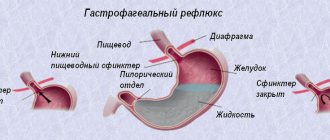
Among other gastroenterological diseases, gastroesophageal reflux disease (GERD) is one of the most common. This disease not only significantly reduces a person’s quality of life, but can lead to serious complications, such as esophageal cancer. Gastroesophageal reflux disease develops due to the backflow of stomach contents into the esophagus.
With GERD, symptoms are a consequence of the irritating effect of gastric contents on the mucous membrane of the lower esophagus. The damaging effect is caused by acid (acid reflux) or bile (alkaline reflux). The main complaint with this condition is heartburn, but other symptoms of esophageal irritation, as well as extra-esophageal manifestations of the disease, may occur.
At CELT you can get advice from a gastroenterologist.
- Initial consultation – 4,200
- Repeated consultation – 3,000
Make an appointment
Causes of gastroesophageal reflux disease
The term “gastroesophageal reflux disease” (GERD) has recently emerged and to a certain extent has replaced the previous names “reflux esophagitis” and “reflux disease”.
Although these terms are synonymous, the new name “gastroesophageal reflux disease” is more complete, since it includes a characteristic symptom complex caused by the reflux of acidic gastric contents into the esophagus. In this case, not only the reflux itself matters, but also the ability of the esophagus to free itself and cleanse itself of such an irritant. This phenomenon is called esophageal clearance. It is believed that with normal clearance of the esophagus, single refluxes do not lead to gastroesophageal (gastroesophageal) reflux disease. If the clearance of the esophagus decreases, in response to the periodic intake of acidic stomach contents, its mucous membrane quickly becomes inflamed.
A decrease in the tone of the lower esophageal adductor muscle is also of great importance, which is due to the frequent development of gastrin insufficiency in this disease. Gastrin is an important hormone of the stomach; it performs a general trophic function, regulates the tone of the closing muscles, and gastric secretion. The mechanism of gasgreen formation is disrupted in peptic ulcer disease, and reflux esophagitis develops, as a rule, in many such patients.
The mechanism of gastroesophageal reflux disease is now being clarified, taking into account the role of nitric oxide. Most clinicians interpret gastroesophageal reflux disease as varying degrees of damage to the mucous membrane of the distal esophagus, accompanied by characteristic clinical symptoms and resulting from constant pathological reflux of gastric duodenal contents into the lumen of the esophagus.
According to modern concepts, gastroesophageal reflux disease is considered as a consequence of impaired motility of the esophagus and stomach. Of key importance in the development of gastroesophageal reflux disease is a decrease in the anti-reflux barrier, a decrease in the tone of the lower esophageal closure and esophageal clearance, an increase in episodes (number) of its relaxations and an increase in intragastric pressure. Additional factors that create conditions for the development of gastroesophageal reflux disease are aggressive components of gastric contents ( hydrochloric acid, pepsin, bile acids, pancreatic enzymes trypsin and phospholipase) against the background of decreased resistance of the esophageal epithelium.
Gastroparesis, decreased saliva production (Sjögren's disease), and impaired cholinergic innervation of the esophagus are important.
A special role in the development of gastroesophageal reflux disease is assigned to the microorganisms Helicobacter pylori. Drinks containing caffeine (coffee, tea, cocoa, Coca-Cola and Pepsi-Cola), juices (especially citrus fruits), alcohol, milk, tomatoes, horseradish, onions, garlic, pepper and other spices increase the acid-forming function of the stomach and reduce tone inferior esophageal closure.
Gastroesophageal reflux disease should be distinguished from secondary reflux esophagitis, which is observed in peptic ulcers, slippery hiatal hernia after gastric surgery, scleroderma, esophageal cancer, etc.
The main symptoms of gastroesophageal reflux disease are heartburn and regurgitation (belching), they appear at least 2 times a week for 4-8 weeks or more. Patients also complain of a feeling of compression in the epigastric region, which occurs 15-40 minutes after eating and is provoked by the consumption of foods that stimulate the synthesis of hydrochloric acid in the stomach and bile in the liver. These products include:
- fried foods,
- spicy dishes,
- juices,
- alcohol,
- dry red wines,
- carbonated drinks such as Coca-Cola, Pepsi-Cola, Fanta,
- coffee,
- chocolate,
- cocoa,
- radish,
- oil in large quantities.
Often patients with gastroesophageal reflux disease complain of pain behind the sternum radiating to the neck, lower jaw, left shoulder and arm, under the left shoulder blade. In the latter case, differential diagnosis with coronary heart disease (angina) should be carried out. Chest pain in gastroesophageal reflux disease is associated with:
- food consumption, in particular overeating,
- low head position during sleep.
Usually stops after drinking antacids or alkaline mineral waters (Polyana Kvasova, Polyana Kupel, Luzhanskaya).
Such complaints are usually provoked by physical activity, frequent bending of the body, fullness of the stomach with liquid, fatty, sweet foods, alcohol, and intensify at night. The entry of the contents of the esophagus into the lumen of the bronchi can lead to bronchospasm, bronchoaspiration Mendelssohn syndrome (for a fatal case, it is enough for 2-4 ml of acidic gastric juice to enter the bronchial tree).
Symptoms of GERD
The typical clinical picture of the disease is characterized by heartburn, which worsens when bending over, physical activity, after a heavy meal and in a lying position, belching with a sour or bitter taste. May be accompanied by nausea and vomiting. Depending on the severity of the course, dysphagia is noted - a swallowing disorder, which can be primary (as a result of impaired motor skills) or be a consequence of the development of strictures (narrowings) of the esophagus.
GERD often occurs with atypical clinical manifestations: chest pain (usually after eating, worsening when bending over), heaviness in the abdomen after eating, hypersalivation (increased salivation) during sleep, bad breath, hoarseness. Indirect signs indicating a possible pathology are frequent pneumonia and bronchospasms, idiopathic pulmonary fibrosis, a tendency to laryngitis and otitis media, and damage to tooth enamel. GERD, which occurs without severe symptoms, is of particular danger in terms of the development of severe complications.
Few serious illnesses occur without symptoms, and reflux esophagitis is no exception. Gastroesophageal reflux itself cannot always be identified, so the main symptom by which reflux esophagitis is determined is heartburn. It occurs in 80% of patients. Also, reflux esophagitis is often accompanied by belching, sometimes with a sour taste (with a reflux of bile from the duodenum - bitter), and sometimes chest pain, especially after eating, and excessive salivation at night.
There are also a number of symptoms that most people do not associate with GERD, but yet they are directly related to it. The fact is that gastroesophageal reflux can cause particles of gastric contents - food debris and aggressive gastric juice - to enter the respiratory tract and oral cavity.
Therefore, if a patient has symptoms such as chronic bronchial asthma and other diseases of the lower respiratory tract, chronic pharyngitis and laryngitis, permanent dental diseases, such as caries, then this is a reason to contact a gastroenterologist.
Children's digestive organs are designed to withstand frequent exposure of gastric contents to the surface of the esophagus, since gastroesophageal reflux and regurgitation of food are common in children. However, if regurgitation, regurgitation and vomiting occur too frequently in infants, this may be a sign of improper functioning of the lower esophageal sphincter. Older children may complain of heartburn, a burning sensation in the abdominal cavity.
How to treat gastroesophageal reflux disease?
Drug treatment of gastroesophageal reflux disease is divided into 2 phases: initial (initial) and secondary.
In the first phase, a transit pump inhibitor (lamprazole, pantoprazole) is prescribed, the purpose of which is to heal erosive esophagitis and completely overcome clinical manifestations. Initial treatment should last 4 weeks. Subsequently, a transfer is made to a dose that maintains remission for the next 4 weeks. For erosive GERD, the duration of initial treatment should be 4-12 weeks, followed by one of the long-term therapy regimens. The generally accepted treatment strategy with antisecretory drugs is to initially prescribe double doses of proton pump inhibitors for 4-8 weeks, followed by long-term treatment.
The second phase is long-term treatment, the goal of which is to achieve remission. Carried out in 3 options:
1) long-term daily use of proton pump inhibitor in anti-relapse doses;
2) “on-demand” therapy: use of a proton pump inhibitor in full dose in a short 3-5-day course in case of widespread symptoms;
3) “weekend” therapy: use of a proton pump inhibitor in an anti-relapse dose.
If initial treatment is ineffective, esophagoscopy and pH monitoring should be performed within 2 weeks. If monitoring indicates a nocturnal “breakthrough” of acidity, then the patient should be prescribed famogidine or renitidine in addition to a double dose of a proton pump inhibitor. If reflux is bile, then ursodeoxycholic acid (ursosan) or a cytoprotector is indicated. To improve the resistance of the mucous membrane of the esophagus, a decoction of flax seeds (1/3 cup each), sucralfate (Venier), Maalox, phosphate gel, Gelusil, Gestal, Pee-Khoo is recommended.
The most effective is Maalox. Such patients are prescribed prokinetics - cisapride or cerucal (metoclopramide), which increase the tone of the lower esophageal closure, reduce the severity of gastroesophageal reflux and reduce acidification of the esophagus.
Positive results are obtained from sea buckthorn and rosehip oils. The dose is selected individually - from 1 teaspoon at night to 1 teaspoon 3-4 times a day.
Endoscopic and surgical treatment of GERD is recommended for patients in the following cases:
- the need for long-term drug therapy;
- insufficient effect of drug therapy;
- diaphragmatic hernia, large volume of reflux;
- complications - bleeding, strictures, Barrett's esophagus, esophageal cancer;
- personal wishes of the patient.
Treatment effectiveness criteria:
- healing of erosive lesions of the esophagus,
- disappearance of heartburn,
- improving quality of life.
The recurrence rate during the first year after successful completion of treatment is 39-65% for erosive GERD.
How does a doctor diagnose reflux esophagitis?
Any diagnosis of the disease should begin with a consultation with a doctor. The doctor will clarify the nature of the pain, its frequency and duration. The doctor can also find out the patient’s dietary habits to determine his lifestyle. After the conversation, the doctor may examine the tongue.
Note! Fibroesophagogastroduodenoscopy (FEGDS) is considered one of the most effective methods for diagnosing this disease.
With gastrointestinal reflux, the tongue may be coated with a white coating. To rule out other diseases, the doctor should palpate the abdomen.
If no painful sensations are detected, then the patient is referred for an instrumental examination.
Using a probe and a camera at its end, you can see a clear picture of the gastrointestinal tract disease. With reflux, the lining of the esophagus will be red. In some cases, your doctor may order tissue to be removed from the area for further testing.
Also used for diagnosis:
- x-ray,
- daily pH-metry (determination of acidity level),
- esophagomanometry (determining the functionality of the lower esophageal sphincter),
- ECG (to rule out heart disease),
- Chest X-ray (to rule out lung diseases).
Taken together, all diagnostics will allow you to see an accurate picture of the course of the disease. The main thing is to see a doctor in time.
What diseases can it be associated with?
The nature of gastroesophageal reflux disease is explained by impaired motility of the esophagus and stomach; the disease develops against the background of a reduced antireflux barrier, reduced tone of the lower esophageal closure and esophageal clearance.
An increased risk of experiencing symptoms of gastroesophageal reflux disease are disturbances in the production of digestive hormones (gastrin) and pancreatic enzymes against the background of a decrease in the resistance of the esophageal epithelium.
Gastroparesis, decreased saliva production (Sjögren's disease), and impaired cholinergic innervation of the esophagus are important. GERD is most likely to occur in a person who is a carrier of Helicobacter pylori, who also has a higher risk of developing gastric ulcers.
Treatment of gastroesophageal reflux disease at home
The most important condition for the treatment of gastroesophageal reflux disease is lifestyle changes:
- quitting smoking and drinking alcohol,
- weight loss,
- avoiding a horizontal body position after eating and during sleep,
- refusal to wear corsets, bandages, or anything that increases intra-abdominal pressure.
It is important to change the mode and nature of nutrition:
- overeating must be avoided
- Avoid eating at night,
- Avoid lying down after eating
- Minimize fat-rich foods in your diet: milk,
- cream,
- goose meat
- duck,
- pork,
- lamb,
- coffee,
- tea,
- coca cola,
- citrus fruits and juices from them,
- tomatoes,
- garlic,
- dry red wines.
Patients with long-term heartburn (10 years or more), erosive forms of GERD, and Barrett's esophagus are subject to clinical observation.
In the case of Barrett's esophagus with low-grade dysplasia, proton pump inhibitors should be prescribed at a double dose for at least 3 months, followed by a reduction in the dose to the standard dose. Endoscopic monitoring with biopsy should be performed annually. For high-grade dysplasia, another endoscopic examination with multiple biopsies from altered areas of the mucous membrane should be performed. For a patient with Barrett's syndrome and high-grade dysplasia, endoscopic mucosal resection or surgical esophagotomy is recommended.
Proton pump inhibitors (blockers)
Proton pump inhibitors are currently the most effective medications for GERD. Their advantages when used during this pathological process:
- modern proton pump blockers are more likely to eliminate pain near the chest;
- normalize the level of acidity of gastric juice, and can also maintain these indicators throughout the day;
- long-term use of blockers has a beneficial effect on the healing of esophageal erosions in the vast majority of situations;
- with proper, constant use of such medications, it is possible to count on long-term stable remission (no exacerbations).
Because of such positive characteristics, experts prefer this drug directly. Representatives of this subgroup of medications include:
- "Omeprazole";
- "Rabeprazole";
- "Lansoprazole";
- "Esomeprazole";
- "Pantoprazole."
The dosage of medications is adjusted depending on the stage of development of GERD or the presence of adverse effects.
What drugs are used to treat gastroesophageal reflux disease?
- pantoprazole - 20 mg 2 times a day or 40 mg 1 time a day at night, course of treatment is 4 weeks; maintenance dose of 20 mg at night for the next 4 weeks;
- famotidine - 20 mg 2 times a day before breakfast and dinner;
- ranitidine - 150 mg 2 times a day;
- sucralfate - 500 mg 1-1.5 hours after meals 4 times a day;
- Maalox - 1-2 packets 3-4 times a day;
- metoclopramide - 10-20 mg 3-4 times a day.
Los Angeles classification
This classification was proposed in the last century in Los Angeles. It has its own characteristics. The Los Angeles classification proposes to define the disease by the parameter of how extensive the lesion is.
Interesting! The nuances of using the drug Pepsan-R: cheap analogues
| Damage level | Peculiarities |
| A | The mucous membrane is damaged in one or more places at the same time. The size of the ulcer does not exceed 5 mm. In this case, the wound does not spread beyond one fold. |
| B | The size of the ulcer increases. It becomes larger than 5 mm, but does not go beyond the fold. |
| C | The pathological process in this case already affects several folds of the mucous membrane. The affected area expands and is more than 8 mm. The esophagus is already 75% affected. |
| D | The tissue of most of the organ is damaged. |
With any type of lesion according to this classification, various complications are possible.
Any classification of GERD by ICD code or other parameters provides for easier diagnosis for doctors. They have the opportunity to quickly begin treatment and eliminate the cause of the pathology.
Treatment of gastroesophageal reflux disease with traditional methods
Folk remedies have proven positive in the treatment of gastroesophageal reflux disease. Discuss with your doctor the appropriateness and dosage of folk remedies in your specific case. It can be:
- decoction of flax seeds - 1 tsp. Brew flaxseeds in a glass of boiling water, leave for 5 minutes over low heat, leave for another half hour, strain; take ⅓ glass three times a day before meals, warm;
- herbal mixture - combine 4 parts of St. John's wort herb, 2 parts each of calendula officinalis flowers, plantain leaves, licorice roots, calamus and 1 part each of tansy and peppermint flowers; 1 tsp pour a glass of boiling water over the resulting collection, strain after half an hour and take ⅓ glass three times a day before meals, warm;
- sea buckthorn and rosehip oils - the dose is selected individually from 1 teaspoon at night to 1 teaspoon 3-4 times a day.
Treatment of gastroesophageal reflux disease during pregnancy
Treatment of gastroesophageal reflux disease in pregnant women should be carried out under the supervision of a specialized specialist. If GERD manifests itself during pregnancy, then there is a high probability that the disease will be temporary, and the symptoms will disappear after childbirth.
At the initial stage of GERD during pregnancy, the doctor will recommend lifestyle changes, then herbal medicine, and only with extremely uncomfortable symptoms, drug treatment is appropriate. Basically, treatment of GERD in pregnant women is symptomatic, improving the quality of life and well-being of the expectant mother.
Prevention
Primary preventive measures for GERD consist of following the specialist’s instructions regarding an active lifestyle (quitting smoking, drinking alcoholic beverages).
It is prohibited to use medications that disrupt the functioning of the esophagus and that reduce the protective characteristics of its mucosa.
Secondary preventive measures are to reduce the frequency of relapses and prevent progression of the disease.
A mandatory component of secondary preventive measures for GERD is adherence to the above instructions for primary prevention and non-drug therapy for such a disease.
In order to prevent exacerbations, if there is no esophagitis or a mild form of esophagitis is observed, timely treatment “on demand” will retain its importance.
Despite the fact that some drugs can aggravate the symptoms of GERD, the use of others causes drug-induced esophagitis, a disease during which the same symptoms appear as with GERD, but not due to reflux.
Drug-induced esophagitis occurs when a pill is swallowed but does not reach the stomach because it is stuck to the wall of the esophagus.
If GERD is not eliminated in a timely manner, it is fraught with adverse consequences. In this regard, it is necessary to consult a doctor and choose the optimal treatment.
Which doctors should you contact if you have gastroesophageal reflux disease?
- Gastroenterologist
When examining a patient with gastroesophageal reflux disease, dry mouth (xerostomia), hypertrophied fungiform papillae of the tongue (the result of gastric hypersecretion), a positive left or right phrenicus symptom, and signs of laryngitis (hoarseness) are revealed.
The diagnosis of gastroesophageal reflux disease is confirmed x-ray - in the presence of reverse flow (reflux) of the contrast agent from the stomach into the esophagus, the results of round-the-clock pH monitoring in the esophagus (at a normal pH of 5.5-7 pH in a patient with GERD for 5 minutes - 1 hour or more - less than 4).
However, the gold standard for diagnosing gastroesophageal reflux disease is the endoscopic method. Classification of esophageal lesions according to esophagoscopy:
- 0 degree - the mucous membrane of the esophagus is intact;
- I degree of severity - individual erosions that do not merge with each other and/or erythema of the mucous membrane of the distal esophagus;
- II degree of severity - erosions that merge with each other, but do not spread to most of the mucous membrane of the lower third of the esophagus;
- III degree of severity - erosive lesions of the lower third of the esophagus, erosions merge and spread to the entire surface of the mucous membrane of the distal esophagus;
- IV degree of severity - erosive and ulcerative changes or complications (stricture of the esophagus, bleeding, metaplasia of the mucous membrane with the formation of an endoscopic picture of a “pavement” and the formation of Barrett’s esophagus).
Diagnostic criteria for suspected GERD:
- typical clinical symptoms: heartburn and sour belching;
- test with a proton pump inhibitor: the effectiveness of a 5-7-day course of using modern proton pump inhibitors, such as esomeprazole (rabeprazole, pantolrazole);
- endoscopic confirmation of esopharitis;
- positive results of 24-hour esophageal pH monitoring (pH less than 4, duration of at least 5 consecutive minutes).
Additional diagnostic methods:
- general blood test and biochemical blood test;
- Helicobacter pylori test (breath test);
- biopsy - indicated if endoscopy raises suspicion of intestinal metaplasia, in patients with ulcerative lesions of the esophagus and/or its stenosis, if non-reflux etiology of esophagitis is suspected).
What role does psychosomatics play in development?
Even Cicero in the 1st century BC. It has been proven that all diseases of the body arise from pain in the soul. The psychological state plays an important role not only in terms of treating diseases, but also at the stage of their onset. Diseases of the gastrointestinal tract are often called diseases associated with psychosomatics.
American psychotherapist Milton Erickson claims that every disease initially arises in our head , and only then does it manifest itself on the body. As for reflux esophagitis, he is confident of its psychosomatic origin. The main problem of this disease is the direction of the stomach contents not towards the intestines, but towards the esophagus. That is, the wrong direction of processed food occurs.
This condition may occur as a result of changes in gastric motility. Often, the appearance of gastro-food reflux at the subconscious level is due to a person’s desire to turn back time in order to correct some actions in his life.
Psychosomatic disorders are treated by a psychotherapist. His arsenal contains many different treatment methods. The most striking are: NLP, art therapy, hypnosis, psychoanalysis, family therapy, etc.
Treatment of other diseases starting with the letter - g
| Treatment of sinusitis |
| Treatment of galactorrhea |
| Treatment of pulmonary hamartoma |
| Treatment of lung gangrene |
| Treatment of gastritis |
| Treatment of hemolytic leukopenia |
| Treatment of hemorrhagic stroke |
| Treatment of hemorrhoids |
| Treatment of pulmonary hemothorax |
| Treatment of hemophilia |
| Treatment of hemochromatosis |
| Treatment of genital herpes |
| Treatment of hepatitis G |
| Treatment of hepatitis A |
| Treatment of hepatitis B |
| Treatment of hepatitis D |
| Treatment of hepatitis E |
| Treatment of hepatitis C |
| Treatment of hepatosis |
| Treatment of hepatorenal syndrome |
| Treatment of hepatocellular carcinoma |
| Treatment of herpes |
| Treatment of hydronephrosis |
| Treatment of pulmonary hydrothorax |
| Treatment of gynecomastia |
| Treatment of overactive bladder |
| Treatment of hyperbilirubinemia |
| Treatment of endometrial hyperplasia |
| Treatment of hyperprolactinemia |
| Treatment of hypertensive crisis |
| Treatment of hypertension |
| Treatment of tonsil hypertrophy |
| Treatment of hypospadias |
| Treatment of hypothyroidism |
| Treatment of hypothyroid coma |
| Treatment of glycogenosis |
| Treatment of worms |
| Treatment of glomerulonephritis |
| Treatment of ulcers on tonsils |
| Treatment for tension headaches |
| Treatment of gonorrhea |
| Treatment of liver granuloma |
| Treatment of nail fungus |
| Flu treatment |
The information is for educational purposes only. Do not self-medicate; For all questions regarding the definition of the disease and methods of its treatment, consult your doctor. EUROLAB is not responsible for the consequences caused by the use of information posted on the portal.