What is gastritis?
The diagnosis of gastritis can be made only after studying the morphological structure of a biopsy sample from the gastric mucosa.
Unfortunately, this often does not happen, and people with epigastric pain and heartburn are unreasonably diagnosed with gastritis. But this symptomatology fits only into the concept designated as functional dyspepsia - a short-term digestive disorder. Inflammation of the stomach, in turn, is a rather serious disease.
Clinical picture
Clinical manifestations are determined by the type of gastritis; symptoms are optional and nonspecific.
Chronic gastritis type A most often occurs in middle and old age, with clinical symptoms of a “flaccid stomach”, aching pain and a feeling of discomfort after eating food, belching, and an unpleasant taste in the mouth. Most often, this form of gastritis is characterized by a long asymptomatic course until B12-deficient megaloblastic (pernicious) anemia develops.
With bacterial gastritis (Helicobacter) type B, which most often develops in young people, there are complaints of severe pain in the epigastric region, most often provoked by errors in the diet (fried or spicy foods, chocolate, alcohol consumption). Painful sensations occur during meals or after 20–30 minutes; in some cases, hunger pain and night pain occur; I am worried about heartburn, belching and regurgitation, and an unpleasant taste in the mouth. A tendency to constipation often develops.
Long-term Helicobacter gastritis with increased secretory function of the stomach, in addition to the above, is characterized by the occurrence of symptoms of “intestinal” dyspepsia in the form of stool disorders (constipation, unstable stools, flatulence, rumbling).
In the case of Helicobacter antral gastritis in the stage of secretory hyperfunction, the occurrence of an “ulcer-like” symptom complex, which can be regarded as a pre-ulcerative condition, cannot be excluded.
Similar complaints, in most cases, are present in some forms of gastritis, accompanied by changes in gastric motility, increased gastroesophageal reflux and exacerbation of the disease.
The clinical symptoms of type C gastritis (reflux gastritis) do not always correspond to the degree of gastric damage established by endoscopy and histological examination; even identified obvious gastric lesions can be asymptomatic. The patient is sometimes bothered by pain during or immediately after eating food, nausea, vomiting, and heartburn.
Radiation gastritis, which can occur after the use of radiation therapy, is accompanied by moderate or severe coagulation necrosis of the gastric mucosa with the development of secondary inflammatory infiltration. The damaging effects of radiation depend on the dose of radioactive radiation. Minor changes are usually reversible and regress with the restoration of the mucosa to its normal state within 4 months.
Severe radiation damage is accompanied by the appearance of ulcers, fibrosis and obliterating hyalinosis of blood vessels.
Eosinophilic (allergic) gastritis is characterized by chronic diarrhea, intolerance to certain foods and pharmaceuticals. A patient with this type of gastritis experiences abdominal pain, nausea, vomiting, weight loss, and eosinophilia is detected in the blood.
General clinical symptoms include astheno-neurotic syndrome (general malaise, increased irritability, cardialgia, low blood pressure are not excluded).
Atrophic forms of chronic gastritis, which are combined with secretory insufficiency, may have symptoms similar to dumping syndrome (spontaneously occurring weakness, loose stools, pale skin with cold sweat that appears after eating).
The occurrence of chronic gastritis, accompanied by B12-deficiency anemia, is characterized by weakness, fatigue, and hypersomnia; a decrease in vitality with loss of interest in the environment is detected. The patient is bothered by pain and burning in the mouth, tongue, paresthesia in the lower and upper extremities simultaneously on both sides.
The occurrence and progression of atrophic disorders of the gastric mucosa are highly dependent on the duration of the disease and the age of the patient. The spread of atrophic gastritis occurs in the direction from the antrum of the stomach to its body, and the widespread form of type B gastritis gradually forms.
Severe malaise, loss of appetite, symptoms of a “flaccid stomach”, symptoms of polyhypovitaminosis with secretory deficiency and B12-deficiency anemia distinguish it from the previously mentioned antral variant of chronic gastritis and are similar to chronic gastritis type A+B.
During a general examination of the patient, there may be no signs of the disease.
The most dangerous complications of gastritis are the occurrence of gastric bleeding and malignancy.
Briefly about the anatomy of the stomach
The stomach is a muscular organ located between the esophagus and duodenum in the epigastric region. It is separated from the first by the cardiac sphincter, and from the second by the pyloric sphincter. The wall is represented by the following three layers:
- serous - provides sliding relative to other organs;
- muscular - promotes mixing and movement of the food bolus (motor function);
- mucous - with the help of cells of this layer, digestive enzymes, mucus and hydrochloric acid are produced (secretory function).
The regulation of the muscular system is carried out by the autonomic nervous system, the stomach itself (the release of gastrin into the blood, which enhances the active activity of the glands of the stomach or gastronomy), hormone-like substances of the duodenum and pancreas. The body itself has the following divisions:
- bottom;
- body;
- major and minor curvature;
- antrum.
Laboratory research
To conduct a comprehensive diagnosis of gastritis, various studies can be performed. To identify the disease, the patient must undergo some tests from the list given in the table.
| Type of analysis | Description |
| Donating blood for general analysis | Using this diagnostic procedure, the biochemical composition is checked. They take blood from a finger. The analysis is carried out quite quickly, the results are usually ready in no more than two hours. The procedure must be carried out on an empty stomach. The patient must first avoid drinking alcohol and not eating fried foods. In the presence of pathology, a reduced number of platelets and hemoglobin, as well as leukocytes and erythrocytes, is detected. ESR is considered a fundamental indicator of the presence of the disease. In the case of gastritis it is increased. |
| Taking a stool test | Fecal sampling allows you to collect data on the presence of purulent or bloody discharge. The analysis helps to identify inflammation or pathologies in the gastrointestinal tract of an infectious nature. Before collecting stool, it is advisable for the patient to avoid eating foods high in iron. |
| Analysis of urine | It allows you to verify the correct diagnosis and determine the presence of concomitant diseases. |
| Donating blood for biochemical analysis | Allows you to differentiate gastritis from other pathologies. |
After laboratory tests, the patient must undergo hardware diagnostics.
Analyzes are also mandatory
Why does gastritis occur?
For its occurrence, a number of provoking factors are necessary, which lead to various types of gastritis. Among them:
- Helicobacter pylori infection. Today it is considered the main cause and according to P. Ya. Grigoriev, Doctor of Medical Sciences, Professor, it is this that is the cause of gastritis in 95% of cases. The microorganism was isolated in 1983 from the antrum of a patient with gastritis. This was done by B. Marshall and D. Warren. But it is worth noting that more than 90% of the population is infected with the bacterium, but not everyone experiences an inflammatory process in the stomach. From this we can draw a logical conclusion that infection is only a predisposing factor, but not the primary cause. Helicobacter easily survives in an acidic environment, even at pH values equal to 2. It produces many biologically active substances, thanks to which it overcomes protective barriers, colonizes the gastric mucosa and damages it. Among them: urease, mucinase, alkaline phosphatase, superoxide dismutase, phospholipase, adhesin proteins and others;
- autoimmune factor (about 15% of cases). Characterized by the formation of antibodies to parietal cells of the mucous membrane. They are localized in the area of the body and fundus of the stomach and produce hydrochloric acid and specific intrinsic Castle factor - a gastromucoprotein necessary for converting vitamin B12 into its active form;
- duodenogastric reflux. This is the reflux of the contents of the duodenum into the stomach due to insufficiency of the pyloric sphincter. Pancreatic and duodenal juices lead to the destruction of the protective mucous barrier in the stomach, especially in the antrum. Most often occurs after surgical interventions on the stomach;
- medications. Negatively affect the stomach with long-term use: glucocorticoids (Prednisolone), non-steroidal anti-inflammatory drugs (Aspirin, Diclofenac, Ketorolac, Ibuprofen, etc.), cytostatics (Methotrexate), anti-tuberculosis drugs (Isoniazid), potassium chloride;
- allergic factor. In persons with food allergies, in particular to fish, dairy products, chocolate, inflammatory changes are often found in the gastric mucosa;
- disturbance of the rhythm of nutrition (dry food, poorly chewed), consumption of low-quality products, especially smoked meats, fried and spicy foods. So, in an experiment on dogs, feeding them ground red pepper caused the development of gastritis. This also includes alcohol abuse;
- smoking. Components of tobacco smoke contribute to damage to the mucous barrier, an increase with a subsequent decrease in secretory function, and disruption of the regeneration (self-healing) of gastric epithelial cells.
Among the diseases that can provoke gastritis, the most important are chronic pancreatitis, hepatitis, cholecystitis and colitis (inflammation of the pancreas, liver, gallbladder and large intestine).
The development of gastritis is now increasingly promoted by stressful situations.
Indeed, today they are simply impossible to avoid. They are present in the life of every person every day. When exposed to them, there is an increase in the production of hydrochloric acid by the parietal cells of the stomach, the excess of which affects the gastric mucosa.
But what happens to the stomach? When exposed to an etiological agent, the mucous membrane and cells of the integumentary epithelium are initially damaged. The number of glandular cells decreases, cellular infiltrates are formed, represented by lymphocytes, neutrophils and plasma cells. As this process progresses, it can move to deeper structures of the mucous membrane; in addition to inflammatory changes, degenerative (destructive) changes with complete or partial atrophy of the glandular formations of the stomach begin to be present. Gastritis is prone to progression and damage to new parts.
Tests for the study of stomach diseases
To diagnose a specific pathology of an organ and its classification, it is mandatory to undergo the following types of tests:
- General blood and urine analysis. The result will show whether the patient has an inflammatory process in the body.
- Fecal analysis. This procedure is necessary in order to find out how food is digested and to monitor the presence or absence of blood impurities in the masses in order to exclude or confirm perforation of the ulcer.
- Biochemical blood test. The doctor pays attention to indicators such as cholesterol, hemoglobin and sugar levels. They allow you to identify concomitant diseases: pancreatitis, diabetes or anemia.
- Determination of blood group. If the patient's outpatient card does not indicate the blood type, this test is mandatory. This is necessary in case of an emergency, if the patient suddenly needs a transfusion.
- Enzyme immunoassay blood test. Performed to identify the bacterium Helicobacter pylori. It is this that in most cases causes the development of stomach diseases.
Diagnosis of chronic gastritis includes all of the listed types.
What are the types of gastritis?
First of all, there is an acute type of gastritis. It occurs with a single exposure to a strong irritating factor. For example, when various chemicals enter the stomach, medications that negatively affect the stomach, etc. It can also occur quite often in acute infectious diseases and metabolic disorders in the body. The following forms are distinguished:
- catarrhal or simple. Occurs especially often in children. It is a consequence of poor nutrition (strict diets, consumption of large doses of alcohol, fried and spicy foods) or poisoning, even minor ones. There is probably no person who has not endured it at least once. The gastric mucosa becomes reddened (hyperemic), with foci of dystrophic changes and infiltration with leukocytes;
- corrosive. Occurs when there is contact with strong alkalis or acids, salts of heavy metals - lead, mercury, cadmium. Foci of necrosis (death) appear in the stomach tissues;
- fibrinous. Manifests itself in severe infectious diseases such as typhoid fever, diphtheria, tuberculosis, etc.;
- phlegmonous. Characteristic is purulent melting of the gastric wall with penetration of pus into the mucous membrane. It may occur as a complication, for example, of stomach cancer or peptic ulcer.
Acute forms can be completely cured after eliminating the causative factor.
Chronic gastritis according to the Houston classification is divided into:
- autoimmune (type A) - autoantibodies are formed to the parietal cells of the stomach. Accompanied by B12-deficiency (pernicious) anemia due to insufficient production of Castle factor;
- bacterial (type B) - associated with Helicobacter pylori infection. It is the most common type;
- chemical (type C) - due to the reflux of bile acids into the stomach from the duodenum.
Special forms of gastritis:
- radiation;
- granulomatous - occurs with Crohn's disease, which can affect any part of the gastrointestinal tract, including the oral cavity;
- eosinophilic or allergic;
- lymphocytic - a rather poorly studied species;
- hypertrophic or Menetrier's disease, characterized by increased development of the mucous membrane with the subsequent formation of adenomas and cysts in the stomach - benign formations.
There are many other forms of gastritis, such as viral, fungal, tuberculous, erosive, erosive-hemorrhagic, associated with amyloidosis, sarcoidosis, and renal failure. They are quite rare, and in each specific case it is better to contact a competent specialist.
Laboratory methods for examining chronic gastritis
THIS IS REALLY IMPORTANT! Right now you can find out a cheap way to get rid of stomach pain. FIND OUT >>
An adult patient or child must undergo general and specific tests:
- Test for general blood parameters. Gastritis can be suspected by detecting low hemoglobin, platelets, erythrocytes, leukocytes with an increased ESR.
- Laboratory evaluation of stool for the presence of occult blood and Helicobacter. This test determines the amount of acidity that can cause poor digestion.
- General urine test. It is done for prevention and allows you to detect underlying diseases and the presence of a secondary infection.
- Biochemistry analysis. The method allows you to differentiate gastritis from pancreatic diseases, and identify the presence of Helicobacter. In case of Helicobacter pylori infection, the blood will show normal values for the parameters being studied. If there is autoimmune chronic gastritis, hyperbilirubinemia is determined, which is confirmed by anemia due to vitamin B12 deficiency, a decrease in protein content, and a jump in gamma globulins.
- Specific tests. They are carried out to detect other microbes that have caused intoxication of the body, such as salmonella, staphylococcus, shigella. Tests are carried out for the concentration of protein and its fractions in plasma, calculation of pepsinogen in the blood and digestive juice, determination of the activity of alkaline phosphatases, transaminases, concentrations of electrolytes such as potassium, sodium, calcium.
- Bacteriological analysis.
- Immunological research.
Return to contents
Symptoms
The clinical picture will depend, of course, on the localization of the inflammatory process. When the body of the stomach is damaged, only heaviness in the epigastric region persists for a long time, which appears immediately after or during meals, especially spicy ones. If the antrum is damaged, problems arise with the evacuation of the food bolus from the stomach, an increase in pressure inside the organ occurs and, as a result, increased reflux from it into the esophagus. For a long time, a person may not feel the presence of the disease due to the active regeneration of the mucous membrane, but as the process progresses, the symptoms become, as they say, “in your face.” Dyspeptic syndrome is formed, manifested by:
- heartburn, manifested by a burning sensation behind the sternum. Occurs when acidic contents from the stomach reflux into the esophagus;
- pain or burning sensation in the epigastric area;
- belching of bitter, sour or just air;
- regurgitation;
- a sour feeling in the mouth;
- nausea and vomiting. Sometimes they are the only manifestations of gastritis.
This picture is more typical of gastritis with high acidity, but in case of its decrease it is possible:
- bloating, due to the fact that due to a disorder in the coordinated functioning of the alimentary tract, poorly digested food enters the underlying sections from the stomach, the local microflora is activated, and the product of its vital activity is an increase in gas formation;
- bowel dysfunction;
- weakness, pale skin, drowsiness;
- feeling of fullness or heaviness in the epigastric area;
- belching “rotten egg” due to insufficient digestion of food, its stagnation and developing fermentation processes.
If this symptom complex appears, you should consult a general practitioner or gastroenterologist.
Differential diagnosis of angina pectoris and myocardial infarction
Leading pain syndrome Angina pectoris (lat. angina pectoris, outdated synonym: angina pectoris) is a disease characterized by pain or discomfort in the chest
Myocardial infarction is one of the clinical forms of coronary heart disease, occurring with the development of ischemic necrosis of the myocardium due to absolute or relative insufficiency of its blood supply
With MI, the painful attack lasts longer (30 minutes or more), is accompanied by severe hemodynamic disturbances, and is not relieved by nitroglycerin. Fear of death is also characteristic.
“Rapid response” enzymes that enter the peripheral bloodstream from the necrosis zone: (with MI), also leukocytosis, with a shift in the leukocyte formula to the left.
• myoglobin is a muscle protein (the norm in the blood is up to 40 ng/ml), with myocardial damage it increases 10 times or more within 1-2 hours (the maximum increase is after 4-8 hours). Normalization occurs by the end of the first day of MI.
• Troponin-T (a specific myocardial protein not found in skeletal muscle) has its first peak at 2-3 hours with a peak at 8-10 hours, and high levels remain for 4-7 days. A single measurement of this test after 72 hours can be an indicator of the prevalence of MI.
• the MB-CPK isoenzyme is more specific (in high concentrations it is noted only in the heart, but in low concentrations it is found in skeletal muscles). A level of less than 10 μg/L indicates small-focal MI, and more than 10 μg/L indicates large-focal MI.
• total CK (norm - 20-80 conventional units, or up to 1.2 mmol/l, in SI) increases after 4-6 hours (peak after 1-2 days), and normalizes on the 4th day
During an attack of angina, there are no laboratory changes.
Changes on the ECG: In case of MI – the necrosis zone on the ECG is reflected by changes in the QRS complex, the appearance of a pathological Q wave in leads located above the infarction area, elevation of the ST segment above the isoline in leads located above the infarction area, discordant displacement of the ST segment below the isoline in the leads, opposite the infarction area, negative T wave in leads located above the infarction area.
With Angina: Outside of an attack of angina, there are no characteristic changes on the ECG. However, if it is possible to register an ECG at the time of an attack, a decrease in the ST segment is detected. The same changes can be detected when performing a test with physical activity (bicycle ergometry).
Diagnosis of gastritis
To clarify the diagnosis of gastritis after collecting patient complaints and mandatory palpation (palpation) of the abdomen, the following can be used:
- intragastric pH-metry - to determine the secretory function of the stomach;
- fibrogastroduodenoscopy with mandatory collection of material for biopsy. It is performed using a special device - a gastroscope equipped with a video camera. It is a fairly informative research method that allows you to assess the condition of the mucous membrane, the exact localization of the inflammatory process, and the presence or absence of precancerous changes. Before the study, fairly simple preparation is carried out. A light dinner is allowed until 6 pm; teeth cleaning; taking oral tablets and giving injections; Drink water two to four hours before the test. It is only prohibited to eat food on the day of the procedure, even if it is planned for the second half of the day;
- definition of Helicobacter. Urease or breath tests are used; polymerase chain reaction; enzyme immunoassay, which allows you to determine antibodies to it in the blood; determination of specific antigens in feces such as HpSA or in saliva; their detection during cytological or histological examination in biopsy specimens taken during FGDS (at least 5 fragments are taken);
- stool occult blood test. It is carried out to identify complications of gastritis (for example, peptic ulcer) or diagnose erosive forms that can be accompanied by varying degrees of bleeding;
- ultrasound examination of internal organs (liver, pancreas, gall bladder) - to identify concomitant pathologies;
- electrogastroenterography. Using this method, you can detect reflux (reflux) from the duodenum into the stomach, i.e. allows you to evaluate motor-evacuation function;
- Manometry of the upper gastrointestinal tract - determines the pressure in the stomach and duodenum.
Patient examination
At the first stage of the examination, the doctor interviews and examines the patient. Before determining gastritis, it is necessary to carry out a differential diagnosis with gastric and duodenal ulcers, peritonitis and gastric bleeding.
A general examination of the patient allows one to assess the severity of his condition. For gastritis it will be satisfactory. The patient behaves calmly, without showing excessive activity, as in pathologies that cause acute pain.
The doctor assesses the patient's position. When gastritis worsens, a person may take a forced position to relieve pain. Most often this position is on the side. The knees are pulled towards the stomach.
The patient's consciousness is clear. He calmly and accurately answers all the doctor's questions. If the disease is accompanied by pain, this is expressed in facial expressions.
The skin is normal. Their color has not changed. With gastric bleeding, pale skin is observed. In addition, the patient breaks out in cold sweat.
Chronic gastritis is often accompanied by dry skin and the appearance of cracks in the corners of the mouth. There is also an unpleasant odor from the mouth.
When examining a patient, the doctor pays special attention to the tongue. The condition of the mucous membrane of the tongue is assessed. With gastritis and other stomach diseases, plaque appears on it.
Hypoacid gastritis causes a condition called “geographic tongue.” The taste buds atrophy and as a result, discolored areas of the mucous membrane appear. Often the pathology is accompanied by cracks in the tongue.
When visually assessing the condition of the abdomen, attention is paid to whether it takes part in breathing. If not, then the doctor may suspect pathologies such as perforated ulcers and peritonitis.
After a general examination of the patient has been carried out, additional examination methods are prescribed.
Modern treatment. Is it possible to cure gastritis forever?
Depending on the cause of the disease, different treatment regimens may be used. Thus, for gastritis associated with Helicobacter pylori infection, eradication therapy is carried out - three- or four-component. The first includes:
- proton pump inhibitors - Pantoprazole, Omeprazole, Esomeprazole, Dexlansoprazole, etc.;
- two antibacterial drugs from the following - Amoxicillin, Tinidazole, Metronidazole, Clarithromycin, Josamycin, Furazolidone, Levofloxacin, Tetracycline.
In the second regimen, bismuth preparations are added, for example, bismuth tripotassium dicitrate (De-Nol). It is more rational to use antibacterial agents three days after taking proton pump inhibitors. During this time, the latter create an optimal environment in the stomach for the complete destruction of Helicobacter.
The effectiveness of eradication therapy is achieved 2 weeks after discontinuation of all drugs by determining Helicobacter pylori antigens in the patient’s stool.
If proton pump inhibitors are intolerant, H2-blockers of histamine receptors - Famotidine and Ranitidine - can be used. It is worth noting that when taken repeatedly, their effect decreases (the phenomenon of tachyphylaxis), so they should not be used for long-term treatment. To temporarily eliminate symptoms, antacid drugs can be used - Maalox, Phosphalugel (allowed during pregnancy), Gaviscon, Almagel, etc.
The combination of drugs is selected only by specialists.
A special place is occupied by the correction of the patient’s emotional background. Most gastritis is associated precisely with disruption of the autonomic nervous system. Against this background, disturbances in the regulation of secretory activity and gastric motility may occur. For this purpose, herbal preparations can be used in mild cases, for example, valerian, motherwort, hawthorn and their various combinations (Novo-passit, Central B, Alora, etc.); in severe cases - Grandaxin, Tenoten, Betamax.
To treat autoimmune gastritis, symptomatic therapy is used, including in the initial stages drugs that help reduce the secretion of hydrochloric acid, gastroprotective drugs (Venter, De-nol, etc.), antispasmodics (No-shpa, Drotaverine, Platyfillin). With the development of atrophic processes, they switch to replacement therapy with the following drugs:
- Acidin-pepsin;
- Pepsidil;
- Abomin;
- natural gastric juice.
In the treatment of chemical gastritis, it is important to identify a drug that promotes the development of inflammation of the gastric mucosa and promptly discontinue it. With reflux gastritis, it is necessary to normalize the circulation of bile. Ursodeoxycholic acid drugs can help with this - Choludexan, Ursohol, Urosan, etc. In addition, prokinetic drugs are used to correct motor skills - Motorix, Cerucal, Domperidone, Motilium, Primer.
Instrumental methods
For these purposes, various equipment and tools are used. A broader complex is used for chronic inflammation than for acute inflammation. In the latter case, the main method is examination, since the manifestations are more pronounced in children and adults.
PAY ATTENTION! Do not prolong gastritis or an ulcer until stomach cancer, it is better to be on the safe side, but this will be necessary. read the story of Galina Savina >>
Fibrogastroduodenoscopy is one of the main diagnostic methods included in the group of endoscopic ones. Tools:
- a probe in the form of a thin flexible tube;
- mini camera on the probe;
- a monitor on which the information received by the camera is visualized.
The examination requires inserting a probe into the digestive organ through the mouth and esophagus. FGDS determines:
- location of inflamed foci in the gastric walls;
- type, nature, stage of membrane damage;
- excludes peptic ulcer disease.
Simultaneously with the stomach, the duodenum is examined, which is often also affected by gastritis. Endoscopic examination results:
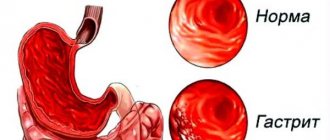
- When the mucosa is shiny with fibrin plaque, which is hyperemic and edematous with foci of hemorrhage, non-atrophic or superficial gastritis is diagnosed.
- With severe thinning of the membrane with a smoothed relief, gray color and translucent choroid plexuses, atrophic gastritis is determined. The disease is considered moderate if thinning areas alternate with small areas of white atrophy of varying shapes. If atrophy has reached the last stage, a sharp thinning of the mucous membrane of a cyanotic hue is visualized, which is easy to wound with a simple touch. In this case, folds are not detected.
- With an enlarged pylorus, hyperemic and edematous mucosa, and a significant amount of bile in the stomach, reactive gastritis resulting from chemical poisoning is diagnosed.
- Multiple or single erosive areas form on the mucous membrane during drug-induced gastritis.
- If large folds, similar to the convolutions of the brain, and excessive amounts of mucus are found in the stomach, hypertrophic gastritis is diagnosed. The shell can be easily damaged. Erosions often bleed.
Return to contents
Biopsy
Produced during FGDS. A special probe is used to remove a piece of affected tissue from the walls of the stomach of a child or adult for laboratory testing. The samples are taken from different parts of the stomach. This makes it possible to more accurately determine or refute the presence of Helicobacter, the activity of which is different in different parts of the organ. For this purpose, 2 biopsies are taken from the antrum and the body of the digestive organ. The Helicobacter test is performed using 4 methods:
- bacteriological;
- morphological, which includes the determination of cytology, tissue histology;
- reduced biochemical;
- immunohistochemical.
Return to contents
pH-metry
It is known that gastritis is an acid-dependent pathology, so an analysis is required to determine the acid content in gastric juice. For these purposes, pH measurement is used, which is classified as:
- Express test is a probe method for measuring acid in the stomach using special electrodes.
- 24-hour pH-metry, which allows you to evaluate the dynamics of fluctuations in acidity levels in two ways:
- tube, carried out by introducing a nasogastric tube into the digestive organ;
- probeless, which involves swallowing a capsule, which is attached to the wall of the stomach to transmit information to the acidogastrometer, and then removed from the body naturally;
- endoscopic pH-metry, which involves taking and analyzing a biopsy sample during FGDS.
Return to contents
Gastric juice assessment
Gastric contents are collected during gastroscopy. Beforehand, an adult or child needs to take a special breakfast with components that stimulate the secretion of digestive juice. The method allows you to determine the cause of inflammation of the walls of the organ. For example, an increased gastrin content indicates the presence of Helicobacter bacteria in the body. Focal gastritis with tissue atrophy is characterized by reduced acidity, decreased activity of pepsin and gastricsin. A strong change in these parameters indicates severe atrophy. Antral gastritis is manifested by three types of secretion:
- hyperreactive;
- hyperparietal;
- panhyperchlorhydric.
Is it possible to cure gastritis forever?
As we found out, there are a huge number of types of gastritis and conditions that provoke it. Thus, we can conclude that with proper and timely detection of the cause of this condition and its elimination, gastritis can be eliminated forever. In this case we are talking about acute forms of inflammation of the stomach associated with Helicobacter or another infection. For complete recovery it is necessary:
- follow the recommendations of a conscientious attending physician;
- eradicate all family members, since this bacterium is transmitted from sick people, and the infection rate is more than 90%. Even in cases of successful getting rid of it, you can soon “pick it up” again, even from a loved one (through kissing, eating from the same dish, etc.);
- after treatment, you must use only your personal utensils and other household items;
- give up alcohol and smoking;
- avoid stressful situations or other psycho-emotional overload;
- maintain a rest regime with sufficient night sleep (at least seven to eight hours a day);
- Do not eat foods that irritate the gastric mucosa.
Unfortunately, autoimmune gastritis, reflux gastritis and other rare forms are very difficult to treat, and in some situations lifelong use of medications that alleviate the condition is recommended.
ethnoscience
It is best to use folk remedies as an addition to the main therapy and only after consultation with your doctor.
In some cases, this treatment can only cause harm.
To treat gastritis with high acidity, the following can be used:
- sea buckthorn berries. 200 g should be poured into a liter of boiled water, strain and consume 3 tablespoons half an hour before meals for 3 weeks;
- natural honey. Before each breakfast, dissolve a spoonful of honey in a glass of warm water and drink it all in one go. It should be used for at least one month;
- herbal infusion. Consists of St. John's wort, celandine, chamomile and yarrow. Pour the mixture of medicinal herbs into one liter of boiling water and leave for half an hour. Take half a glass 3 times a day, treatment course is 3 weeks. The infusion may also be suitable for relieving acute stomach pain;
- decoction of flax seeds. It also helps with the feeling of heaviness. To prepare, you need to pour 3 tablespoons of seeds with a glass of boiling water and leave for 1 day. Take 2 tablespoons half an hour before meals for at least ten days;
- sea buckthorn oil. Suck from the tip of a spoon three times a day for three weeks. Repeat the course in a month;
- potato juice. Drink half a glass half an hour before breakfast. The course of therapy is at least two weeks. After a few weeks, if the effect is positive, the procedure can be repeated;
- peppermint infusion. It will not only help in the treatment of gastritis, but also calm the nervous system. To prepare, use 3 tablespoons of crushed leaves, pour boiling water over it, and infuse. Take half a glass in the morning and evening for up to 10 - 14 days.
For gastritis with low acidity, other remedies are used. Among them:
- blackcurrant juice. On an empty stomach in the morning you need to drink half a glass of fresh juice, the course of treatment is no more than one week. It stimulates the production of hydrochloric acid;
- infusion of elecampane root. Pour boiling water over 20 g of crushed roots, leave for an hour, strain. Take a tablespoon half an hour before meals for at least two weeks;
- mumiyo. 1 g of the drug must be dissolved in a glass of water. Drink a glass once a day in the morning ten minutes before meals.
The drug Befungin can also be included in this group. It contains growths of the birch chaga fungus, which has an anti-inflammatory, tonic effect, improves motility of the gastrointestinal tract. It is an excellent addition to the treatment of chronic gastritis.
When treating with the traditional method, it is necessary to remember possible allergic reactions.
Treatment
Therapeutic measures for gastritis must necessarily take into account the type of gastritis, the severity of clinical symptoms, the characteristics of secretion and the phase of the disease.
In the majority of cases, treatment measures are carried out in an outpatient setting; in case of exacerbation or difficulties in differential diagnosis, it is recommended to hospitalize patients.
To eliminate pain and dyspeptic disorders, an integrated approach is required, which includes observing work and rest (avoiding physical strain, minimizing negative emotions and nervous overload), which can provoke impaired motility of the digestive tract, following dietary recommendations, and taking pharmaceuticals.
During an exacerbation, a mechanically, chemically gentle diet with limited consumption of large amounts of food is recommended. As the symptoms of gastritis are eliminated, nutrition should be complete, using a stimulating effect during the period of remission in patients with insufficient secretory and acid-forming functions of the stomach.
Patients with various types of gastritis are prohibited from chocolate, coffee, carbonated drinks, and alcohol.
It is necessary to exclude from the diet: canned food, concentrates and surrogates of various products, herbs, spices, as well as products that provoke fermentation processes (milk, sour cream, grapes, black bread); Smoked, fried and fatty foods, and culinary products made from butter dough are excluded.
The diet should include a complete, balanced set of proteins, fats and carbohydrates and should not be limited to eating only jelly, soups and semolina. Eating food 5-6 times in small portions allows you to realize its “anti-acid” effect.
– in case of hypersecretion, antacid pharmaceuticals and those that suppress secretory function are prescribed;
– in case of secretory insufficiency, replacement therapy is carried out;
– pharmaceutical preparations of pancreatic enzymes are recommended for use only in cases of confirmed exocrine pancreatic insufficiency, one of the manifestations of which is steatorrhea;
– disturbances of gastroduodenal motility (insufficient peristalsis and decreased gastric tone) are eliminated by prescribing prokinetic pharmaceuticals;
– for severe pain, antispasmodic medications are used;
– for gastritis with insufficient secretory function, medications that stimulate appetite (bitterness) are prescribed;
– in some cases, with increased excitability of the central nervous system, sedatives and tranquilizing drugs are prescribed;
– surgical treatment is indicated for patients with antral rigid gastritis.
Type A gastritis - no specific treatment has been developed; in the case of a progressive course, unchanged secretory function and immune disorders, short-course glucocorticoid therapy is used.
In case of moderate secretory insufficiency, table No. 2 according to Pevzner is prescribed; stimulating and replacement therapy with hydrochloric acid pharmaceuticals is used, but due to low efficiency it has been used less and less recently.
In case of megaloblastic anemia, correction is carried out with vitamin B12.
Type B gastritis - the standard treatment for this form of gastritis is Helicobacter pylori eradication in accordance with the recommendations set out in the Maastricht Agreement.
Gastritis type C - the main direction of treatment is to normalize the motility of the digestive tract and neutralize the destructive effect on the mucous membrane of bile acids, which are thrown into the stomach with duodenal contents.
Eosinophilic (allergic) gastritis – treatment consists of identifying and eliminating contact with substances that provoke allergies; treatment of the underlying disease, in which the development of a similar form of gastritis is possible.
Giant hypertrophic gastritis - a high-calorie, protein-enriched diet and antisecretory pharmacotherapy are prescribed. In the case of the development of persistent hypoproteinemia and repeated bleeding, surgical treatment is necessary.
What can and cannot be eaten with gastritis?
A necessary condition for the treatment of gastritis is adherence to an appropriate diet. The frequency of meals is carried out individually. For example, frequent split meals 5-6 times a day in some people only worsens the course of the disease and leads to an even greater release of hydrochloric acid. Permitted for use:
- soups with pureed cereals;
- low-fat varieties of fish and meat (hake, pollock, cod, chicken);
- porridge - buckwheat, oatmeal, wheat;
- boiled potatoes;
- Among dairy products, preference should be given to milk and fermented baked milk;
- eggs;
- from fruits - sweet varieties of apples, bananas.
- whole wheat bread.
During an exacerbation, it is necessary to follow a diet for at least one month.
You should avoid using:
- coffee;
- pickles;
- chips;
- fried foods;
- hot seasonings;
- carbonated drinks;
- sweets, cakes, pastries;
- sour juices and fruits.
In case of low acidity, the following are contraindicated:
- fatty fish and meats (pork, lamb, mackerel, etc.);
- salo;
- raw vegetables (radish, cabbage, carrots);
- nuts.
Prevention
Primary prevention
Primary prevention should include normalizing lifestyle, organizing multiple dietary meals, limiting negative effects on the stomach (smoking, drinking alcohol, pharmaceuticals), and minimizing the influence of harmful factors of production and the environment.
Great importance is given to the timely detection and regular treatment of pathological conditions that can cause chronic gastritis; complete cure of acute gastritis, intestinal infections, helminthiases, chronic diseases of the liver and biliary tract, pancreas.
It is not advisable for healthy people to eradicate Helicobacter pylori even if it is detected.
Primary prevention of autoimmune gastritis and special forms of chronic gastritis has not been developed.
Secondary prevention
Secondary prevention of chronic gastritis involves a course of Helicobacter pylori eradication, which is mandatory for all Helicobacter pylori-positive patients with chronic gastritis.
Prevention of exacerbations of reflux gastritis involves multiple meals in small portions (5-6 times a day), exclusion of overeating and causes that may be accompanied by an increase in pressure in the abdominal cavity (constipation, flatulence, tight belts, significant physical activity accompanied by muscle tension in the anterior abdominal wall ).
Patients are recommended sanatorium-resort treatment with the use of mineral waters, nutritional therapy, balneo- and climate therapy, and physiotherapeutic methods of treatment.
Patients with chronic gastritis need clinical observation with preventive examinations 2 times a year, selection of treatment and determination of further tactics for the use of therapeutic measures.
www.piluli.kharkov.ua