the body, muscle tissue, improve the functioning of the heart muscle and replenish the amount of glycogen in the liver.
If you have Graves' disease, you should not eat the following foods:
- baked goods made from white flour;
- sugar;
- strong tea and coffee;
- alcohol;
- semi-finished products, canned food;
- highly carbonated drinks;
- peas, beans, beans, lentils;
- radishes, beets;
- mushrooms.
All of the above products irritate the intestinal mucosa, which greatly interferes with the functioning of the stomach. You should also completely stop smoking.
Meals should be divided into five times a day, portions should not be large.
Folk remedies
It is possible to cure diffuse toxic goiter using traditional methods, but everything must be agreed with the attending physician. To treat diseases with folk remedies, the following recipes are used:
- White bloodroot. Pour 10 grams of dry plant with a glass of boiling water and leave to infuse in a thermos overnight. Drink half a glass of the decoction three times a day 30 minutes before meals. Gradually the dosage should increase to a full glass. The course of treatment is 10 months;
- Motherwort tincture. Helps calm the central nervous system. You can buy the remedy at the pharmacy, but you can also make it at home: pour 15 grams of dry motherwort leaves into a glass of boiling water. Leave to infuse for 15 minutes, squeeze, filter and take 1 tablespoon three times a day.
- Walnuts. Pour 300 grams of walnut partitions with 1 liter of alcohol (60%). Place in a dark place for two weeks. Filter the infusion and drink a teaspoon three times a day 20 minutes before meals. The course is 3 weeks;
- A decoction of cocklebur. Pour 2 tablespoons of the herb into 500 ml of boiling water and leave to steep for 30 minutes. Then filter and take 1 tablespoon 6 times a day;
- Sea kale powder. Take three times a day 25 minutes before meals. Course duration is 1 month.
Physical exercise
Basedow's thyroid disease damages bone strength. To support the musculoskeletal system, special physical exercises are recommended. Heavy and sudden physical activity should be avoided. Yoga and meditation are best. Under no circumstances should you take hydrogen sulfide, sun or sea baths.
Etiology of Graves' disease
The cause of the disease is autoimmune disorders. These disorders occur when the immune system begins to attack the thyroid gland with antibodies, as if it were foreign tissue. Why this happens is still not known. There are theories that this is due to viruses, radioactive iodine, and genetic predisposition also plays a big role, since this disease occurs among close relatives. The disease often occurs in people with other diseases of the endocrine system: diabetes mellitus, Addison's disease, hypoparathyroidism.
Prevention
To prevent the disease, it is necessary to determine the level of platelets and leukocytes once a month. To prevent severe forms of the disease, clinical observation in the clinic is recommended. If left untreated, a severe complication of Basedow's disease may develop - thyrotoxic crisis or coma . This complication can be fatal.
One of the preventive measures is to carry out general strengthening therapy and sanitation of inflammatory foci - the elimination of all possible infections. The patient should maintain a hygienic regime, combat stress and lead a healthy lifestyle.
Clinical symptoms
There are a lot of signs. Some of them relate to general symptoms, that is, those that may accompany diseases of other systems (fatigue, nervousness, weight loss). And some occur only with Graves' disease (a combination of goiter and exophthalmos). They are all divided into several groups:
- Symptoms associated with heart damage. Thyroid hormones (thyroxine, triiodothyronine) cause the heart to beat faster (tachycardia), which causes the organ to fail. This is manifested by the appearance of arrhythmia, extrasystole, and hypertension.
- Signs of endocrine disorders: adaptation disorder, heat intolerance, sudden weight loss.
- When a person gets sick, sweating increases, nails and hair become brittle, and there may be swelling in the lower leg area.
- The human nervous system is disrupted. Such patients quickly get tired, feel weakness, and unobtrusive muscle pain. In addition, they are very irritable and whiny. Their sleep is disturbed and their mood often changes.
- During the disease, the digestive tract also suffers, as a result of active work of the stomach and intestines. This is manifested by diarrhea, nausea, and vomiting.
- Ophthalmological disorders in the form of exophthalmos: protruding eyes, pronounced shine, swelling of the soft tissues around them, rare blinking, incomplete closure of the eyelids. This threatens inflammation, drying out and complete blindness. If other pathological conditions arose as a result of the excessive influence of thyroid hormones, then ophthalmopathy was due to a direct attack by antibodies.
More about pathology
Graves' disease of the thyroid gland is of an autoimmune nature. It is characterized by rapid cell proliferation and excessive production of glandula thyreoidea hormones, leading to thyrotoxicosis, which is systemic in nature.
It has several names:
- hyperthyroidism;
- Perry's disease;
- Flajani's disease;
- Graves' disease;
- diffuse toxic goiter.
Graves' disease more often affects representatives of the weaker than the stronger sex; middle-aged people are also at risk, but young people and old people are much less susceptible to this pathology. The incidence of the disease in the human population is about one percent, it confidently ranks second after hypothyroidism.
Usually there is a clear connection between the onset of the disease and the insufficient supply of iodine ions in the body.
Interesting! The pathology is genetically determined and is transmitted, in the vast majority of cases, through a generation through the female line - to the granddaughter from the grandmother.
What diseases can it be associated with?
Graves' disease is often detected against the background of other endocrine diseases or periods of hormonal changes.
The detection of a nodular formation in the thyroid gland in a patient with thyrotoxicosis does not exclude Graves' disease. In some cases, diffuse functional autonomy of the thyroid gland occurs without the formation of nodules. In this case, scintigraphy plays the main role in differential diagnosis (with functional autonomy, “hot” nodes and/or uneven increases in isotope uptake are detected). Typically, Graves' disease develops in the older age group of patients; there is no endocrine ophthalmopathy and no antibodies to the thyroid gland.
Subacute thyroiditis is characterized by an acute onset, pain in the neck radiating to the back of the head and ears, severe thyroid tenderness, low-grade fever, increased ESR (erythrocyte sedimentation rate), lymphocytosis, decreased isotope uptake during scintigraphy and rapid response to glucocorticoid therapy
With painless (“silent”) thyroiditis, symptoms of thyrotoxicosis are rarely observed, and with hormonal studies, subclinical thyretoxicosis is diagnosed. The scintigraphy data shows a decrease in isotope uptake.
Pregnancy - the content of free fractions of thyroid hormones is within physiological values, the content of total fractions is naturally increased. The use of thyreostatics is excluded.
Postpartum thyroiditis is a type of painless thyroiditis that occurs in the first 6 months after childbirth and is the most common cause of thyroidopathy in the postpartum period.
Stages of the disease
Graves' disease, the symptoms and causes of which were discussed above, is divided into three stages:
- Light.
- Average.
- Heavy.
The criteria for dividing the disease into stages are given in the following table:
| Criteria | Stage I | Stage II | Stage III |
| General state | Does not change | Average | Heavy |
| Body mass | Reduction by 1/10 | Reduction from 1/10 to 1/5 | Reduction of more than 1/5 |
| Heart rate | Less than or equal to 100 beats/min | More than 100 beats/min | More than 120 beats/min |
| Arterial pressure | Increased | Increased | Increased |
| Other organs | Without changes | Without changes | Damage to other organs |
Determining the stage is necessary so that the doctor can more accurately prescribe treatment. As for the complications of Graves' disease, the most dangerous of them is thyrotoxic crisis, which requires emergency care.
Complications
With diffuse goiter (Graves disease), the following complications often develop:
- atrial fibrillation;
- atrial fibrillation;
- arterial hypertension;
- cachexia;
- heart failure;
- decreased vision;
- ophthalmopathy;
- hepatitis;
- hepatosis;
- depression;
- hypokalemia (low potassium levels in the blood);
- paralysis;
- crisis
Complications more often occur with diffuse severe goiter and irregular medication use.
Treatment
There are different approaches to therapy, depending on the stage of the disease, concomitant diseases, age and other factors. There are:
- Drug therapy;
- Surgery;
- Radioactive iodine therapy.
Drug therapy
Thyreostatics are used as etiological therapy. These are drugs that prevent the thyroid gland from taking up iodine. Without it, hormone synthesis will not occur. On the domestic market, among the thyreostatics you can find tyrosol, mercazolil and others. Which drug is better to choose and the course of treatment is prescribed by the treating endocrinologist. The prognosis for such treatment varies for patients. In some cases they recover, but in others the disease progresses and they have to turn to other treatment methods.
In addition, if a person has complications, sedatives, antiarrhythmics, antiemetics and other drugs are prescribed as pathogenetic treatment.
Vitamins and minerals are prescribed as symptomatic therapy.
Surgery
If pharmacotherapy is ineffective, part of the gland is removed, leaving up to 3 mm of organ tissue. Gentle, organ-preserving surgery, in most cases, causes a relapse. After surgery, drug therapy does not stop, because resection of the gland does not eliminate the disease itself. Not all people can have surgery. Contraindications:
- Liver damage in the acute period;
- Severe form of the disease;
- Severe concomitant pathologies of other organs;
- Elderly age.
Surgical treatment of Graves' disease is not always successful. In addition, there are a number of complications. The most difficult thing is a thyrotoxic crisis. If the preparation or the operation itself is not carried out correctly, a sharp drop in T3 and T4 causes the pituitary gland to produce a lot of TSH. This increases the level of thyroid hormones to a life-threatening state.
A person’s temperature rises, blood pressure and pulse increase, loss of consciousness and other nervous system disorders.
Such a crisis is treated in the intensive care unit on the principles of critical illness.
Radioactive iodine therapy
The treatment method for Graves' disease involves injecting radioactive iodine into the body, which will damage gland cells, preventing the production of hormones. It is prescribed when pharmacotherapy is ineffective and there are contraindications to surgery.
This procedure is prohibited for children, pregnant and nursing mothers. It is mainly used for older people. The course of treatment includes a diet with a low intake of iodine-containing foods.
Treatment during pregnancy
Since pregnancy is a special period for a woman, it needs to be treated in a special way. Firstly, combination therapy cannot be prescribed, only one drug. The dose should be minimal so that the hormones T3 and T4 are at the upper limit of normal. You need to choose a drug so that it does not pass through the placenta into the baby’s bloodstream. When the effect of treatment is achieved, you need to see a doctor every week.
Causes of Basedow's disease
Basedow's disease is an autoimmune disease , due to the fact that the immune system attacks its own body. The reason for this phenomenon is the negative effect of antibodies on the thyroid gland receptors responsible for thyroid-stimulating hormone (TSH, thyrotropin, thyrotropin), which is produced by the pituitary gland and which stimulates the thyroid gland.
When thyroid-stimulating hormone binds to thyroid receptors, the antibodies cause hyperactivity of this endocrine organ.
Physical and mental stress play a very important role in the occurrence of this disease. Any major life event (change of job, change in family) can contribute to the onset of Graves' disease.
Complications and prognosis
The outcome of treatment for toxic goiter will vary significantly in each case. Therapy, started correctly and on time, will help quickly eliminate the hormonal fire and maintain the functionality of internal organs. Long-term toxicosis will lead to fairly rapid destruction of the heart muscle. The result will be disability and an unfavorable outcome. Predicting the behavior of toxic exophthalmos is even more difficult. Often these changes persist for life, despite proper X-ray exposure.
X-rays are used to treat exophthalmos
Thyrotoxic crisis is a dangerous complication of thyrotoxicosis. This condition is caused by a sudden jump in hormone levels in the blood. This situation may develop in the coming hours after surgery. The crisis is manifested by high fever and rapid pulse. If left untreated, the crisis progresses to a coma. This situation requires urgent specialist intervention and therapy in an intensive care unit. DTG is often complicated by relapse.
Graves' disease: symptoms
At the initial stage of the disease, there are no symptomatic manifestations. It is worth considering that the symptoms of the pathology differ from person to person and may vary. It all depends on:
- immune response;
- characteristics of the body;
- depending on the severity of the disease.
That is why it is quite difficult for a specialist to quickly make a diagnosis.
Initially, a person may complain about:
- excessive sweating,
- unstable mental state (increased nervousness, mood swings),
- sleep disorders,
- attacks of increased heart rate,
- trembling in the limbs.
Over time, a person loses weight, because... rapidly losing weight even with a standard diet and appetite.
If a person has Graves' disease, he does not tolerate high temperatures well, even in the cold he feels hot.
With the further development of the pathology, the symptoms only intensify. Trembling may spread throughout the entire body. The patient begins to behave nervously, fussily, the skin is often moist. The skin becomes darker, yellowness appears in the eyelid area.
Sometimes there is swelling (of the feet, legs), which looks like a thickening. On palpation, pain and density of the formations are noted.
But the most characteristic symptom can be called changes in the eyes. They become shiny and wide open (Dalrymple syndrome). The eyeballs are rounded, enlarged and become bulging. The eyelids are swollen.
Pathogenesis
The causes of Graves' disease are:
- heredity. Patients often have a genetic predisposition to the disease (due to the activity of thyroid-stimulating antibodies). Their hormone mimicry allows them to increase the synthesis as well as the secretion of thyroid-type hormones. The human body produces antibodies as a result of the presence of suppressors, which are also called irregular T-lymphocytes. It is they, instead of establishing control over the immune system, that begin to destroy the thyroid gland. The formed antibodies enlarge the thyroid gland and also inhibit apoptosis, which is the cause of hyperplasia;
- stressful situations. Diffuse toxic goiter can be caused by psychological trauma, which serves as a trigger for Graves' disease. Stress can trigger many different reactions, including an increase in the amount of secretion from the adrenal cortex. Increased synthesis in the adrenal glands increases the production of thyroid hormones. In addition, stress itself can cause changes in the immune system;
- viral diseases. It is the viruses that enter the body that cause a weakening of the immune system, which, in turn, helps to increase the synthesis of hormones that affect Graves' disease. In addition, antiviral drugs that a person can take uncontrollably (Interferon, Amiksin) increase the likelihood that diffuse toxic goiter will appear. This is explained by their active effect directly on thyroid cells;
- excess iodine. The more iodine a person consumes through food and medications, the more active the autoimmune process is. Iodine itself also stimulates the synthesis of thyroid hormones.
Too much thyroid hormone disrupts the functioning of not only the thyroid gland, but also other systems and organs: increased metabolism is observed and thermogenesis is disrupted. Diffuse toxic goiter hits the heart, blood vessels and brain the hardest.
Diffuse toxic goiter causes the thyroid tissue to grow and the production of the hormones T3 (triiodothyronine) and T4 (thyroxine) to increase. Graves' disease got its name due to the similarity of an enlarged thyroid gland to goiter in animals. An increase in the amount of hormones contributes to the depletion of the human body, causing disruption of systems and organs. Scientists have found that the risk of contracting this disease increases by 2 times if a person smokes.
Surgical treatment - thyroidectomy
Surgical treatment of Graves' disease in our country is included in compulsory medical insurance and is provided free of charge upon referral from the clinic.
During surgery, doctors remove the entire thyroid gland or may leave very small areas of the thyroid gland, but these have little effect on further treatment.
It is important that the thyroid gland is removed completely, and not half. This is due to the fact that as long as there is a main target for AT-rTSH in the body, there is a possibility of re-development of thyrotoxicosis.
Indications for removal of the thyroid gland are:
- Intolerance to thyreostatic drugs (allergic reactions, complications);
- Failure to take antithyroid drugs as recommended by your doctor;
- Moderate and severe eye damage;
- Large thyroid gland (more than 40 ml);
- The presence of nodular formations suspicious for oncological pathology;
- Refusal or inability to undergo radioiodine therapy.
Complete surgical removal of the thyroid gland is the most reliable method, which allows not only to quickly recover from thyrotoxicosis, but also to avoid its relapse.
Most often, after surgery, an almost invisible scar remains like this.
The disadvantages of this type of treatment are possible complications:
- Removal of the parathyroid glands along with the thyroid gland.
This will lead to the development of hypoparathyroidism. A condition in which the body does not absorb calcium. But today this condition is easily treated and taking special medications will make you feel good.
- Damage to the recurrent laryngeal nerve.
This can cause voice changes, hoarseness, and decreased volume. Therefore, for people whose life is connected with singing, if Graves' disease develops, I would first recommend treatment with radioactive iodine.
- Bleeding during surgery.
But don’t worry, the average rate of complications during surgical removal of the thyroid gland does not exceed 3% [2, 3].
What to do after removal of the thyroid gland?
If during the operation your entire thyroid gland was removed, and you were prepared for the operation so that the levels of T4 and T3 were within normal limits, then the next day after the operation you need to start taking levothyroxine (L-thyroxine, Eutirox).
After removal of the thyroid gland, it is very important to take levothyroxine medications daily and for life!
At first, you will need to work closely with an endocrinologist in order to select the optimal dose of the drug that is right for you.
Further, when the dose of levothyroxine is selected correctly, you, with the exception of the need to take one tablet every morning, will feel like a full-fledged person for whom there are practically no restrictions.
Graves' disease: modern approaches to treatment
Graves' disease (diffuse toxic goiter) is one of the most common diseases of the thyroid gland. The article discusses the etiology, pathogenesis and clinical picture of the disease, as well as methods of its diagnosis and treatment. Currently, laboratory diagnosis of thyrotoxicosis is based on clinical symptoms, increased concentrations of free thyroxine, triiodothyronine and undetectable levels of thyroid-stimulating hormone. To treat Graves' disease, medical and surgical methods, as well as radioiodine therapy, are used.
Table 1. Types of thyrotoxicosis and their causes
Table 2. Effect of excess thyroid hormones on the body
Table 3. Classification of thyrotoxicosis
Table 4. Clinical forms of hyperthyroidism
Table 5. Differential diagnosis of thyrotoxicosis
Table 6. Drug treatment for Graves' disease
Table 7. Mechanism of action of the main groups of drugs used in the treatment of Graves' disease
Table 8. Advantages and disadvantages of treatments for Graves' disease
Introduction
Diseases of the thyroid gland (TG) affect all metabolic processes. It is no coincidence that their presence is associated with serious changes in many body systems, worsening the prognosis and quality of life of patients [1, 2]. That is why it is extremely important to know the clinical manifestations of thyroid pathologies, the principles of their diagnosis and treatment methods.
We have to admit that there is still terminological confusion regarding thyroid diseases. In the literature, two terms are used to refer to them – “thyrotoxicosis” and “hyperthyroidism”. However, these concepts are not identical. In particular, hyperthyroidism is one of the common causes of thyrotoxicosis.
Hyperthyroidism should be understood as a condition caused by both excessive synthesis and excessive secretion of thyroid hormones (thyroxine (T4) and triiodothyronine (T3)). It can be considered as hyperfunction of the thyroid gland, for example, in diffuse toxic goiter (DTZ).
With thyrotoxicosis, thyroid hyperfunction is not always observed. This pathology may be caused by inflammatory processes in the thyroid gland, accompanied by destruction of follicles and the release of ready reserves of thyroid hormones. This variant develops in subacute (de Quervain's thyroiditis), postpartum, painless and cytokine-induced thyroiditis, the thyrotoxic phase of chronic autoimmune thyroiditis, as well as in amiodarone-induced thyrotoxicosis type 2. Overdose of drugs containing thyroid hormones (in particular, suppressive therapy) leads to the development of artificial forms of thyrotoxicosis (Table 1).
Diagnosis of thyrotoxicosis is based on clinical symptoms, increased concentrations of free T4 and T3 (free T4 and free T3) and an undetectable level of thyroid-stimulating hormone (TSH). In the case of a low level of TSH and an increase in at least one of the fractions of thyroid hormones, a diagnosis of “manifest thyrotoxicosis” is established; if both fractions are within normal limits, the diagnosis is “subclinical thyrotoxicosis.” The next stage of diagnosis is the search for the etiological factor - the trigger of the disease. Differential diagnosis of thyrotoxicosis involves the determination of antibodies to thyroid-stimulating hormone receptors (AT-rTSH). Of the instrumental methods, the simplest and most informative is considered to be ultrasound examination, which allows one to accurately determine the volume of the thyroid gland, the echogenicity of its structure, the presence of nodes and characteristics of blood flow, as well as thyroid scintigraphy with 131I or 99mTc, reflecting the functional activity of the thyroid tissue [3, 4 ].
Graves' disease
Thyrotoxicosis is the main manifestation of Graves' disease, also known as thyrotoxicosis.
Graves' disease is a systemic autoimmune disease that develops as a result of the production of AT-rTSH (immunoglobulin (Ig) G) and is clinically manifested by damage to the thyroid gland with the development of thyrotoxicosis syndrome in combination with extrathyroid pathology (ophthalmopathy, pretibial myxedema, acropathy, damage to the cardiovascular system, etc. .) [2, 5]. Pathology develops more often in women than in men. Thus, the ratio of women to men with Graves' disease varies from 5:1 to 10:1 [6].
Etiology and pathogenesis
The development of Graves' disease is associated with a congenital defect of specific T lymphocytes. Due to the breakdown of immunological tolerance, B-lymphocytes are activated, producing thyroid-stimulating immunoglobulins - AT-rTSH. The binding of stimulating antibodies to the TSH receptor leads to its activation. As a result, the production of hormones by thyrocytes increases and clinical manifestations of thyrotoxicosis develop [7, 8]. Unlike most other autoimmune diseases of the endocrine glands (type 1 diabetes, hypocortisolism), Graves' disease does not involve destruction, but stimulation of the target organ (hyperthyroidism). T4 remains the main secretory product of the thyroid gland, but the T3/T4 ratio often increases. As the production of thyroid hormones increases, their free fractions increase [9, 10].
Inherited impairment of immunological tolerance may contribute to the survival and proliferation of individual lymphocytes responsible for the autoimmune reaction against thyrocytes, as well as their secretion of IgG in response to environmental factors. Among the trigger factors, the role of viral infection, stress, and smoking is discussed. In particular, emotional stress leads to increased secretion of cortisol, while the activity of T-lymphocytes is suppressed. As a result, autoreactive lymphocytes are freed from their suppressor influence and can fully exhibit their activity. We are talking, in particular, about the synthesis and production of thyroid-stimulating immunoglobulins. Smoking almost doubles the risk of developing the disease [11].
Graves' disease is often associated with other autoimmune pathologies, such as pernicious anemia, alopecia, vitiligo, myasthenia gravis, and idiopathic thrombocytopenic purpura.
Symptoms of thyrotoxicosis
With thyrotoxicosis, changes occur in almost all types of metabolism, but the most pronounced are disorders of fat metabolism. This affects the work of many systems and organs, primarily the cardiovascular, digestive and other endocrine glands in addition to the thyroid gland (Table 2).
Symptoms of the disease develop and progress quite quickly [12].
Patients with thyrotoxicosis are often observed by doctors of other specialties - cardiologists, internists, gastroenterologists and neurologists; they are referred to endocrinologists only when a detailed clinical picture appears. Thus, in elderly people, symptoms of the disease are often regarded as cardiovascular or oncological pathology.
It has been established that an excess of thyroid hormones disrupts the coupling of oxidation and phosphorylation processes at the level of tissue respiration. As a result, heat production increases. Increased heat transfer is achieved due to increased sweating, which is expressed by certain clinical symptoms of the skin (becoming soft, moist and velvety). Therefore, in most patients with DTG, the temperature remains normal. Subcutaneous fat progressively decreases in all parts of the body, depending on the severity of thyrotoxicosis.
Accelerated metabolism is associated with increased oxygen consumption by various organs and tissues, which is achieved by accelerating blood circulation.
Persistent tachycardia, independent of physical activity, is considered one of the main symptoms of thyrotoxicosis. The second cause of tachycardia is the direct effect of thyroxine on the heart muscle [13].
Thyrotoxic tachycardia has the following features:
- shortening of diastole, as a result of which the lack of oxygen in the myocardium worsens;
- increase in total energy consumption per unit time;
- increased risk of developing ectopic impulses, which leads to heart rhythm disturbances and, over time, to cardiovascular failure.
Most often, with DTG, atrial fibrillation develops. This symptom is so pathognomonic that it may be the basis for examining the patient for thyrotoxicosis.
Circulatory failure in thyrotoxicosis has a number of features. It develops according to the right ventricular type, accelerated blood flow and increased cardiac index remain. With thyrotoxicosis, myocardial infarction rarely occurs, which is obviously associated with a lower risk of developing atherosclerosis and adaptation of the myocardium to hypoxia. An increase in heart size is observed only with the appearance of atrial fibrillation and is primarily due to dilatation of the ventricles.
Signs of left ventricular hypertrophy on the electrocardiogram are observed in a third of patients, but are functional in nature (after elimination of thyrotoxicosis, pathological abnormalities disappear).
The classic manifestation of the disease is cardiac arrhythmia - atrial fibrillation, and the frequency of arrhythmia increases with age. Atrial fibrillation is accompanied by an increased risk of thromboembolism [14].
Symptoms from the visual organs are numerous. These include a characteristic fixed, frightened gaze with widening of the palpebral fissures, increased shine of the eyes, rare blinking, Graefe's symptom (when the gaze is fixed on an object slowly moving downwards, a white strip of sclera remains between the upper eyelid and the iris), etc. These manifestations are most likely are caused by increased tone of the sympathetic nervous system and disappear when thyrotoxicosis is compensated.
The most severe pathology complicating the course of Graves' disease is endocrine ophthalmopathy (infiltrative orbitopathy). This is an autoimmune organ-specific disease that occurs with damage to retrobulbar adipose and connective tissues, orbital muscles, optic nerve and periorbital tissues [15].
Inflammatory exudation and infiltration of retrobulbar tissue, as well as extraocular muscles, lead to an increase in intraocular pressure with impaired blood flow in the orbital tissues and a sharp increase in the volume of orbital tissues with the development of exophthalmos [16, 17]. Retrobulbar edema is caused by a significant increase in the production of glycosaminoglycans by orbital tissue fibroblasts. Characteristic signs of the pathology are photophobia, lacrimation, periorbital edema, foreign body sensation in the eyes, and retro-orbital pain. These symptoms include diplopia, swelling of the conjunctiva, and decreased visual acuity. Smoking and poorly controlled thyrotoxicosis significantly worsen the course of endocrine ophthalmopathy.
Excess thyroid hormones also have a toxic effect on liver cells. They activate proteolytic cytoplasms and also promote the formation of SH radicals, which leads to disruption of the cholesterol-synthesizing, glycogen-forming, and detoxification functions of the liver. First, this manifests itself as low cholesterol in the blood, then as a violation of carbohydrate metabolism. As the severity of the disease increases, the level of liver transaminases increases. When thyrotoxicosis is eliminated, all disorders are eliminated [12].
The toxic effect of thyroid hormones on the central nervous system is realized by influencing cells and increasing their sensitivity to adrenaline and norepinephrine. Clinical signs of thyrotoxic encephalopathy include headache, emotional lability, rapid mental exhaustion, inability to concentrate, and sleep disturbances. During treatment with thyreostatics, all changes disappear. In some cases, this can become a differential diagnostic feature [18].
Muscle weakness is especially noticeable when climbing hills or stairs, getting up from your knees, or lifting heavy objects. After normalization of the thyroid status, muscle strength is restored quite quickly, muscle mass takes longer.
Due to insomnia and muscle weakness, such patients often develop a feeling of fatigue.
In patients with thyrotoxicosis, a disturbance of calcium-phosphorus metabolism is also observed. Loss of calcium and phosphorus in urine is significantly increased relative to normal. However, their concentration in blood serum is usually within normal limits. Osteoporosis is more common in older women. The results of numerous studies indicate that excess thyroid hormones have a catabolic effect on bone tissue. Radiological signs resemble menopausal osteoporosis [19].
The reproductive system is also negatively affected by excess thyroid hormones. In men, libido decreases and sometimes gynecomastia develops. Women are characterized by menstrual irregularities, including amenorrhea, and anovulation is possible.
In elderly patients, goiter is often absent or there is a slight increase in the size of the thyroid gland in combination with nodular goiter. The disease is characterized by a mild or oligosymptomatic course [18]. In an atypical course, severe weight loss with symptoms of anorexia may be observed against the background of general and progressive muscle weakness, which raises suspicion of cancer. In elderly patients, cardiovascular disorders often predominate. Therefore, as noted earlier, all patients with newly diagnosed unexplained heart failure or atrial fibrillation should be evaluated for thyrotoxicosis. It should also be remembered that in old age the metabolic manifestations of thyrotoxicosis can be erased, while the clinical picture is often dominated by apathy, lethargy, depression, weakness (apathetic thyrotoxicosis), in other cases - signs of proximal myopathy.
Diagnosis and classification
The diagnosis of Graves' disease, or DTD, is made on the basis of the above clinical symptoms, high levels of thyroid hormones (f. T4, f. T3) and low TSH levels in the blood. An increased titer of AT-rTSH, a marker of immunogenic thyrotoxicosis, serves as evidence that the cause of thyrotoxicosis is Graves' disease. Its persistence during treatment indicates a high risk of disease decompensation [3].
The name of the pathology “diffuse toxic goiter” implies the presence of a goiter. However, in some cases the volume of the thyroid gland is not increased. Therefore, when making a diagnosis, it is recommended to indicate the volume of the thyroid gland in milliliters, especially since ultrasound volumemetry is widely available in clinical practice.
Traditionally, thyrotoxicosis is classified according to severity (Table 3). However, the evaluation criteria are based on highly variable parameters (heart rate, weight loss, etc.). In this regard, it seems more appropriate to distinguish subclinical, manifest and complicated hyperthyroidism (Table 4).
During the treatment of manifest or complicated hyperthyroidism, decompensation, compensation or relapse are possible. These conditions reflect the effectiveness of the treatment measures taken, and therefore should be recorded in the clinical diagnosis.
When carrying out differential diagnosis to determine the cause of thyrotoxicosis, great importance is given to ultrasound, and in some cases, thyroid scintigraphy (Table 5). With Graves' disease, there is a decrease in the echogenicity of the thyroid tissue of a diffuse nature, an increase in its volume and increased blood flow. A diffuse increase in radiopharmaceutical (RP) uptake during scintigraphy allows one to distinguish Graves' disease from other causes of thyrotoxicosis. With functional autonomy of the thyroid gland (toxic adenoma, multinodular toxic goiter), a hot node (or nodes) and reduced uptake of radiopharmaceuticals by the rest of the thyroid tissue are detected. Thyrotoxicosis, not associated with thyroid hyperfunction (with destructive thyroiditis), is characterized by reduced absorption of radiopharmaceuticals [4].
Orbital ultrasound, computed tomography, and magnetic resonance imaging can be used to visualize pathological changes in retrobulbar tissues.
Treatment methods
There are several treatments for Graves' disease: the use of thyreostatic drugs (thionamides), radioiodine therapy and surgery. Each of them has a number of advantages and disadvantages. The most promising method of treatment is radioiodine therapy.
Drug therapy
Regardless of the chosen method of exposure, thyreostatic therapy is first performed to achieve euthyroidism. With the help of thyreostatics, it is possible to achieve remission of Graves' disease in 35–50% of patients. Long-term conservative treatment does not make sense for large goiters (thyroid volume > 35–40 ml), severe complications of thyrotoxicosis, relapse of thyrotoxicosis after 12–18 months of full thyrostatic therapy [20, 21].
Thionamides (thiamazole, propylthiouracil) block the synthesis of thyroid hormones and stop the manifestations of thyrotoxicosis. It is assumed that thyreostatics can have an immunosuppressive effect (Table 6).
At the initial stages of treatment, thyreostatics are prescribed in maximum doses: 30–40 mg/day thiamazole (1-methyl-2-mercaptoimidazole) for two or three doses or 300 mg/day propylthiouracil (6-propyl-2-thiouracil) for three or four taken after meals. The duration of action of thiamazole reaches 40 hours, while its activity is approximately ten times higher than that of propylthiouracil. With this therapy, after four to six weeks, 90% of patients with moderate thyrotoxicosis manage to achieve compensation for the disease. A laboratory sign of this is the normalization of the level of St. T4 (TSH level may remain reduced for a long time) [22]. From this point on, the dose of the thyreostatic agent is gradually reduced to a maintenance dose (thiamazole 2.5–10.0 mg/day, propylthiouracil 12.5–50.0 mg/day). Conservative treatment usually lasts from 12 to 24 months. The longer the thyreostatic therapy, the higher the likelihood of achieving stable remission. In the presence of a goitrogenic effect and/or prerequisites for the development of drug-induced hypothyroidism, a combination of thyreostatics with L-thyroxine (25–50 mcg/day) is recommended to maintain a euthyroid state [23].
The main disadvantage of thionamide therapy is the development of side effects. Minor side effects, such as skin manifestations (urticaria, rash, itching), arthralgia, are observed in approximately 5% of patients and, as a rule, only during the first few weeks of therapy [24]. If minor skin reactions occur, antihistamines may be prescribed. In the presence of persistent moderate and mild side effects, the thyreostatic drug should be discontinued and radioiodine therapy or surgery prescribed. If the last two treatment methods are not indicated, transfer to another antithyroid agent is possible [25].
When prescribing thyreostatics, patients must be informed about the possibility of agranulocytosis (0.5–0.7% of cases). Agranulocytosis is characterized by symptoms of an infectious disease. When they appear, therapy is stopped.
In addition to antithyroid drugs, beta blockers, glucocorticosteroids, sedatives and cardiac glycosides, and potassium preparations are used (Table 7).
Beta blockers can reduce the period of preoperative preparation by relieving symptoms from the cardiovascular system, which is achieved by direct action on beta receptors of adrenaline, as well as by influencing the peripheral metabolism of thyroid hormones. It should be emphasized that to assess the adequacy of the dose of thyreostatics, one cannot rely on pulse rate.
For patients with obvious thyrotoxicosis, beta-blockers (Anaprilin 120 mg/day for three to four doses or long-acting drugs, for example Concor 5 mg/day, Atenolol 100 mg/day once) are advisable to prescribe until drug-induced euthyroidism is achieved, and often for a longer period term. In severe, prolonged thyrotoxicosis and the presence of symptoms of adrenal insufficiency, glucocorticosteroids are indicated: prednisolone 10–15 mg/day orally or hydrocortisone 50–75 mg/day intramuscularly [26]. Drugs in this group should be discontinued gradually. Beta blockers should be used with caution in patients with asthma, congestive heart failure, bradyarrhythmia, and Raynaud's phenomenon. As an alternative, calcium channel blockers are indicated [27].
Surgery
Surgery was the first and main method of radical treatment for Graves' disease [28]. With its appearance in the 1940s and 1950s. less than 1% of experts recommend thyrostatic therapy and radioiodine therapy. However, according to recent foreign studies, surgery has again become the method of choice when indicated (versus radioiodine therapy), especially in patients with low socioeconomic status [29, 30]. In some cases, surgery is recommended immediately after diagnosis, in others - after conservative treatment, sometimes quite long.
The absolute indications for surgical treatment for diffuse toxic goiter are [31, 32]:
- large goiter with signs of compression of surrounding organs and anatomical structures, regardless of the severity of thyrotoxicosis;
- combination of DTG with neoplastic processes in the thyroid gland;
- severe form of thyrotoxicosis with heart rhythm disturbances such as atrial fibrillation;
- intolerance to thyreostatics;
- lack of lasting effect from conservative therapy for two years, relapse of the disease.
However, situations often arise that can be regarded as relative indications for surgical treatment:
- lack of qualified endocrinological care at the patient’s place of residence;
- social or living conditions that exclude the possibility of regularly taking medications.
Surgical treatment of DTG requires preoperative preparation of patients. Its main goal is to achieve a euthyroid state.
Depending on the severity of thyrotoxicosis, thyroid volume, and the presence of concomitant diseases, drug compensation of thyrotoxicosis is achieved at different times using different doses of thyreostatics. It is important to remember that poor compensation of thyrotoxicosis creates a threat of massive release of thyroid hormones into the bloodstream during surgery and the development of thyrotoxic crisis in the early postoperative period, a condition in which mortality reaches 60% [33].
Radioiodine therapy
In a number of cases (intolerance to thyreostatics, relapse of thyrotoxicosis, contraindications to surgical treatment associated with severe somatic diseases), therapy with radioactive iodine (131I) can be considered as the most optimal method of treatment (Table 8). However, it has certain limitations. It cannot be used in case of a large volume of the thyroid gland and a retrosternal location of the goiter. Treatment with 131I is contraindicated during pregnancy and breastfeeding. Hypothyroidism usually develops within 6–12 months after administration. In addition, in some situations, preparation for radioiodine therapy requires medical compensation of thyrotoxicosis with the help of thyreostatics. The latter are canceled five to seven days before the introduction of 131I [34–39].
Before radioactive iodine therapy, treatment with thiamazole is justified if there is a risk of exacerbation of thyrotoxicosis (that is, in those patients in whom symptoms are severe or the level of free T4 is two to three times higher than normal, in patients with cardiovascular disorders, endocrine ophthalmopathy). Patients at risk should also receive beta-blockers before radioiodine therapy. However, in case of agranulocytosis, an allergic reaction to a thyreostatic agent, radioactive iodine therapy can be prescribed without prior preparation.
Currently, the majority of patients with Graves' disease, as well as with other forms of toxic goiter, receive radioiodine therapy as treatment. This is due to the fact that the method is effective, non-invasive, relatively cheap, and free of the complications that can develop during thyroid surgery.
The goal of radioiodine therapy is to eliminate thyrotoxicosis by destroying hyperfunctioning thyroid tissue. In DTG, adequate 131I activity should be given as a single dose (10–15 mCi) to achieve hypothyroidism in patients. Follow-up includes determining the level of St. T4 and St. T3 at intervals of four to six weeks. If thyrotoxicosis persists six months after radioiodine therapy, re-treatment is indicated.
Conclusion
Thyrotoxicosis syndrome covers a wide range of pathologies, the main of which is Graves' disease. Currently, the main methods of correcting thyrotoxicosis are drug therapy, surgery and radioactive iodine therapy. A deep understanding of the problem and mastery of modern diagnostic methods make it possible to formulate a diagnostic algorithm necessary for applying a personalized approach to the management of such patients.