Acute appendicitis is one of the most common acute surgical diseases of the abdominal organs. The mortality rate for this disease is 0.1–0.3%, and the number of postoperative complications remains quite high and reaches 40% in complicated forms [1].
The use of laparoscopic appendectomy in emergency surgery for acute appendicitis can improve treatment results and save patients from traumatic laparotomy and associated complications [2]. In recent years, this method has become a priority; there have been reports of the use of laparoscopic appendectomy for acute appendicitis complicated by peritonitis or appendiceal abscess [3–9]. However, the possibilities of expanding the indications for the use of endovideosurgical technology in the treatment of acute destructive complicated appendicitis have not been fully determined and require further research.
The purpose of the study is to improve the results of treatment of patients with acute inflammation of the appendix and its complications through the widespread use of laparoscopic appendectomy.
Cause
The main reason indicating the need for surgery is an acute form of inflammation of the appendix or suspicion of appendicitis. Other factors that bring the patient to the operating table:
- Increased symptoms of body poisoning by products of the inflammatory process.
- Violation of the integrity of the appendix and penetration of purulent products into the internal organs, the development of peritonitis.
- Increased risk of rupture.
Depending on the patient’s condition and the stage of the disease, the operation is performed in two ways:
- According to plan.
- In an emergency, or urgent form.
Planned
Surgical intervention is used if removal is impossible or prohibited. This is usually carried out in the presence of infiltration. Initially, drug treatment is performed to relieve the acute form, and then cutting is prescribed when there is no threat to the health and life of the patient.
Urgent
The acute form of the disease provokes emergency removal. Occurs when an organ ruptures and peritonitis.
The development of chronic appendicitis is associated with the periodic occurrence of a discomfort state. Its treatment is carried out using medications and surgery. The doctor chooses the methods. If symptoms appear infrequently and not intensely, they try to treat with medications.
Advantages and disadvantages of laparoscopic appendectomy
The important advantages of laparoscopy over classical appendectomy are:
- Excellent cosmetic result;
- Lower incidence of complications, in particular adhesive disease;
- Low trauma;
- Short recovery period and rapid restoration of working capacity;
- Possibility of a full examination of the abdominal organs and, if necessary, performing other surgical operations without widening the incision;
- Economic benefits due to shorter hospitalization, less medication consumption and faster return to work.
The disadvantages of the method include the need for expensive equipment, staff training, and the inability to perform laparoscopy in patients with certain concomitant diseases.
Indications for laparoscopy of appendicitis:
- Appendicitis;
- Mucocele;
- Benign tumor processes, cysts, parasitic lesions;
- Carcinoid tumors.
As you can see, the reasons for laparoscopy are similar to those for open surgery, and the form of appendicitis and the presence of complications do not always serve as an obstacle to minimally invasive intervention.
Russian surgeons have identified groups of patients with concomitant diseases who, if possible, should undergo laparoscopy:
- Diagnostically unclear cases when observation does not completely exclude an acute inflammatory process in the appendix (diagnostic laparoscopy turns into therapeutic);
- Young women who do not exclude the possibility of becoming pregnant and giving birth to a child, in whom it is difficult to distinguish between acute appendicitis and gynecological pathology. In women, unjustified appendectomy reaches, according to some data, 47%, and subsequently it results in adhesions and secondary infertility;
- Women of any age seeking the best cosmetic effect;
- Patients with certain concomitant diseases that increase the risk of purulent complications - diabetes mellitus, obesity;
- Children for whom laparoscopy is preferable due to the low likelihood of adhesions later.
An important reason for laparoscopic removal of appendicitis is the desire of the patient himself to undergo just such treatment. Of course, in this case, the latter should weigh all the pros and cons, and if there is insufficient trust in the surgeon or the absence of a highly qualified specialist, the desire will still have to be abandoned.
Contraindications to laparoscopy of the appendix are similar to those for other surgical diseases:
- Severe concomitant diseases of the kidneys, liver, heart;
- Long periods of pregnancy;
- Severe coagulopathies and bleeding disorders.
Many surgeons consider pregnancy as a relative contraindication, because the negative effect of pneumoperitoneum on the fetus has not been proven, and impeccable surgical technique and minimally invasiveness make it possible to maintain pregnancy and speed up the recovery of the expectant mother.
Blood clotting disorders also have a dual meaning. On the one hand, they can lead to massive bleeding, on the other hand, such patients, if appendicitis occurs, one way or another need its treatment, so it is still better if the operation is less traumatic, and if replacement therapy is prescribed, laparoscopy for coagulopathies does not lead to greater blood loss than in people with normal coagulation.
Relative contraindications may be old age, severe obesity, atypical location of the appendix, peritonitis, but in these cases the issue of surgical access is decided individually.
In addition to general pathology, local contraindications are also identified. These include:
- Dense inflammatory infiltrate in and around the appendix;
- Pronounced adhesive process;
- Abscessing periappendicular process - when gas is pumped into the abdominal cavity, it can rupture and lead to peritonitis, and manipulation of such an abscess is fraught with damage to large vessels and the intestinal wall;
- Advanced peritonitis with the formation of a large conglomerate of intestinal loops, massive fibrinous deposits, many foci of purulent inflammation (abscesses), which require open surgery, a full revision and lavage of the abdominal cavity.
Diagnostic examination
Before removing an organ, an examination is carried out and tests are taken. This is done to exclude other pathologies to confirm the diagnosis.
Inspection
The surgeon first examines the patient to identify symptoms of appendicitis. The procedure consists of palpation and tapping the area of the body where it hurts, and preliminary determination of the location of the appendage. Attention is paid to what position the patient takes. A visual examination of the condition of the abdomen is performed. At the site of inflammation, the skin will be raised and inflamed.
Blood and urine tests are taken to determine the degree of inflammation and rule out diseases with similar symptoms.
Instrumental examination
The use of equipment is necessary to make an accurate diagnosis and determine the location of the appendix:
- Ultrasonography.
- Computed tomography using contrast.
Operation stages
Traction. The distal end of the appendix is grabbed with a clamp inserted through access 3 and lifted towards the anterior abdominal wall
.
The vermiform appendix is freed from adhesions and adhesions, and then positioned so that the mesentery is in the frontal plane
.
The mesentery is transected in one of 4 ways.
1. An electrosurgical monopolar clamp or dissector is inserted through access 2
.
In small portions of 2-3 mm, the mesenteric tissue is captured and coagulated, moving towards the base of the appendix (Fig. 18-5, see color insert). Particular care is required near the dome of the cecum. The following sequence of actions is strictly observed: a small portion of tissue is captured with a dissector, removed from the intestine and only then coagulated
.
Pay attention to the proximity of intestinal loops to the instrument. This method is the simplest, provides reliable hemostasis and takes little time
.
It is necessary to completely isolate the base of the appendix along the entire circumference, preparing it for the application of a ligature
.
2. To treat the mesentery, you can use bipolar coagulation, which is safer, but requires a special instrument and is somewhat longer in time. With an infiltrated thickened mesentery, bipolar coagulation is less effective and requires fragmentation of the mesentery
.
3. Ligation of the mesentery with a ligature: a window is formed at the base of the appendix in the mesentery, a ligature is passed through it, both ends of which are removed out through a trocar
.
The node formed extracorporeally is lowered into the abdominal cavity (Fig
. 18-6, see color insert).
The mesentery is divided with scissors. The application of individual titanium clips is quite expensive and unreliable, especially in infiltrated tissues
.
4. The mesentery is crossed with a stapler
. The appendix stump is formed in one of 3 ways.
1. The ligature method is the most common in laparoscopy. It is recognized as safe by domestic and foreign surgeons
.
After crossing the mesentery, an endoloop is inserted through access 3, placed over the appendix and lowered to the base using a clamp (Fig
. 18-7, see color insert).
The loop is tightened and the ligature is cut off. Usually, one or two ligatures are left on the stump of the appendix, superimposed on each other (one of them can be replaced with an 8-mm clip)
.
A ligature, clip or surgical clamp is also applied to the distal stump of the appendix, using which the specimen is immediately removed after cutting off (Fig
. 18-8—18-10, see color
insert and Fig
. 18-11).
The size of the stump above the ligature is 2-3 mm
.
After cutting off the appendix, the mucous membrane of the stump is superficially coagulated with a spherical electrode inserted through access 2 (Fig
. 18-12).
We remind you that coagulation near metal clips is unacceptable. With sufficient experience, the duration of LA does not exceed the time of open surgery, amounting to 20-30 minutes
.
2. Hardware method
.
Through a 12-mm trocar from access 3, an endosurgical stapler is inserted, which is applied separately to the appendix and its mesentery, crossing sequentially
.
If the tissue thickness is small, both structures are stitched at the same time (Fig
. 18-13).
Hardware appendectomy reduces the operating time and allows, if necessary, aseptic resection of the dome of the cecum
. The only drawback of the method is the high cost of the stitching machine.
Rice. 18-11. The vermiform appendix is removed immediately after cutting off
.
Rice. 18-12. The mucous membrane of the stump is carefully coagulated with a spherical electrode.
Rice. 18-13. Hardware appendectomy
.
Rice. 18-14. Removing the drug through a 10/20 mm adapter sleeve.
3. Immersion of the stump into the dome of the cecum by applying intracorporeal purse-string and Z-shaped purse-string sutures
.
The technique was developed by the founder of LA
K. Zemm [9]. It requires quite painstaking work and perfect mastery of the endosurgical suture technique.
Removing the drug is a crucial moment of the operation. To avoid the spread of intra-abdominal infection, the drug is removed immediately after cutting off. It is necessary to prevent contact of the inflamed appendix with the tissues of the anterior abdominal wall, otherwise infection of the tissues will most likely lead to the development of purulent complications
. To do this, use one of the following methods:
1 . If the diameter of the appendix and mesentery is less than 10 mm, the drug can be easily removed through trocar 3
.
2. For larger drug diameters, a 10/20 mm adapter sleeve is used (Fig.
. 18-14).
3. The appendix is placed in a container before removal.
End of operation. The intervention area is thoroughly washed with 500-700 ml of antiseptic solution
.
The patient is returned to the original position, and the rinsing water is aspirated. A drainage is installed in the abdominal cavity
. The wounds are sutured.
The postoperative period is much easier than after a traditional appendectomy. The patient is activated by the end of the first day after removal of the drainage
.
Liquid food is allowed
.
Antibiotics are prescribed to all patients. The duration of the hospital period after LA is 3-7 days
. In uncomplicated cases, the period of disability does not exceed 14 days.
Types of surgery
An appendectomy is the surgical removal of an inflamed organ (appendix). The entire process is cut out, the remains are sutured and hidden inside the cecum.
In surgical practice, two main methods of intervention inside the patient’s body are used:
- Laparotomy. An incision is made in the area where the inflamed appendix is located. Open surgery.
- Laparoscopy (endoscopy). For removal, small punctures (three) are made in the abdominal area.
The methods have both positive and negative aspects.
Laparotomy
Is the classic way. Laparotomy is the first abdominal operation performed on the appendix. Indications:
- The diagnosis was confirmed: acute appendicitis.
- The acute form gave complications - peritonitis.
- Consequences of an acute illness in the form of an infiltrate that connects the appendix, cecum, small intestine and omentum.
- Chronic appendicitis.
Peritonitis and clinical signs of acute illness are indicators for urgent surgery. When there is an infiltrate inside, conservative treatment is used aimed at relieving the inflammatory process. Therapy can take 2-3 months. Then a planned removal is scheduled.
When laparotomy should not be performed:
- The patient is in agony.
- If the patient independently refuses surgical procedures in writing.
- Planned intervention. Dysfunction of the cardiovascular system, breathing, kidneys and liver.
Preparation for the operation does not require special measures. If the patient has a violation of the water-salt balance or peritonitis has developed inside, then liquids and broad-spectrum antibiotics enter the body through intravenous administration.
Progress of the operation:
- Introduction of anesthetic solution. General anesthesia is given. The solution enters the body either through injection into a vein or through an inhalation device. It is extremely rare that anesthesia is administered through the spinal canal.
- The site of the future operation is treated with antiseptic agents. Iodine in alcohol, betadine, and alcohol are used as disinfectants.
- An incision is made in the area where the appendicitis is located. Penetration inside is carried out by cutting tissue layer by layer.
- A visual inspection of the internal contents is carried out. The appendix rises above the organs.
- The process is cut off (resection is performed). In this case, sutures are placed at the site of the incision of the mesentery and appendix.
- Then excess fluid is removed, a drainage system is installed (tubes for removing inflammation products), and sanitation is carried out with tampons and electric suction.
- The incision in the peritoneum is sutured with special threads. Access is closed by layer-by-layer stitching of tissues in the reverse order of penetration.
Access to the peritoneum is carried out according to the following options:
- Volkovich-Dyakonov method, oblique incision.
- Lenander's method. Longitudinal section.
- Access via transverse incision.
Drainage is performed in several cases:
- Rupture of the appendix and development of peritonitis.
- Formation of pus at the site of surgery.
- Inflammation develops in the retroperitoneal tissue.
- Incomplete blockage of blood vessels damaged as a result of surgery. Incomplete hemostasis of arteries.
- There are no clear indications for cutting out an inflamed organ.
- There was an incomplete immersion of the remnants of the process into the body of the cecum.
The drainage is removed after 2-3 days if healing proceeds without complications.
The cutting process during laparotomy takes from 40 minutes to one hour. If complications are present (adhesive disease, incorrect location of the organ), then the surgical process lasts from two to three hours. The recovery process lasts up to a week. It is recommended to remain in bed for 2-3 days from the day of surgery. External sutures are removed on the 7th or 10th day.
Appendicitis Clinic
At the onset of the disease, the clinical picture is similar to other diseases. Women may perceive painful sensations as inflammation of the appendages. Men, feeling pain in the bladder, mistake it for a urological or kidney problem.
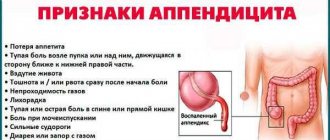
You should be wary if in adults:
- Pain, discomfort in the abdomen on the right side, usually starting in the morning or at night.
- Tight belly.
- Rapid pulse.
- White tongue.
- Nausea, repeated vomiting.
- Fever 2-3 hours after the onset of pain.
- Flatulence.
- Diarrhea or false urge to have a bowel movement.
- Difficulty walking, relief when lying down.
In children under 3 years of age, this disease practically does not occur, since breastfeeding creates protection against inflammatory processes.
Children from 3 to 7 years old cannot correctly explain their pain, therefore, to recognize appendicitis, you need to rely on the following signs:
- Decreased activity.
- White coating on the tongue.
- Shifting pain from the navel to the right lower abdomen, sometimes above the pubis or in the right hypochondrium.
- An increase in body temperature up to 40 degrees, not associated with a cold.
- Lack of appetite.
- Nausea and vomiting.
- Frequent bowel movements or diarrhea, possibly mucus.
- Pain in the abdomen, unending for several hours, aggravated by coughing.
- When pressing on the abdomen, the pain decreases.
- Impaired urination.
Children over 12 years of age have symptoms similar to those of an adult. A special feature is the “toxic scissors” syndrome. At normal body temperature or its decrease, a rapid pulse of up to 120 beats per minute is observed.
Treatment methods
The traditional scenario for the operation to remove the appendix is carried out by creating a small incision not exceeding 12 centimeters. The entire procedure can be divided into several stages:
- Introducing the patient into a state of anesthesia. Today, removal of the appendix is most often performed under general anesthesia. If there are contraindications to general anesthesia, anesthesia is performed using the tight infiltration method or through conduction blockade;
- After this, the surgeon dissects the abdominal wall layer by layer, this allows you to avoid postoperative complications associated with damage to nerve endings, as well as respond in a timely manner to the sudden occurrence of bleeding;
- The muscles, like the edges of the surgical wound, are separated by blunt surgical instruments;
- After opening the internal space of the abdominal cavity, the doctor carefully examines the abdominal wall itself, assesses the condition of neighboring organs and begins to remove the intestinal loops, behind which the appendix itself is located;
- Next, the surgeon removes the appendix and sutures the surgical wound. First, the inflamed process is isolated from other tissues using a clamp and ligature;
- The surgeon places a purse-string suture on the stump (the edges of the sutures are inside the stump);
- After completing all surgical procedures inside the abdominal cavity, the surgeon forms external sutures. The peritoneal walls are usually held together using self-absorbable suture material. The surgeon places from 8 to 12 stitches, using synthetic or silk threads;
- The external postoperative suture must be removed 1 - 2 weeks after surgery.