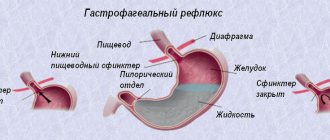
Cystic fibrosis is a severe hereditary chronic disease that occurs as a result of a mutation in a protein that is involved in the movement of chloride ions across the cell membrane, resulting in damage to the exocrine glands that produce sweat and mucus. The role of mucus in the human body cannot be underestimated: it moisturizes and protects organs from drying out and infection by pathogenic bacteria. Thus, disturbances in mucus production deprive a person of one of the most important mechanical barriers. Cystic fibrosis is incurable and inevitably leads to serious disruption of the functioning of internal organs.
What does the term “cystic fibrosis” mean if it is dissected into its component parts? “Mucus” is mucus, “viscidus” is viscous, which one hundred percent corresponds to the essence of the disease. Sticky, sticky mucus collects in the pancreas and bronchi, literally “clogs” and clogs them. Stagnant mucus is a favorable environment for the proliferation of pathogenic bacteria. The gastrointestinal tract, paranasal sinuses, kidneys and the entire genitourinary tract are also affected.
What is cystic fibrosis
Cystic fibrosis is a chronic genetic disease. The pathology is otherwise called “cystic fibrosis”.
The disease does not occur suddenly in men or women during adulthood. The diagnosis is made soon after birth. Since people are already born with the disease, it cannot be transmitted to other people.
Important! In approximately 4% of all patients with cystic fibrosis, the disease can be diagnosed in adults, and the entire period before this the pathology is asymptomatic.
Usually the pathology is detected in infants. When the disease can be identified in children under one year of age, the chances of preserving and prolonging the child’s life increase. Previously, patients with this disease soon died. However, now, although it is still impossible to cure the disease, with proper therapy, the life expectancy of people with this diagnosis is up to 35-45 years.
Cystic fibrosis in newborns leaves an imprint on a person’s entire life. Symptoms affect different areas of health. This is due to the fact that the pathology affects more than one system of the body. The digestive, respiratory, reproductive, intestinal and other systems are gradually involved in the pathological process.
The term cystic fibrosis comes from two Latin words meaning mucus and sticky. This is exactly what happens with all external secretion fluids: they thicken, stagnate and lead to disturbances in the organs.
Causes of cystic fibrosis
The main cause of cystic fibrosis is a hereditary pathology that occurs as a result of a mutation in the gene - the transmembrane regulator of cystic fibrosis. This gene is involved in the metabolism of epithelial tissues lining the digestive tract, liver, pancreas, reproductive and bronchopulmonary organs. The gene mutation leads to disruption of the structure of the synthesized protein, it becomes viscous and thick. Due to stagnation of mucus and an increase in the level of chlorine and sodium in it, the epithelium of the glands begins to decrease in size and is replaced by connective tissue.
The accumulation of mucus creates favorable conditions for the proliferation of opportunistic flora, therefore the risk of purulent complications and concomitant diseases increases sharply. With cystic fibrosis in adults, reproductive function is significantly affected.
Mechanism of disease development
The first signs of cystic fibrosis may appear in a child only at six months of age. However, the occurrence of the disease occurs due to the fact that both parents pass on a gene that has undergone a mutation, which is responsible for the normal production of fluids produced by different glands of the body.
The type of inheritance of cystic fibrosis is autosomal recessive. For a child to get sick, both the father and mother must pass on the broken gene. When the gene is passed on to only one of the parents, carrier status occurs, but the disease does not begin.
Forms of cystic fibrosis
The disease we are considering is characterized by many different manifestations that are relevant to it, and all of them are determined by the severity of pathological changes, the relevance of complications, as well as the age of the patient. The forms of cystic fibrosis can be the following:
- predominantly pulmonary (bronchopulmonary or respiratory);
- predominantly intestinal;
- mixed (in this case, both the respiratory system and the gastrointestinal tract are affected simultaneously);
- meconium ileus;
- erased and atypical variants of forms of manifestation of the disease.
This division of cystic fibrosis into forms is conditional, because the indication of predominantly pulmonary damage is compared with actual disorders of the digestive system, while intestinal damage is accompanied by the development of corresponding changes in the bronchopulmonary system. It is also important to note that the disease is characterized by a variety of clinical manifestations in each individual case of its occurrence. Many organs are affected, but the lungs, intestines, pancreas and liver are the most affected. Meanwhile, one of the most important features of cystic fibrosis is that the mental abilities of patients are in no way affected.
Erased and atypical forms of the disease can be identified as a result of examination for the relevance of chronic sinusitis in a child. At an older age, cystic fibrosis can be detected in case of infertility in men. Infertility in men, regardless of the form of the disease, is its concomitant pathology. It provokes azoospermia (lack of sperm in the seminal fluid), azoospermia, in turn, develops due to atrophy of the spermatic cord (i.e. due to its reduction in size or due to damage to its tissues, due to which the its inherent functions), due to its congenital absence or as a result of obstruction (i.e. obstruction). These disorders can also occur in those patients who are only carriers of the cystic fibrosis gene.
Cystic fibrosis in women manifests itself in a decrease in fertility (the ability to reproduce offspring), which is caused by an increased degree of viscosity, which is relevant for the discharge of the uterine cervical canal, which complicates the possibility of sperm migration.
Causes of the disease
The main cause of the development of this disease is a gene mutation. It is because of this that the disease is considered incurable.
The reasons why patients experience a wide range of symptoms are as follows:
- disruption of the secretion of normal sputum;
- excess calcium and sodium chloride in excreted fluids;
- accumulation of mucopolysaccharides.
Under the influence of this group of factors, complications associated with gene mutations develop.
CYSTIC FICIDOSIS: A MODERN APPROACH TO DIAGNOSIS AND TREATMENT
Recently, some progress has been made in the scientific approach to cystic fibrosis as a result of advances in the fields of cellular pathology, genetics and molecular biology. This article provides an overview of the current state of the problem of cystic fibrosis and addresses the main causes, mode of inheritance, modern therapy and new advances in the study of this pathology.
Cystic fibrosis (CF) is one of the most common autosomal recessive inherited disorders in the European population and represents an important cause of morbidity and mortality among children and young adults. In the past decades, the number of the CF patients has increased considerably due to improved diagnosis and a more comprehensive approach to therapy. Recently, the scientific knowledge about CF has been improved as the result of advances in cell pathology, genetics and molecular biology. This article reiews the current status of our understanding of CF: and covers the main causes, mode of inheritance, current therapy and new approaches to the pulmonary disease.
E. L. Amelina, A. G. Chuchalin Research Institute of Pulmonology, Ministry of Health of the Russian Federation, Moscow
Yes. L. Amelina, AG Chuchalin Pulmonology, Ministry of Health of the Russian Federation, Moscow
M
ucoviscidosis (CF) is a hereditary disease caused by systemic dysfunction of the exocrine glands. The disease was first described relatively recently, in 1938. Pathologist Dorothy Andersen described cystic degeneration of the pancreas in combination with pulmonary pathology in young children [1]. Then the English name of the disease arose - Cystic fibrosis (cystic fibrosis). In 1946, Farber proposed the term “cystic fibrosis” (from the Latin mucus - mucus, viscus - viscous), indicating the role of increased viscosity of excreta secreted by the exocrine glands. However, even earlier, in ancient German legends, it was indicated that if a salty taste is felt when kissing a child, the child is doomed [2].
N - normal gene M - cystic fibrosis gene
Fig. 1. Autosomal recessive type of inheritance in CF.
In recent years, scientific knowledge about CF and the mechanism of its development at the cellular and molecular level has rapidly developed. It is now known that CF is the most common monogenic disease among Europeans. Every 25th representative of the European race is a carrier of the CF gene. The prevalence of CF is highest in Central Europe - 1 affected child per 2000 births [3]. Epidemiological studies on the incidence of CF cases in Russia have established conflicting data - from 1: 3860 newborns [4] to 1:12,300 [5].
Rice. 2. The mechanism of ion transport through the apical membrane of an epithelial cell in CF.
Advances in the diagnosis and treatment of CF have led to significant changes in life expectancy for this disease. In 1938, 70% of those affected died within the first year of life. In 1996, the average life expectancy of CF patients in the United States and Western Europe reached 29 years. The similar figure for Russia is only 16 years [6]. A patient aged 72 years was observed at the Adult CF Center at Brompton Hospital. This lag is due to the insufficient development of the nationwide network of specialized CF centers and the lack of an independent CF clinic for adults.
Etiology and pathogenesis
CF develops as a result of a mutation in a gene located on the long arm of the seventh chromosome. The type of inheritance is autosomal recessive (Fig. 1). Currently, more than 400 mutations are known, of which the most common mutation in Europe and Russia is F 508 (loss of the amino acid finylalanine at position 508). Such a change in DNA structure leads to disruption of the function of the MB transmembrane regulator (CFTR), a protein that ensures the transport of chloride ions through the apical part of the epithelial cell membrane (Fig. 2). As a result of this defect, chlorine anions are retained in the cell, increasing the absorption of sodium and water cations, “drying up” the mucus produced by the exocrine glands. An increase in the viscosity of excreta leads to clogging of the ducts of the exocrine glands, accumulation of excreta and the formation of cysts. A picture of systemic dysfunction of the exocrine glands develops. Those organs are affected in whose epithelial cells the function of chloride channels is impaired. These are the upper and lower respiratory tract, sweat ducts, excretory ducts of the salivary glands, pancreas, bile ducts, intestines, vas deferens. Due to the blockade of chloride channels, reabsorption of chlorine and sodium ions in the sweat ducts does not occur, which leads to a significant increase in the concentration of these ions in 1 ml of sweat. This phenomenon is used in the diagnosis of CF. It should also be remembered that in the hot season, such patients experience a significant loss of electrolytes during physical activity, which can lead to collapse. Damage to the pancreas, caused by blockage of its ducts with a thick, viscous secretion, leads to the formation of cysts and subsequently to cystic fibrous degeneration of the pancreatic parenchyma. As a result, exocrine pancreatic insufficiency develops with symptoms of steatorrhea, malabsorption with concomitant deficiency of fat-soluble vitamins A, D, E, K, and retardation in physical development. At older ages, due to fibrous degeneration of the pancreatic stroma and damage to the islets of Langerhans, endocrine pancreatic insufficiency develops, leading to the formation of diabetes mellitus.
Damage to the bile ducts leads to the development of biliary cirrhosis with portal hypertension, expressed in varicose veins of the esophagus (possibly with bleeding from them), ascites, splenomegaly and hypersplenism. In all patients with CF, ultrasound examination can reveal a picture of cholestasis; in 15%, gallstones form against this background [7].
Fig.3. Plain radiograph of patient V., 15 years old, during an exacerbation of a chronic purulent-inflammatory process in the lungs (a) and after a course of IV antibacterial therapy (b). Focal and peribronchial infiltration has decreased, but gross strengthening and deformation of the pulmonary pattern, expansion of the roots of the lungs, and hyperairiness remain.
The main mechanism of intestinal damage is that due to impaired transport of sodium and chlorine ions, the content of electrolytes and fluid in the intestinal lumen is sharply reduced, which can lead to meconium intestinal obstruction in infancy, rectal prolapse in childhood, and the development of intestinal obstruction at the level of the ileocecal angle at an older age. Bilateral atresia of the vas deferens leads to azoospermia and male infertility in 97% of affected men [8]. Almost all patients with CF suffer from sinusitis; 30% of patients have nasal polyposis [9]. Lung pathology occupies a special place in the clinical picture of CF. It is lung damage with subsequent complications that leads to 70% of deaths in CF [7]. The pathological process in the lungs begins after the birth of a child, when a thick and viscous secretion forms in the lumen of the bronchi, leading to disruption of mucociliary clearance. The resulting mucostasis is a favorable basis for the development of infectious and inflammatory processes. Chronic purulent bronchitis and frequent bronchopneumonia lead to the formation of atelectasis, bronchiolo-bronchiectasis, and at a later age complications arise in the form of pneumothorax and pulmonary hemorrhage. As pathological changes in the bronchopulmonary system progress, ventilation-perfusion imbalance increases, hypoxia, pulmonary hypertension occurs, and chronic pulmonary heart disease forms. All this leads to an increase in respiratory and cardiovascular failure, which is the direct cause of death of the patient.
Clinical manifestations
A large number of mutations, affecting to varying degrees the quantity and quality of the CFTR protein in epithelial cells, determines the diversity of clinical manifestations of CF. Clinical manifestations of CF can occur both in early infancy and in a later period of the patient’s life. With a relatively benign course of the disease, CF can be asymptomatic for a long time; in some cases, the diagnosis is made during an examination for chronic sinusitis or male infertility. In the neonatal period, a slight increase in body weight and signs of malabsorption attract attention. In 10% of cases, CF begins with meconium ileus in early infancy [10]. In the postnatal period, repeated bronchopulmonary infections become the leading manifestation of CF. The diagnosis of CF is made based on the characteristic clinical picture combined with a positive sweat test. The classic diagnostic triad for CF is:
- positive sweat test (sweat chloride more than 60 mEq/L);
- pulmonary pathology of an infectious-inflammatory nature;
- intestinal syndrome.
The diagnosis is confirmed:
- burdened family history;
- positive result of genetic analysis;
- increased levels of immunoreactive trypsin in the blood (the study has diagnostic value for neonatal screening, since these indicators are increased from birth to 8 weeks of life);
- azoospermia caused by obstruction of the vas deferens.
When diagnosing CF, adults should pay attention to the characteristic appearance of the patient. These are, as a rule, young patients with signs of poor nutrition, short stature, and a long history of chronic bronchitis, bronchiectasis, chronic sinusitis or chronic pancreatitis. Active questioning can reveal complaints of diarrhea; girls may have menstrual irregularities. A physical examination of the patient reveals an asthenic physique, a barrel-shaped chest, and deformation of the distal phalanges in the form of “drumsticks.” Dyspnea and acrocyanosis may occur. On auscultation, rales of various sizes are heard over the lungs. Palpation of the abdomen can reveal an increase in the size of the liver and spleen. An X-ray examination reveals hyperairiness of the lungs, visible areas of infiltration or atelectasis, thickening of the bronchial walls, and a possible picture of pneumothorax. A computed tomography scan reveals multiple bronchiectasis. Pulmonary function tests reveal obstructive disorders in combination with an increase in residual volume. Restrictive changes are also possible as a result of developed pneumosclerosis. The diffusion capacity of the lungs decreases in later stages of the disease due to hypoventilation [11]. The electrocardiogram shows signs of tachycardia and overload of the right side of the heart. Microbiological analysis of sputum is extremely important for determining the causative agent of the infectious process in the bronchopulmonary system, for prognosis of the course of the disease and targeted prescription of antibacterial therapy. Antibacterial drugs recommended for the treatment of patients with CF
| Saphilococcus aureus | Cloxacillin | 25 mg/kg/day |
| Flucloxacillin | 70 mg/kg/day | |
| Fusidic acid | 50 mg/kg/day | |
| Clindamycin | 20 - 40 mg/kg/day | |
| Rifampicin | 15 g/kg/day | |
| Cephaloporin antibiotics 1st and 2nd generation | 100 mg/kg/day | |
| Pseudomonas aeruginosa | ||
| Prevention of chronic colonization | Ciprofloxacin | 20 - 50 mg/kg/day orally |
| Colistin | 1 - 2 million units in inhalation twice a day | |
| Chronic colonization | ||
| Treatment of exacerbations (3 weeks) | Azlocillin | 250 - 500 mg/kg/day intravenously |
| or | Piperacillin | 300 mg/kg/day intravenously |
| Amikacin | 15 mg/kg/day intravenously | |
| planned courses | Gentamcin | 8 - 12 mg/kg/day intravenously |
| 2 weeks every 3 months | Tobramycin | 10 - 20 mg/kg/day intravenously |
| 2 antipseudomonas | Netilmicin | 10 - 12 mg/kg/day intravenously |
| drug | Cefsulodin | 100 - 150 mg/kg/day intravenously |
| Ceftazidime | 100 - 250 mg/kg/day intravenously | |
| Aztreons | 150 – 250 mg/kg/day intravenously | |
| Thienamycin | 50 – 75 mg/kg/day intravenously | |
| Ciprofloxacin | 15 - 50 mg/kg/day orally, intravenously | |
| Long-term therapy | ||
| Colistin | 1 - 2 million units in inhalations | |
| Gentamicin | 160 – 240 mg twice daily | |
| Tobramycin | 100 – 300 mg | |
| Carbenicillin | 1 - 2 g |
The microbial landscape in CF is quite characteristic. In early childhood, Staphylococcus aureus (Staphylococcus aureus) dominates, then Haemophilus influenzae (Haemophilus influaenzae) joins, and Pseudomonas aeruginosa (Pseudomonas aeruginosa) appears in adolescence. In recent years, especially in Western Europe and America, Pseudomonas cepacia, or Burgholderia cepacia, which is resistant to most antibiotics, is often sown [12]. The addition of Pseudomonas aeruginosa infection can have various consequences for the patient: from asymptomatic carriage to, more often, a significant deterioration in the course of the disease with a pronounced activation of the inflammatory process and deterioration in functional indicators.
Treatment
CF treatment tactics are based on clinical, functional and microbiological data. The main goals of the therapy are:
- reduction of bronchial obstruction;
- infection control;
- improvement of the patient's nutritional status.
It is necessary to actively treat concomitant complications, compensate for the resulting respiratory and heart failure, and ensure maximum comfort for the patient in the terminal period of the disease. New, revolutionary treatments for CF (eg, gene therapy) are under development. Reduction of bronchial obstruction
carried out using several groups of drugs.
These are mucolytics, bronchodilators in combination with kinesitherapy techniques. Mucolytics - drugs that reduce the viscosity of sputum (N-acetylcysteine and its analogues) - are used in tablets, inhalations and intravenously. Since 1994, DNase has been used, a drug that breaks down the DNA of destroyed neutrophils in the bronchial lumen. As recently completed multicenter studies have shown, daily double inhalations of 2.5 mg of the drug lead to an improvement in the patient’s well-being, a decrease in the number of exacerbations, an improvement in functional indicators and, ultimately, in the patient’s quality of life [13]. Bronchodilators are also used to improve bronchial obstruction. These are drugs of b-agonists (salbutamol, salmeterol) and M-anticholinergics (ipratropium bromide). The effectiveness of their use is determined by the indicators of reversibility of obstruction after inhalation of the drug when studying the function of external respiration. Bronchodilators are most often used in a complex of daily procedures, including inhalation of mucolytics and kinesitherapy exercises. Kinesitherapy is a type of physiotherapy aimed at mobilizing and evacuating mucus from the bronchial tree. The most common forms of kinesitherapy are the active breathing cycle and huffing, autogenous drainage, postural drainage in combination with percussion massage. It is possible to use a flutter and a PEP mask (positive expiratory pressure) to create positive expiratory pressure and prevent expiratory collapse [14]. Fighting infection.
The introduction of antibiotics into the therapeutic armamentarium in 1940 was the most significant event that changed the prognosis of CF patients.
Antibiotics are still the cornerstone in the treatment of this pathology. Antibacterial therapy is prescribed taking into account the result of sputum culture in intermittent courses during exacerbations or routinely, as well as as part of basic therapy to prolong the period of remission between exacerbations (see table). The pharmacokinetics of antibacterial drugs in CF is changed: due to the acceleration of drug metabolism in the liver and increased renal clearance, the maximum concentration of the administered antibiotic in the blood serum of a CF patient is less than expected. Therefore, CF requires large doses of the drug with maximum frequency of administration. Antibacterial therapy for CF is based on the results of microbiological examination of sputum with determination of the antibiotic sensitivity of the isolated pathogen [15]. When treating exacerbations, the drugs of choice for staphylococcal infections are penicillin-resistant penicillins (flucloxacillin, dicloxacillin), 1st and 2nd generation cephalosporins (cephalexin, cefaclor), doxycycline, clindamycin, rifampicin, fusidine are also used. In recent years, methicillin-resistant staphylococcus has sometimes been cultured from the sputum of CF patients. In this case, vancomycin becomes the drug of choice. When colonized with Pseudomonas aeruginosa, therapy is usually carried out with the use of two antipseudomonas drugs, intravenously, for a course of at least 14 days. These are drugs from the group of 3rd generation cephalosporins (ceftazidime), aminoglycosides (gentamicin, sisomycin, amikacin), carbapenems (thienam, meronem). A drug from the group of difluorinated quinolones, ciprofloxacin, is the only antipseudomonal drug produced in tablet form, which is very important for outpatient management of patients. Treatment of exacerbations begins with an increase in temperature, increased cough, worsening shortness of breath, and an increase in the amount of sputum. Objective indicators of exacerbation are: oxygen desaturation, a decrease in forced expiratory volume per second by 10% or more, changes in the physical and radiological picture. In many CF centers, a course of intravenous therapy for carriage of Pseudomonas aeruginosa is carried out every 3 months as planned. Intravenous antibiotic therapy can be carried out not only in a hospital setting, but also at home. Outside of an exacerbation, long-term inhalation of antipseudomonal drugs (colimycin, carbenicillin, gentamicin) is recommended to suppress the ongoing infectious process. Long-term studies of the effectiveness and safety of inhaled antibacterial therapy have proven stabilization of clinical manifestations and improvement of functional indicators, as well as a decrease in colonization of Pseudomonas aeruginosa. Due to the lack of systemic exposure, side effects of inhaled antibacterial therapy are minimal. The effectiveness of inhalation therapy depends largely on the inhaler used. The combination of a nebulizer and compressor has a number of advantages over an ultrasonic nebulizer. When using a nebulizer, better dispersion is achieved, in which the inhaled drug penetrates the lower respiratory tract; In addition, the ultrasonic inhaler slightly heats the drug, which can change the properties of the antibiotic. Daily treatment for a CF patient should look like this: treatments begin with inhaled bronchodilator, if indicated; then - inhalation and/or mucolytic tablets; after 10 - 15 minutes - kinesitherapy, coughing; after a pause - antibiotic inhalation. Improving nutritional status
is very important for the general well-being of the patient and the course of the infectious process, the development of the respiratory muscles, and ultimately for the prognosis of the CF patient [16]. To correct it you need:
- identify exocrine pancreatic insufficiency;
- carry out constant replacement therapy with new generation enzyme preparations. These are microspherical enzymes with a pH-sensitive shell (Creon, pancitrate). The drug is prescribed with each meal in a dose of up to 2000 units. lipase per 1 kg of patient body weight. If, at a similar dosage, symptoms of malabsorption persist or there are signs of hyperacid gastritis, H2 receptor blockers (cimetidine, ranitidine) or proton pump inhibitors (omeprazole) are added to therapy;
- With adequate replacement therapy, there should be no restrictions in the diet of CF patients. On the contrary, taking into account the constantly ongoing infectious process, the calorie intake for CF should be 120 - 150% of the required, 35% of which comes from fats;
- additional intake of vitamins A, D, E, K is necessary - as a rule, double the usual daily amount is prescribed.
To prevent cholestasis, it is recommended to continuously take ursofalk (ureidodeoxycholic acid), a hydrophilic bile acid that prevents the formation of gallstones;
- if the above actions are ineffective, if the patient’s body weight decreases significantly, high-calorie nutritional supplements are prescribed in the form of cocktails, at a dose that replaces 800 kcal/day for adults. If necessary, resort to tube feeding at night using an esophageal or gastric tube.
A new direction in the treatment of CF is the use of anti-inflammatory therapy. Since bronchial obstruction in CF is largely caused by a hyperactive inflammatory reaction, it seems advisable to use steroidal and non-steroidal anti-inflammatory drugs. An American study that lasted 4 years and ended recently revealed a significant improvement in respiratory function in patients systematically taking ibuprofen, as well as a decrease in the need for antibacterial drugs [17]. Corticosteroid drugs are used to treat patients with CF with concomitant bronchial asthma or allergic bronchopulmonary aspergillosis. In a 4-year study to determine the effectiveness of systemic corticosteroid therapy at a dose of 2 mg/kg every other day, significant clinical and functional effects were obtained. However, according to delayed data (after 6 years), growth retardation, osteoporosis, and cataracts were identified in the group of patients receiving steroids [18]. Corticosteroid drugs are recommended for short courses in the treatment of exacerbations. The role of inhaled steroid therapy in the treatment of CF is currently being investigated. Treatment of complications.
As pulmonary pathology progresses in CF, complications such as hypoxemia develop, leading to pulmonary hypertension and the development of cor pulmonale.
In this case, long-term oxygen therapy is carried out (in accordance with blood gas parameters), treatment with angiotensin-converting enzyme inhibitors (captopril, enalapril), as well as traditional treatment of developing circulatory failure. Severe inflammation of the tracheobronchial tree, especially in areas of bronchiectasis, often leads to pulmonary hemorrhage, which, however, is rarely the direct cause of death of the patient. If conservative treatment is ineffective, angiography with embolization of the bronchial artery or surgery is recommended. Pneumothorax is a fairly common complication of CF in adults, developing due to rupture of subpleural bullae. After removing free air from the pleural cavity in case of repeated pneumothorax, chemical or surgical pleurodesis is performed. Now in countries where lung transplantation is performed, the indications for this procedure have been narrowed. Transplantation
is another option for CF patients after drug therapy resources have been exhausted. Indications for transplantation are severe respiratory failure with a forced expiratory volume of 1 second less than 30%, the absence of contraindications, and the active desire of the patient [19]. During transplantation, both lungs are transplanted; it is also possible to transplant the lung-heart complex, followed by the “domino” procedure, i.e., transplanting the heart of a CF patient to another recipient. Due to the severe shortage of donor organs, transplantation from living donors (one lobe from each parent) is sometimes performed, but this operation raises many ethical objections and is performed extremely rarely [19]. Another hope for CF patients and their doctors is gene therapy [20]. The CFTR protein gene has been synthesized, and active attempts are being made to introduce this gene into bronchial epithelial cells. It has been proven that even a 10% level of normal CFTR can ensure physiological lung function. The first clinical trials were conducted using an adenovirus vector (USA, Canada) and liposomes (England, France). A clinically significant result has not yet been obtained [20], however, research continues, since if successful, a new stage in the treatment of CF will begin - the stage of an etiological approach to the treatment of this disease.
Literature:
1. Andersen DH. Cystic fibrosis of the pancreas and its relation to celiac disease. A clinical and pathological study. Am J Dis Child 1938;56:344-99. 2. Chuchalin A.G., Samilchuk E.I. Cystic fibrosis - state of the problem. Ter. archive - 1993;65;(3):3-8. 3. Hodson ME, Geddes DM (Eds), London: Chapman and Hall, 1995. 4. Potapova O. Yu. Abstract - Molecular genetic analysis of cystic fibrosis in Russia - S.P. 1994, p. 24. 5. Petrova N.V., Materials of the scientific-practical conference of the RDKB - M - 1995, p. 96. 6. Kapranov N. I. Rachinsky S. V. Cystic fibrosis - M. - 1995. 7. Cystic Fibrosis Foundation. 1995. Patient Registry 1994 Annual Data Report. Bethesda, Maryland. 8. Taussig LM. The reproductive system, in Cystic Fibrosis Brugman, SM (Ed. LM Taussig), Thieme-Stratton, New York 1984;324-7. 9. Davis PB, et al. Cystic Fibrosis Am J Respir Crit Care Med 1996;154:1229-56. 10. Warner JO, et al. Cystic fibrosis in children, in Respiratory Medicine (second edition), London 1995:1330-40. 11. van Haren EHJ, et al. Bronchodilator response in adult patients with cystic fibrosis: effects on large and small airways. Eur J Respir Dis 1991;4:301-7. 12. Govan JWR, et al. Evidence of transmission of Pseudomonas cepacia by social contact in cystic fibrosis. Lancet 1993;342:15. 13. Hodson ME. Aerosolized dornase alfa (rhDNase) for therapy of cystic fibrosis. Am J 1995;151:70-4. 14. Pryor JA and Webber BA. Physiotherapy for cystic fibrosis-which technique? Physiotherapy 1992;78:105-8. 15. Webb AK. The treatment of pulmonary infection in cystic fibrosis Scand J Infect Dis Suppl 1995;96:24-7. 16. Cysyic Fibrosis Trust. Management of cystic fibrosis in adults UK 1995. 17. Konstan MW, et al. 1995 Effect of high-dose ibuprofen in patients with cystic fibrosis. 18. Niolaizik WH, MH. Schoni, 1996 Pilot study to assess the effect of inhaled corticosteroids on lung function in patients with cystic fibrosis J Pediatr 128:271-4. 19. Kotloff, Zuckerman. Lung transplantation for cystic fibrosis: special considerations Chest March 1996;109(3):787-98. 20. Southern KW. Gene therapy for cystic fibrosis: current issues. Brit J Hosp Med 1996;55(8):495-9.
Etiology of cystic fibrosis
Although there are many varieties of the disease depending on the organ affected, consider the main ones. The classification includes several forms.
Pancreatic lesions
Cystic fibrosis of the pancreas is cystic fibrosis, in which a disruption in the production of secretions occurs in this important organ. The substance produced by this gland contains a complex of enzymes involved in digestive processes. When the production of this secretion is disrupted, the extraction of useful substances from foods becomes impossible. As a result, even the most nutritious and healthy food passes through in transit and does not supply the body with valuable compounds.
When the liver suffers
One type of pathology is when the liver is affected. It is in this organ that bile is produced. Increasing its density leads to stagnation and serious consequences. Such problems are dangerous, but, fortunately, the liver is affected in only 4% of cases with cystic fibrosis.
Respiratory tract damage
The walls of the bronchi, lungs and other parts of the respiratory tract are covered with mucous membrane. The secretion occurs constantly and this is necessary so that foreign particles in the form of dust and pathogenic microorganisms are promptly removed from the body.
When cystic fibrosis occurs in the pulmonary form, involving the respiratory tract in the process, sputum stagnates in the bronchi and lungs, which leads to the settling of bacteria, viruses, and dust on the walls of organs. The smallest bronchi are completely blocked, which leads to obstructive conditions and interferes with proper ventilation of the lungs.
Damage to the genital organs
There are no complaints about the functioning of the genital organs in women with cystic fibrosis. The pathology does not affect the functioning of the reproductive system.
In men, the disease affects the testicles. These organs produce sperm. When these processes are disrupted, men become infertile. This occurs as a result of blockage of the reproductive ducts.
Changes in the functioning of the sweat glands
With cystic fibrosis, patients' sweat becomes excessively salty and sticky. The analysis will show increased levels of chlorine and sodium.
Damage to the gastrointestinal tract
The intestinal form of cystic fibrosis is common. Children with this pathology suffer from inadequate breakdown of food. Fats and proteins are the least digestible; the body accepts carbohydrates relatively normally.
When the digestive organs are damaged, putrefactive processes begin inside the tract. Abnormal breakdown of foods leads to the formation of toxic compounds that poison the body. Bowel movements become frequent, and cases of rectal prolapse are known.
When cystic fibrosis occurs in the intestinal type, the composition of saliva also changes. Chewing dry food becomes very difficult and patients have to drink plenty of water. All these disorders gradually lead to eating disorders and weight loss.
Meconium ileus
Meconium is original feces. With cystic fibrosis, sometimes the manifestation of the disease begins in the first days of life.
When meconium becomes too viscous, it blocks the intestinal passages. Parents may notice that the baby does not pass feces. After a day, the child becomes restless, often burps, and the stomach swells. Vomiting with bile is possible. The vascular pattern on the skin of the abdomen becomes clear, the skin becomes dry and flabby.
An immunoreactive trypsin test is performed. It turns out that this enzyme is not present, so a blockage occurs in the loops of the small intestine. The mucus thickens, and all the above-described signs appear. This problem can only be eliminated surgically.
Features of mixed flow
The mixed form of cystic fibrosis combines the symptoms of several types of course. The disease begins to manifest itself with severe bronchitis and pneumonia, and then intestinal syndrome occurs.
The earlier the doctor was able to diagnose cystic fibrosis and provide first aid, the greater the chance of a favorable outcome.
Symptoms of cystic fibrosis. Diagnosis in children
Most cases of cystic fibrosis are detected in the first two years of a child's life. The disease can be suspected based on the following signs:
- frequent, constantly recurring cough, shortness of breath;
- recurrent or chronic pneumonia;
- unformed, copious, oily and foul-smelling feces;
- chronic diarrhea;
- rectal prolapse;
- prolonged neonatal jaundice;
- retardation in physical development;
- constantly salty taste of the skin;
- swelling;
- deformation of fingers like “drum sticks”;
- enlarged liver and impaired liver function.
Photo: Jerry Nick / wikimedia.org
To diagnose cystic fibrosis, the following is carried out:
- collection of family history and DNA testing (expensive procedure);
- sweat test (using special analyzers to determine the content of sodium and chlorine ions in sweat);
- blood test for the level of immunoreactive trypsin (in cystic fibrosis, this pancreatic enzyme is 5-10 times higher than normal);
- They may prescribe an examination to detect dysfunction of certain organs due to cystic fibrosis (for example, lungs, gastrointestinal tract).
Symptoms of cystic fibrosis
Since cystic fibrosis affects several systems at once, the symptoms can be very diverse. The first exacerbation often occurs precisely in the first year of life, so parents should closely monitor the child’s well-being and, if negative symptoms occur, immediately show the baby to a specialist.
Important! In only 10% of cases of the disease, symptoms appear in the first days of life, with the most unfavorable prognosis.
Symptoms in newborns
When cystic fibrosis manifests itself in infancy, the baby develops symptoms of intestinal obstruction, which is associated with stagnation of meconium:
- absence of bowel movements;
- hysterical crying;
- bloating.
With palpation, you can feel the swollen intestine. Touching causes pain to the child, and the crying becomes stronger.
Symptoms in children under one year of age
At this age, pathology is diagnosed quite often. The main signs of cystic fibrosis during this period are slow weight gain and problems with the respiratory tract.
Important! We can talk about the presence of this genetic disease only if there are disturbances in two systems simultaneously, and not just in one.
You will have to treat the pathology if you have the following set of symptoms:
- instability of stool consistency;
- color change to yellow;
- acquiring a fatty consistency;
- persistent dry cough that gets worse during night sleep;
- attacks of suffocation due to blockage of small bronchi;
- frequent respiratory diseases.
Without assistance, periods of exacerbation will occur more often.
Symptoms depending on the affected system
Early examination of the child allows you to choose treatment that can help control the course of the disease and maintain normal well-being. Signs of the disease may differ depending on which system has undergone the pathological process.
If the digestive system is damaged, the following symptoms may occur:
- slow physical development due to lack of nutrients from food;
- stool disorders;
- enlarged spleen;
- weakness;
- nausea;
- headache;
- swelling of different localization.
Diabetes mellitus occurs less frequently.
When the respiratory system is affected, the intensity of symptoms increases as the stage progresses:
- collapse of some parts of the lung due to partial blockage of the bronchi;
- dry cough;
- hemoptysis;
- dyspnea;
- pale skin;
- discharge of scanty thick mucus.
If a bacterial infection occurs, the mucus may turn yellow or green.
Most symptoms can be stopped, but when adequate therapy is absent, irreversible changes begin in the organs.
general description
Cystic fibrosis (CF) as a given definition of an actual pathology is used in Europe (and, in fact, in our country), while in Canada, Australia, the USA and other countries it is defined as “cystic fibrosis of the pancreas”, and precisely in this version, the features of its morphological manifestations are revealed to the greatest extent. It should be noted that this disease is quite common, as evidenced by the frequency of its occurrence. Thus, only for newborns in European countries, a ratio of 1:2500 is determined, which, in turn, indicates that at least four out of 10,000 newborns have a chance of developing cystic fibrosis.
Cystic fibrosis occurs with the same frequency regardless of gender, that is, both boys and girls are equally susceptible to the disease. Considering the fact that we are talking about a genetic disease, it should be taken into account that patients are already born, and it is impossible to become infected with cystic fibrosis. Meanwhile, this disease can occur for a long time without symptoms, therefore it is advisable to consider cystic fibrosis in adults. Its symptoms are diagnosed in this form in approximately 4% of cases, although in the overwhelming majority this disease manifests itself during the first years of life. Considering the fact that children are born with it, it is often defined as hereditary cystic fibrosis or congenital cystic fibrosis.
Children become ill when they receive one mutant gene from each parent. If only one such gene is inherited, then in this case its carriage is considered (“CF carriers”), in which pathologies corresponding to the disease are not diagnosed. Given that the genes that each person has are paired, each of us, accordingly, is a carrier of two copies of each of the genes (again, one gene from the mother, one from the father). Certain genes are deprived of the ability to function normally if their structure is disrupted. With such a violation in the structure, the gene is altered. Therefore, in order for cystic fibrosis to develop (as, in fact, many other genetic diseases), it is necessary to obtain, as noted in the original example, two altered genes. If the parents are carriers of CF, any child of the couple has a 25% chance of receiving altered genes from each of them.
In approximately 70% of cases of the disease in question, it manifests itself before the child reaches two years of age. Due to the relatively recent introduction of neonatal screening into medical practice, the detection of cystic fibrosis has been significantly reduced over time.
Inheritance of cystic fibrosis
Diagnostics
Early diagnosis will help adults notice pathological changes in a child and provide timely assistance. This will save the child from using unnecessary drugs in the treatment of false bronchitis, pneumonia and other diseases.
First, the doctor will carefully determine the symptoms that have appeared. Classic blood and urine tests will not give any results. To obtain reliable information, sweat tests are carried out. If there is pathology, sweat will contain increased doses of chlorine and sodium. Sometimes the indicators exceed the norm by 3-5 times.
If there is doubt, a genetic examination can be performed to identify a gene defect. After this, there is no doubt about making a diagnosis.
The following studies are carried out less frequently:
- blood biochemistry;
- coprogram;
- sputum analysis;
- X-ray;
- MRI;
- CT;
- bronchoscopy.
The attending physician decides what studies to conduct.
What is this hereditary disease cystic fibrosis?
Cystic fibrosis (CF) is a mutation of one gene, transmitted hereditarily and causing thickening of secretions and blockage of the ducts of all vital organs. The disease was first diagnosed by American physician Dorothy Andersen in 1938. But the true cause of the disease, a mutated gene, was determined only in 1989.
This gene ( cystic fibrosis transmembrane regulator ) in a healthy person controls the intercellular transport of ions such as chlorine and sodium. In a sick person, their regulation is impaired. Due to this, the secretion secreted by the organs becomes thicker and cannot perform its functions.
Secretion plugs formed in the ducts are an excellent breeding ground for pathogens. As a result, a person’s immunity is greatly reduced, he is regularly and seriously ill and without treatment cannot lead a full life. It also leads to the formation of cavities that are hollow or contain fluid (i.e. cysts). Therefore, cystic fibrosis is often called cystic fibrosis .
The disease also has another, stranger name - salty kiss disease . In the 18th and 19th centuries, cystic fibrosis was so called because a mother, having kissed a sick child, felt the taste of salt on her lips, and midwives prophesied a short life for such children.
Europeans, especially children and adolescents, are most susceptible to the disease. According to statistics, about 5% of all patients with cystic fibrosis are people over 40 years of age. The disease is quite common. In Russia alone, one in 8,000 newborns has a mutated gene. Currently, pathology can be detected during the period of intrauterine development through neonatal screenings. But more often cystic fibrosis reveals itself during the first years of a child’s life.
The disease itself is not dangerous to others. If the patient takes appropriate medications, then he can have a family and children, who, with the right approach, are born healthy.
This gene is located on the seventh pair of chromosomes. If one chromosome from a pair has mutated, then the person is healthy, but is a carrier of pathology for his descendants. If both parents are sick or carriers, then a gene mutation in the child is inevitable.
Treatment
It is impossible to completely get rid of cystic fibrosis, since medicine has not yet learned how to correct damaged genes. Treatment consists of using agents that have a supporting effect on organs and systems. Therefore, therapy is symptomatic.
Diet is extremely important. When feeding newborns, it is better to give preference to breast milk, as it contains all the necessary substances and is well absorbed by the body. If the production of pancreatic enzymes is impaired, they are given to the child in the form of granules. Such drugs as Ermital, Creon and Panzinorm are suitable.
Important! Children with cystic fibrosis should be fed only on demand: crying, followed by a lull, and then crying again.
As you get older, it is important to watch your caloric intake. The diet should contain more calories, since much is not absorbed by the patient’s body. Enzymes and vitamin complexes may be prescribed.
If the respiratory system is affected, treatment at home includes the use of the following medications:
- "Acetylcysteine";
- "Ambroxol";
- "Lazolvan";
- "Carcysteine".
Constant use of these remedies allows patients to cough up accumulated mucus normally. Bronchodilators such as:
- "Salbutamol";
- "Fenoterol";
- "Berodual."
To choose a drug, it is better to consult a doctor. He will recommend a product that will be as comfortable to use as possible and is best suited for a specific age category.
Treatment with folk remedies can also give positive results. One of the effective methods is kinesitherapy. In other words, it is “movement therapy.” This folk method consists of performing a set of breathing exercises that can improve the patient’s condition without medications. The complex includes:
- percussion chest massage;
- active deep breathing;
- postural drainage (coughing with the head below body level).
It is important to strictly follow the doctor's prescription, even if some recommendations seem insignificant.
Diagnosis of the disease: newborn screening, genetic studies
For a long time, the only way to make a diagnosis was sweat tests. Today, genetic research is increasingly being used. Since 2007, in our country, all newborns in the maternity hospital undergo mandatory neonatal screening for the five most severe hereditary diseases, including cystic fibrosis. The study can also be done during pregnancy. But we are only talking about an attempt at early diagnosis of cystic fibrosis, which, undoubtedly, is important for prescribing adequate therapy, but the disease itself does not go away. It is hereditary and incurable.
The life expectancy of people with cystic fibrosis varies greatly from country to country. So, in America today the average is 48 years. However, this is the exception rather than the rule. This was achieved thanks to titanic efforts and coordinated work of doctors, scientists and public organizations. They are also actively trying to fight cystic fibrosis in Russia. However, these efforts are not enough, as statistics confirm - in our country, patients with cystic fibrosis live on average 10-15 years less.
These are the kind of reminders you can find in American hospitals. They briefly provide all the important information about the disease - symptoms, as well as the treatment necessary for the patient.
TAKE THE NEXTGEN21 TEST
Is it possible to prevent pathology
There is no specific prevention for this disease. If there have been cases of cystic fibrosis in the families of the husband and wife, during pregnancy or even before its onset, it is necessary to contact centers that conduct genetic examinations and identify the presence of this gene. As shown in the photo, a puncture of amniotic fluid or a piece of chorionic tissue can be taken. This will allow the DNA of the unborn child to be examined.
Competent actions of doctors and parents from the first days of life will allow the child to have as normal a life as possible with such a diagnosis.
Watch the video:
Diagnosis of cystic fibrosis
Diagnosis of cystic fibrosis may require both laboratory and genetic testing. Genetic studies are highly informative and allow one to suspect the development of the disease almost immediately after birth. At the moment, the disease can be detected even before the birth of a child through neonatal screening.
In order to confidently say that a person has cystic fibrosis, a doctor must diagnose the following indicators1,2:
- the presence of bronchial defects or the presence of thick and viscous sputum in the bronchi;
- positive sweat test results;
- the presence of pancreatic enzyme deficiency;
- cases of cystic fibrosis in the family.
How the disease develops
For the normal functioning of the respiratory and digestive systems, organs require mucus. Its role in the operation of these systems is enormous: mucus protects organs and mucous membranes from drying out, does not allow pathogenic microorganisms to multiply, and creates a comfortable environment for good microflora.
A lack of moisture in the intercellular space leads to a decrease in mucus production.
Normally, mucus should be present in the bronchi, covering the entire internal surface and protecting it. When exposed to air, dust, dirt, microorganisms, and foreign particles settle on the mucus and are gradually removed from the bronchial tree by coughing or sneezing.
If the amount of mucus produced is insufficient, the ciliated epithelium is the first to suffer. When microorganisms settle in the bronchi, they begin to use the ciliated epithelium as food.
This leads to inflammatory diseases, narrowing of the lumen of the bronchi, collapse of the alveoli and, as a result, stagnation of mucus.
Prevention
As for the prevention of cystic fibrosis, prenatal diagnosis is considered one of the most important measures to prevent the disease, with the help of which it is possible to identify the presence of a defect in the seventh gene even before birth. To strengthen the immune system and improve living conditions, all patients need careful care, good nutrition, personal hygiene, moderate physical activity and the provision of the most comfortable living conditions.
Chumachenko Olga, pediatrician
11 total today
( 153 votes, average: 4.55 out of 5)
Hydrocele in newborns - causes, symptoms and treatment methods
Hyperactive child: normal or disease?
Related Posts
Cystic fibrosis treatment
Treatment is carried out using inhalations and antibiotics
When cystic fibrosis is diagnosed and treated at an early stage, it becomes possible to significantly improve the quality of life and increase the life expectancy of the patient. Therapy is aimed at using a therapeutic diet, breathing exercises, taking medications, performing physical exercises and other procedures.
There is no general cure for cystic fibrosis. For lung infections, antibiotics are prescribed, which can be given intravenously, inhaled, or taken orally. Sometimes, in the treatment of cystic fibrosis, the antibiotic azithromycin can be prescribed for a long time. Inhalations with hypertonic saline solution and salbutamol are useful and effective. In severe cases of complete loss of function, transplantation may be a mild treatment option.
Pancreatic enzyme replacement medications and fat-soluble vitamin supplements are extremely important during childhood. The attending physician may prescribe physiotherapeutic procedures on the chest.
Prognosis and prevention
Previously, it was mainly pediatricians who dealt with the manifestations of cystic fibrosis; this disease was considered “children’s”. Currently, this pathology is often found in adults, which is explained by the increased capabilities of modern pharmacology. The drugs used make it possible to partially compensate for the impaired secretory functions of the mucous membrane of the bronchial tree and pancreas. And with adequately selected therapy, a child with cystic fibrosis has a chance to grow up.
Important: before use, read the instructions or consult your doctor.
How is cystic fibrosis inherited?
Features of inheritance of cystic fibrosis include:
- The SFTR mutation is recessive. This means that a person with a normal gene on a paired chromosome will not have any symptoms of cystic fibrosis. There are quite a lot of such people in the population. They are carriers of the disease and can pass on the pathological gene to their children.
- The transmission of the gene is not linked to gender, so boys and girls are equally likely to develop the disease.
- A child will have cystic fibrosis only if he inherits 2 defective genes at once. This is possible if both parents have at least one chromosome with a mutation in the corresponding region. The probability of having a sick child may vary (see table).
| Mother is healthy (both chromosomes without mutation) | Mother is a carrier (one gene is mutant, the other is normal) | Mother has cystic fibrosis (both genes are mutant) | |
| Father is healthy (both chromosomes without mutation) | In 100% of cases, children are healthy | The probability of having a carrier child is 50%, the probability of being a carrier is 50% | The probability of having an affected child is 0%, all children will be carriers |
| Father is a carrier (one gene is mutant, the other is normal) | The probability of having a carrier child is 50%, the probability of being a carrier is 50% | 25% chance of having a sick child, 25% chance of having a healthy child, 50% of being a carrier | The probability of having a sick child is 50%, the probability of being a carrier is 50% |
| Father has cystic fibrosis (both genes are mutant) | The probability of having an affected child is 0%, all children will be carriers | The probability of having a sick child is 50%, the probability of being a carrier is 50% | All children will have cystic fibrosis |
It should be understood that the likelihood of having a child with cystic fibrosis is affected only by the fact that the parents have an abnormal SFTR gene. The nature (type) of the mutation does not matter.
Signs
Manifestations of the disease can vary greatly depending on several factors:
- the onset of the first symptoms;
- patient's age;
- duration of the disease.
Patients with cystic fibrosis are mentally fully functional. Among them there are gifted and intellectually developed people. Experts distinguish three main forms of cystic fibrosis. The most common is the mixed type, in which the respiratory and gastrointestinal tracts are involved in the process.
However, in some cases, pulmonary and intestinal forms can occur in isolation. The disease rarely debuts after adulthood. Usually there is a transition of pathology from the childhood form to the adult form. Symptoms are similar in children and adults. Both men and women are diagnosed with infertility.
Pulmonary form
It is characterized by a gradual increase in symptoms. As a result, the disease takes on a chronic, protracted form. In newborns, the sneezing and coughing reflexes are not yet fully developed, so viscous secretions begin to actively accumulate in the respiratory section.
The first symptoms of bronchial lesions include cough with a slight discharge of viscous mucus, shortness of breath, bluish skin, disturbances in sleep and general condition. There are no symptoms of intoxication. Hypoxia (lack of oxygen) causes delays in physical development. Children gain weight poorly, they become lethargic and apathetic.
The following symptoms of cystic fibrosis indicate an infection:
Which doctor should I contact for bowel problems?
- heat;
- cough with thick purulent sputum;
- dyspnea;
- headache;
- nausea and vomiting;
- dizziness;
- disturbance of consciousness.
The patient's chest becomes barrel-shaped. The skin loses its elasticity and firmness and becomes dry. Hair loss is observed. They lose their shine and become brittle. With a long course, the nasopharynx is also affected. Sinusitis is added to the above symptoms. Polyps, adenoids, chronic tonsillitis.
Over time, the symptom of “drumsticks” and “watch glasses” develops. Due to pulmonary insufficiency, the phalanges of the fingers and nail plates are deformed. There are four main stages of development of bronchopulmonary cystic fibrosis:
- There is a persistent dry cough. Shortness of breath appears exclusively during physical activity. The first stage can last up to ten years.
- A dry cough turns into a wet cough. Chronic obstructive bronchitis is present. Shortness of breath appears even with moderate physical activity.
- Complications of cystic fibrosis develop. Pulmonary heart failure develops.
- Lasts only a few months and ends in death.
The photo clearly shows what the lungs look like with cystic fibrosis
Micrasim for cystic fibrosis
The use of enzyme preparations for cystic fibrosis allows one to partially compensate for the insufficient level of one’s own digestive enzymes. And such disorders are observed in almost all people with this disease, because damage to the pancreas is its typical manifestation. In this case, special attention is required to correct the level of lipase, an enzyme that ensures adequate digestion of fats in the small intestine. For this purpose, Mikrasim is prescribed for cystic fibrosis.
The expected clinical effects of such therapy include:
- Improving the absorption of basic nutrients, reducing the likelihood of nutritional malnutrition.
- Reducing the risk of developing diarrhea associated with insufficient digestion of fats.
- Reducing the severity of intestinal discomfort caused by increased gas formation and increased peristalsis against the background of enzyme deficiency.
Micrasim for cystic fibrosis can also be used to treat children in the first years of life, in this case the drug is prescribed in the form of capsules. The dosage is selected by the doctor taking into account the severity of steatorrhea and the age of the child.
Symptoms
Cystic fibrosis in most cases manifests itself before one year of age.
In 10% of cases, symptoms of the disease (meconium ileus or meconium ileus) are detected by ultrasound examination during fetal development in the 2-3 trimester.
In some children, intestinal obstruction is detected in the first days of life. Signs of meconium ileus are:
- lack of physiological excretion of meconium;
- bloating;
- anxiety;
- regurgitation;
- vomiting, in which the presence of bile is detected in the vomit.
Over the course of two days, the child’s condition worsens - pallor and dryness of the skin appear, tissue turgor decreases, lethargy and adynamia appear. Dehydration develops and intoxication increases. In some cases, complications may develop (intestinal perforation and peritonitis).
Intestinal cystic fibrosis manifests itself in most cases after the introduction of complementary foods or artificial feeding due to a deficiency of pancreatic enzymes. Symptoms of this form of the disease are:
- bloating;
- frequent bowel movements
- significantly increased fecal output;
- fetidity and light color of stool, the presence of a significant amount of fat in it.
Possible rectal prolapse when sitting on a potty (observed in 10-20% of patients).
There is often a feeling of dryness in the mouth, which occurs due to the viscosity of saliva, so eating dry food is difficult, and while eating, patients are forced to drink large quantities of liquid.
At the initial stages, appetite may be increased or normal, but due to digestive disorders, hypovitaminosis and malnutrition subsequently develop. As the disease develops, signs of cirrhosis and cholestatic hepatitis (increased fatigue, weight loss, jaundice, darkening of urine, disturbances in behavior and consciousness, abdominal pain, etc.) appear.
Cystic fibrosis of the lungs, due to overproduction of viscous secretions in the bronchopulmonary system, causes obstructive syndrome, which manifests itself:
- prolongation of exhalation;
- the appearance of whistling noisy breathing;
- attacks of suffocation;
- participation in the respiratory act of auxiliary muscles.
An unproductive cough is possible.
The infectious-inflammatory process is chronic and recurrent. Complications are observed in the form of purulent-obstructive bronchitis and severe pneumonia with a tendency to abscess formation.
Symptoms of the pulmonary form of the disease are:
- pale earthy skin tone;
- bluish discoloration of the skin caused by insufficient blood supply;
- presence of shortness of breath at rest;
- barrel-shaped deformation of the chest;
- deformation of the fingers (the terminal phalanges resemble drumsticks) and nails (resemble watch glasses);
- decreased physical activity;
- decreased appetite;
- low body weight.
Symptom of drumsticks and watch glasses in cystic fibrosis.
Bronchial contents usually include Pseudomonas aeruginosa, Staphylococcus aureus and Haemophilus influenzae. Flora may be resistant to antibiotics.
The pulmonary form is fatal due to severe respiratory and heart failure.
Signs of cystic fibrosis in the mixed form include symptoms of intestinal and pulmonary forms. The erased forms of the disease are usually diagnosed in adulthood, since special types of mutations in the CFTR gene cause a milder course of the disease, and its symptoms coincide with those of sinusitis, recurrent bronchitis, chronic obstructive pulmonary disease, cirrhosis of the liver or male infertility.
Cystic fibrosis in adults often causes infertility. 97% of men with cystic fibrosis have congenital absence, atrophy, or obstruction of the spermatic cord, and most women with cystic fibrosis experience decreased fertility due to increased viscosity of cervical mucus. At the same time, some women retain their reproductive function. Mutations of the CFTR gene are also sometimes found in men who do not have signs of cystic fibrosis (the mutation in 80% of such cases results in aplasia of the vas deferens).
Cystic fibrosis does not affect mental development. The severity of the disease and its prognosis depend on the timing of the disease manifestation - the later the first symptoms appear, the milder the disease and the more favorable the prognosis.
Since cystic fibrosis, due to a large number of mutation variants, is characterized by polymorphism of clinical manifestations, the severity of the disease is assessed by the condition of the bronchopulmonary system. There are 4 stages:
- 1st, which is characterized by unstable functional changes, dry cough without sputum production, slight or moderate shortness of breath during physical exertion. The duration of the first stage can reach 10 years.
- Stage 2, which is characterized by the development of chronic bronchitis, the presence of a cough accompanied by sputum, moderate shortness of breath at rest and worsening with exertion, deformation of the terminal phalanges of the fingers. When listening, the presence of hard breathing with moist, “crackling” wheezing is revealed. This stage lasts from 2 to 15 years.
- Stage 3, at which complications arise and the pathological process in the bronchopulmonary system progresses. The formation of bronchiectasis, zones of diffuse pneumofibrosis and limited pneumosclerosis, and cysts occurs. Heart failure (right ventricular type) and severe respiratory failure are observed. The duration of the stage is from 3 to 5 years.
- Stage 4, which is characterized by severe cardiorespiratory failure, ending in death within several months.