Stages
Infertility may develop
The disease is easier to treat in the early stages of its formation. In a later period, there is a high probability of complications, as well as chronicity of the process.
Modern classification distinguishes 4 stages of the disease.
- Within the retrovaginal area there are single lesions. In this case, adenomyosis is very often diagnosed, since there is no growth into the deep layers of the uterus.
- Widespread deep lesions, more than two in number. The vagina and uterus are affected. The formation of cystic formations begins.
- The number of lesions is increasing. There is growth into the rectal area.
- Formation of adhesions. In addition, the peritoneum is affected
.
Severe infiltrative endometriosis develops
. At this stage, surgical intervention up to removal of the uterus is indicated.
Clinic
If a woman is diagnosed with retrocervical endometriosis, what it is needs to be figured out. The majority of gynecological pathologies have related symptoms, so certain unpleasant signs should prompt the girl to visit a gynecologist. Many experts say that retrocervical endometriosis must be differentiated from cancer.
Retrocervical endometriosis with cell proliferation in the rectum. Source: studfiles.net
Since oncological pathologies occur without obvious signs for many years, it is very difficult to identify them in the early stages. Retrocervical endometriosis itself has the following symptoms:
- Patients feel pain in the rectum, perineum, external genitalia, vagina and lumbosacral area of the back;
- According to the nature of the manifestation, the pain can be sharp, shooting, or intensifying during intimacy and during defecation;
- During menstrual bleeding, a large amount of mucus is released;
- There are streaks of blood in the stool;
- If infiltration of the posterior vaginal vault has occurred, then during a gynecological examination the doctor will see small blue areas from which blood oozes during physical exertion or overexertion.
Retrocervical endometriosis has pronounced symptoms, and since the disease progresses rapidly, the likelihood that it is developing oncology is minimal. However, it is precisely this feature of the pathology that leads to the patient temporarily losing her ability to work.
Causes
For the development of the retrocervical form of endometriosis, it is necessary that blood containing endometrial particles enter this area.
The following can lead to this:
- complicated childbirth;
- medical and surgical abortions;
- frequent infectious diseases of the reproductive system;
- incorrect placement of the spiral;
- invasive gynecological procedures.
Some experts talk about the high role of heredity in the development of this form of the disease. According to studies, the risk of developing endometriosis is higher in those women whose close relatives suffered from this form of the disease.
Read about the compatibility of chronic endometritis and pregnancy.
Symptoms
Signs of endometriosis, including its retrocervical form, may be as follows:
- severe pain syndrome (localized in the lower abdomen);
- heavy discharge during menstruation, which also becomes longer;
- discomfort during sexual intercourse.
Expert review Olga Borovikova The clinical picture of the disease may not appear immediately and directly depends on the severity of the process. If the nature of your periods changes or pain occurs, you should seek help from a gynecologist.
Diagnostics
Based on clinical manifestations, the doctor can only suspect the disease. To confirm assumptions, the gynecologist needs to use instrumental research methods.
Diagnosis of endometriosis is carried out in several main stages.
- Patient interview. Studying the patient's life history and illness plays a very important role
. This allows us to identify risk factors for the disease and clarify its clinical picture. - Inspection. A gynecological examination may be accompanied by a smear and colposcopy.
- Carrying out instrumental examination techniques. This may include transvaginal ultrasound, colonoscopy, and abdominal ultrasound. If the doctor suspects damage to the ureter, urography is performed.
If the doctor seems to have insufficient information obtained by these methods, an MRI may be prescribed.
Magnetic resonance imaging
Caution! The procedure allows you to clearly determine the location and severity of the disease. This is achieved due to the fact that the device does not just give a superficial image of the organ, but, as it were, removes it in layers. Therefore, even in the earliest stages of endometriosis, the extent of the damage can be clearly assessed.
The only disadvantage of the method is its high cost. Specialists resort to it in cases where, despite a clear clinical picture, it is not possible to visualize the process using instrumental examination methods.
Ultrasound
If MRI is used quite rarely, then this procedure is performed on every woman diagnosed with endometriosis.
If suspected, the study is carried out using two methods:
- transabdominal;
- transvaginally.
Transvaginal ultrasound is more informative. In this case, a specialist inserts a sensor into the vagina, which will display a photo in real time on the device’s screen.
. The specialist evaluates a number of indicators.
If the disease is present, the following changes may be detected:
- uneven contours of the uterus, as well as changes in the size of the organ;
- changes in the structure of the cervical canal;
- hyperechoic formations, which are foci of the disease;
- cysts.
Ultrasound is performed not only to diagnose the disease, but also to evaluate the effectiveness of treatment.
The main thing is proper examination
Special examination methods
- Ultrasound of the pelvic organs (more informatively, transvaginal or transrectal scanning) has become widespread for diagnosing endometriosis. The method provides reliable diagnosis of adenomyosis, endometrioid cysts, allows one to suspect damage to the rectovaginal septum, but does not detect superficial implants on the peritoneum. Transvaginal ultrasound in the first 3 days after ovulation in the vast majority of cases diagnoses “small” forms of retrocervical endometriosis and endometriosis of the uterosacral ligaments (patent 2008102542/14, Lobanova O.G., 2008).
- Colposcopy can detect endometriosis of the vagina and cervix. If this study reveals pathological changes in the cervix, a cytological examination is required. This method is simple and does not require large material costs, but it is very informative. To make a diagnosis, histological examination data during targeted biopsy are crucial.
- Hysteroscopy should be considered an additional method for diagnosing internal endometriosis. Adenomyosis is characterized by uneven contours of the uterine cavity, difficulties in its expansion, and the surface of the walls of the uterine cavity in the form of crypts. Sometimes clusters of chaotically located trabeculae with cells between them are visible, from which dark bloody thick fluid or small bluish cysts are released. Additional information can be provided by targeted or multifocal trephine biopsy of the myometrium during hysteroscopy.
- Hysterosalpingography (x-ray contrast image of the uterus) to confirm adenomyosis or internal endometriosis has now practically lost its relevance.
- Computed tomography (CT) and/or magnetic resonance imaging (MRI) make it possible to accurately determine the nature of the pathological process, its localization, involvement of neighboring organs, and clarify the anatomical state of the pelvic organs. All this is important for planning the approach and extent of surgical intervention, as well as for dynamic monitoring during conservative therapy.
- If there is suspicion of involvement of the intestines and bladder in the pathological process, it is advisable to perform sigmoidoscopy, colonoscopy, excretory urography and/or cystoscopy as indicated.
- Diagnostic laparoscopy is the leading method of instrumental diagnosis of external endometriosis, allowing to visualize even the initial manifestations of pathology. During laparoscopy, foci of endometriosis can be detected on the peritoneum of the pelvic cavity and ovaries, endometriotic ovarian cysts (endometriomas), endometriosis of the rectovaginal septum, sometimes spreading to the walls of the rectum or sigmoid colon , endometriosis of the bladder and appendix, adhesions. Defects and pockets of the peritoneum indirectly confirm the diagnosis of endometriosis (histologically - in 60-80% of cases). There are more than 20 different types of superficial foci of endometriosis on the pelvic peritoneum. There are red lesions, fire-like lesions, hemorrhagic and transparent vesicles, vascularized polypoid or papular lesions, wrinkled lesions, classic black lesions, white lesions, scar tissue with or without pigmentation; atypical lesions, other lesions if they are confirmed by histological examination. It has been established that red lesions are the most active stage of development. Petechial and vesicular lesions are more common in adolescents and disappear completely by age 26. With increasing age, red hemorrhagic foci are replaced by pigmented and fibrous foci, and in older women black and white cicatricial foci predominate. Laparoscopy allows us to identify signs characteristic of internal endometriosis: a “marble” pattern and pallor of the outer cover of the uterus, a uniform increase in its size or with focal and nodular forms - sharp thickening of the anterior or posterior wall of the uterus, deformation of the wall by a node of adenomyosis. Laparoscopic signs of an endometrioid cyst - ovarian cysts with a diameter of no more than 12 cm; adhesions with the lateral surface of the pelvis and/or with the posterior leaf of the broad ligament; thick chocolate-colored contents. The accuracy of diagnosing endometrioid cysts during laparoscopy reaches 98-100%.
Retrocervical endometriosis is characterized by pain, gluing (soldering) of tissues of the retrouterine space, sometimes involving the walls of the rectum or sigmoid colon in the infiltrative process, infiltration of the rectovaginal septum, distal ureters, isthmus region, uterosacral ligaments, and parametrium.
Drugs
Several groups of drugs are used to treat retrocervical endometriosis:
- combined oral contraceptives;
- gonadotropin-releasing hormone antagonists;
- progestins.
The first group includes the following funds:
- Jess;
- Yarina;
- Claira;
- Janine.
Progestins used for treatment include the following:
- Orgametril;
- Visanne;
- Duphaston.
Difelin, Buserelin, Zoladex belong to the group of gonadotropin-releasing hormone antagonists and can also be used to treat endometriosis. Learn about the causes and treatment of uterine endometriosis.
Treatment
- At the first stage of treatment for retrocervical endometriosis, excision of the endometriosis focus through the vagina is prescribed for diagnostic and therapeutic purposes. Subsequently, the taken material is necessarily sent for histological examination.
- In stages I and II of the disease, the focus of endometriosis is excised within healthy tissue, followed by the application of separate kengut sutures to the vaginal wall. Before applying a suture, it is advisable to perform cryodestruction (exposure to the lesion with liquid nitrogen) of the endometriosis bed, thereby preventing further spread of infiltrates.
- In stage III , a posterior colpotomy is indicated (an incision in the vaginal wall and the underlying vaginal-rectal tissue). Then, foci of endometriosis are excised from the uterosacral ligaments, the serous membrane of the rectum, and laser and cryo-treatment of the area of the uterosacral ligaments is also performed. At the same time, an examination of the pelvic organs, peritoneum and rectouterine cavity is performed.
- At stage IV , young patients are shown diagnostic excision of the endometriosis lesion in order to clarify the diagnosis. Then massive treatment is carried out with hormonal agents from the group of norsteroid gestagens (norgestrel, levonorgestrel, dienogest, etc.), antigonadotropins (danol) or gonadotropin-releasing hormone agonists (lucrin, diferelin, zoladex).
Women with retrocervical endometriosis are also prescribed sanatorium treatment, sedative therapy, baths with radon, iodine and bromine, and symptomatic treatment.
Retrocervical endometriosis must be distinguished from ovarian and rectal cancer.
The prognosis if a woman consults a doctor in a timely manner and receives adequate treatment is favorable in 65% of cases.
Operation
Indications for surgery may include the following:
- a common process affecting distant organs;
- severe pain that cannot be treated;
- disorders of the urinary system;
- adhesive processes.
The extent of surgical treatment depends on the stage of endometriosis.
- In the first stage, the affected areas are excised. In this case, the integrity of the organs is completely preserved and the intervention will not affect the patient’s life in any way.
- In the second stage, partial removal of vaginal tissue is possible.
- The third stage also requires excision of the affected areas of the rectum.
- The fourth stage of the disease is very difficult. In this case, specialists may perform a hysterectomy.
Observation The uterus is not always removed. This is a very serious intervention, which is carried out in extremely severe cases.
. The price of surgical treatment depends on the severity of the process, as well as the clinic in which it will be performed. On average, the price for laparoscopy is 25,000 rubles.
Laparoscopy in the treatment of endometriosis
Laparoscopy is the preferred surgical approach (the “gold standard”) for the treatment of endometriosis of any severity. Advantages of laparoscopic approach:
- minimal tissue trauma,
- the period of postoperative rehabilitation is reduced,
- lower percentage of formation of postoperative adhesions,
- better visualization of the affected tissues thanks to the optical magnification of the endoscope camera, hence more painstaking and skillful work of the surgeon.
When performing laparoscopy, it is possible to remove endometrioid cysts and nodes, cauterize or excise foci of endometriosis on the pelvic peritoneum, separate adhesions, restore the patency of the fallopian tubes and normal pelvic anatomy, and introduce an anti-adhesion gel barrier. It is even possible to remove the uterus and appendages using surgical laparoscopy if the surgeons have the appropriate qualifications.
Abdominal (abdominal) access with an incision into all layers of the abdominal wall is still necessary in cases of extensive organ damage and the need to excise endometriosis nodes from the walls of the rectum and bladder. Here, abdominal surgery is safer for the patient and the doctor.
In patients with severe pain, menstrual dysfunction, in the absence of effect from laparoscopic organ-sparing surgery, but wishing to preserve the uterus, cases of ablation of the uterosacral nerve (LUNA operation) are also used. At the same time, the effect of reducing pain from denervation is described as insignificant.
Surgical treatment is indicated for patients with identified cystic forms of endometriosis, with intractable chronic pelvic pain syndrome, with infertility, with nodular forms of the disease, when adjacent pelvic organs are involved in the process with impaired function and pain.
The goal of surgical treatment is to remove all foci of endometriosis, while observing the principle of organ preservation whenever possible. Removal of disease foci is the main factor in reducing pain in the postoperative period in patients. Also during the operation, adhesions are separated and the normal anatomy of the pelvic organs is restored.
Why is it dangerous?
The main danger of endometriosis is infertility, which it can lead to. With this pathology, pregnancy is difficult and there is always a risk of miscarriage.
The following complications develop against the background of endometriosis:
- increased risk of neoplasms;
- severe anemic syndrome due to blood loss;
- neurological disorders due to pain attacks.
The severity of possible complications requires a quick diagnosis and timely initiation of treatment measures.
Pregnancy
Conceiving with endometriosis is not uncommon. If women do not take COCs, which can be prescribed for the retrocervical form, they can become pregnant
. The chance of this happening is quite high.
With endometriosis, the problem is not to conceive a child, the problem is to bear it. If the source of the disease has spread beyond the uterus, there is always a risk of complications. Therefore, women suffering from endometriosis need to carefully plan their pregnancy and prepare.
If retrocervical endometriosis is only discovered during pregnancy, nothing specific will have to be done. But they will not treat the disease. With a high degree of probability, delivery can be carried out by caesarean section.
In the first week after birth, drug treatment will be prescribed, which will stop the pathological process.
Types of endometriosis
Depending on the location of the process, a distinction is made between genital (damage to the genital organs) and extragenital (located anywhere outside the genital organs) endometriosis. Genital, in turn, is divided into internal (damage to the body of the uterus) and external (damage to the cervix, vagina, ovaries, fallopian tubes, pelvic peritoneum, etc.). As a rule, endometriosis takes the form of separate or merging with other tissues of small lesions (nodules, nests) of round, oval and irregular shape, the cavities of which contain dark, thick or clear liquid. Endometriotic formations can consist of many small cystic cavities (cellular structure) or acquire the character of a cyst (for example, endometrioid (“chocolate”) ovarian cyst). Non-genital (extragenital) endometriosis is found in different organs: appendix, navel, omentum, bladder, ureters, intestines, peritoneum, etc. Internal endometriosis is called uterine adenomyosis. Not to be confused with endometrial adenomatosis (polyps, precancerous process). There is retrocervical endometriosis. Adenomyosis is located in the very thickness of the endometrium. Retrocervical endometriosis is located in the tissue of the parametrium. Endometrioid “chocolate” ovarian cysts are quite common now. Sizes range from small focal formations to large cysts (10-15 cm). Endometriosis of the uterine angle occurs. The uterine angle node is visible, usually dark blue in color. Often develops after an ectopic pregnancy. Endometriosis often develops after operations on the uterus, when the endometrium is sutured with threads. Endometrial cells are pulled along with the thread and needle. Particularly favorite sites for endometriosis are the area of the uterosacral ligaments and the junction of the peritoneum of the uterus into the peritoneum of the rectum (Pouch of Douglas). Small foci of endometriosis are implanted into the peritoneum. The peritoneum in the area of the vesicouterine fold is also often affected, especially the place where the ureter enters the bladder. With endometriosis of the ovary, an endometriosis cyst forms: the ovary increases in size. This is a benign tumor that can degenerate into malignant. An endometriosis cyst puts pressure on the ureter, and if the process is left untreated for a long time, the kidneys may suffer. Posterior cervical endometriosis can manifest itself in a woman as pain during sex. It may seem like a minor medical problem, but it can lead to discord in the family due to the fact that the woman is unable to fulfill her marital responsibilities. Endometriosis of the uterus is manifested by heavy, painful periods, including dizziness and loss of consciousness. Cervical endometriosis is the most “quiet” form; it often occurs in women after treatment for cervical erosion (menstruation has passed and the endometrial cell has entered the treatment area). It manifests itself as prolonged bleeding before and after menstruation. The doctor makes a preliminary diagnosis of “endometriosis” based on complaints and ultrasound data, but it is finally confirmed after laparoscopy.
IVF for retrocervical endometriosis
The disease is not a contraindication for IVF. Only a protracted process involving distant organs can affect the procedure and requires therapeutic measures.
Expert opinion Olga BorovikovaIn order for a woman suffering from endometriosis to become pregnant after IVF, it is necessary to carefully assess the severity of the disease. The severity of the process will play a major role in this matter.
. Thus, with stage 3 or 4 endometriosis, there is a high risk of miscarriage. There is also an increased risk of bleeding and placental abruption, which are typical for IVF.
Endometriosis therapy
Treatment of the disease is prescribed by a gynecologist taking into account several factors: the severity and duration of the disease, the degree and location of the affected areas, and whether the patient has children. Therapy can be medication or surgery.
Surgical methods
Surgical treatment of enometriosis is recommended for extensive localization of the process, ovarian cysts and adhesions. It can be conservative (the uterus and ovaries are preserved, so the woman can become a mother) and radical (complete removal of the uterus).
Laparoscopic surgery may be performed. A laparoscope, an instrument with an optical element, is inserted through an opening in the abdominal cavity, thanks to which the doctor sees the organ from the inside. The operation is carried out very carefully. The doctor uses a scalpel to separate the infiltrate from the uterus and rectum. In addition, a so-called anti-adhesive barrier is introduced, since endometriotic lesions can recover.
Laser treatment scheme
If the internal genital organs are damaged, other specialists, not just gynecologists, may be involved in the operation. Foci of endometriosis can often be found in the intestines. In this case, the operation should be performed in the presence of a coloproctologist.
Drug treatment
Hormonal therapy can be used as the main method of treatment, or in combination with surgery. Women are prescribed oral contraceptives to suppress ovarian function. If the usual regimen for taking birth control pills involves a week's break between courses, then when treating endometriosis, the pills should be taken without a break, thereby artificially creating menopause. The following types of medications are used:
- Progestogens. They reduce the production of estrogen in the ovaries, thereby reducing the degree of endometrial proliferation.
- Gonadotropin-releasing hormone agonists. They are produced in the form of injections and are injected into the patient’s abdominal wall, causing the so-called “chemical castration”.
Much attention is paid to the treatment of pain syndrome, as it sharply reduces the quality of life of patients. Various non-steroidal anti-inflammatory and combined oral contraceptives are used.
Vitamin therapy
Vitamins are necessary to boost immunity, as well as to normalize metabolism in the body. To get enough microelements, you need to normalize your diet. They are found in fresh vegetables and fruits, and animal products. You can also purchase special complexes sold in pharmacies - Aevit, Askorutin, Beresh Plus and others.
Combined treatment of endometriosis
Combination treatment is a combination of hormonal therapy and surgery. Moreover, a course of hormonal medications can be taken both before and after surgery. In the first case, hormones reduce the blood supply to endometriosis lesions, so they decrease in size. Taking hormonal drugs after surgery helps to affect the affected tissues that were not touched by the surgeon. Due to this, the likelihood of relapse of the disease is reduced.
Folk remedies
Traditional therapy can be combined with folk remedies. However, using only folk remedies to treat endometriosis, the disease cannot be cured. You can prepare the following:
- Compress made of gray or blue clay. The raw materials can be purchased at the pharmacy or assembled yourself. You need to take 200 grams of clay, crumble it and add water so that it covers the raw materials. Leave for 10-15 hours, drain the water and thoroughly knead the clay until a homogeneous consistency is formed. Place the mixture on the fire, bring to a boil and simmer for 1 minute. Then it should be poured onto a cellophane surface and molded into a cake 3 cm thick. Then it should be placed on the lower abdomen and wrapped in a towel. To achieve the effect, at least 10 procedures are required.
- A decoction of boron uterus and cinquefoil. Take 1 tbsp. herbs, pour 2 cups of boiling water over it and boil for 15 minutes. The resulting product must be taken during the day in 3 doses. The cinquefoil decoction is prepared in the same way. You need to take it in turns - one day, one day, the second. The course of treatment is 1 month.
- Treatment with leeches. This is an effective way to eliminate endometriosis, but it can only be done in qualified clinics. The course of treatment lasts on average a week.
With qualified treatment, endometriosis will disappear forever. True, sometimes unpleasant consequences are possible - transition to a chronic form, development of infertility, relapse. Treatment of endometriosis is a very long and labor-intensive process. Following all the doctor’s recommendations will be the key to success.
Patient reviews
Barova Elena:
Not long ago I was diagnosed with retrocervical endometriosis. The doctor said that it was necessary to have an operation. For a long time I couldn’t decide who to turn to, until I found out about Levshin Philip Alexandrovich
.
I had the operation done by him
.
No complications
.
The recovery period passed without problems. I took hormonal pills for about 4 more months
. Nothing worries me now.
Sidorchuk Evgeniya:
Personally, I was treated for retrocervical endometriosis by Levshin Philip Aleksandrovich. Excellent specialist
.
Truly a master of his craft
.
The operation went without problems
.
It’s been a long time since I remember painful periods and other problems associated with the disease. I go to the gynecologist twice a year for a preventive examination so that lesions do not appear again
. They said it was possible.
See what curettage is for endometriosis
https://youtu.be/42xdEPUwpXg
Endometriosis is a pathological process that is always characterized by the appearance of lesions (hyterotopies) in organs related to the reproductive system and others. In structure and functionality, these lesions are similar to the endometrium (uterine mucosa)
.
Retrocervical (retrocervical) endometriosis is one of the types of the described disease
.
It usually occurs in women after thirty years of age, but there are exceptions.
The pathology in question is a process in which endometrioid tissue grows directly near the cervix, as well as on its posterior surface and in the area of retrovaginal tissue.
This form of the disease belongs to deep endometriosis, and the mechanism of its development is directly related to microperforation of endometrioid cysts, the growth of pathological foci from the isthmic region of the cervix.
The main feature of this type of endometriosis is infiltrative growth , that is, the growth of pathological areas towards the rectum, posterior vaginal fornix and vaginal-rectal septum.
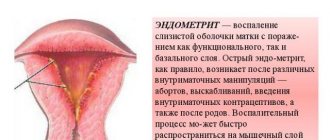
Endometriosis
Endometriosis is an acute problem in general gynecology. The spread of endometriosis in the modern population is catastrophic, which gives this disease a social significance. Every year, endometriosis is diagnosed in thousands of young and beautiful women, the vast majority of whom, even after many years of grueling treatment, will remain infertile and will be doomed to physical suffering associated with pain.
Laparoscopic surgery has ushered in a new era in the treatment of endometriosis. This is a very difficult surgery if you perform full-fledged radical operations, but we have no choice. IVF is a good solution to the problem of infertility caused by endometriosis, but pain, which can psychologically break even very strong people, pain from endometriosis can only be removed through surgery. In any case, IVF results will be better in a surgically treated, prepared patient. Spontaneous pregnancy in 30 percent of operated patients (and this percentage can be much higher in young and timely patients) is also a good chance that we can “hand” to our patients and it is unwise to ignore this possibility.
We know a lot about endometriosis, but not enough. Of all the existing theories of the origin of this disease, not one yet satisfies modern practical medicine. We have well studied the variety of forms and corresponding clinical manifestations, the stages of the pathological process, but what triggers the development of the disease? Where is the weak link that could be influenced in order to prevent the disease? Why do some people get endometriosis and others don’t? And, most importantly, how endometriosis interferes with pregnancy is still not clear.
Endometriosis is a pain. Pain on the eve of or during menstruation, during physical activity, sports, or sexual intercourse. The pain is exhausting, reduces the ability to work, worsens the quality of life, and finally disables the patient.
Endometriosis is infertility. As a factor that persistently prevents pregnancy, endometriosis occupies a leading position, especially among residents of large cities.
Endometriosis is a disease whose diagnosis still causes serious problems for most outpatient doctors. Before a correct diagnosis is made, such patients usually have extensive experience of unsuccessful attempts at conservative treatment of other diseases. Many different remedies have been tried: almost all existing antibacterial drugs, anti-inflammatory drugs, painkillers, immunostimulants, physiotherapy, etc. Patients with infertility caused by endometriosis go through a lot: here are countless hormone studies, attempts to clarify the condition of the fallopian tubes, dozens of ultrasounds, and sometimes MRIs, attempts to identify rare infections, study the immune status, and so on. We are talking only about official medicine, but many also pass through the hands of paramedics - homeopaths, osteopaths, from whom it is not so easy to get out. )))
The problem is not only in making a correct diagnosis in a timely manner, this, as they say, is not so bad. There is still no unity among doctors regarding approaches to the treatment of endometriosis. Among outpatient gynecologists, there is an underestimation of the importance of timely recommendations for laparoscopy. As an example: patients with small endometrioid cysts have been treated with hormonal drugs for years or are simply observed, wasting time. And the disease progresses at this time. The myth at work here is about the extreme trauma of ovarian surgery, the loss of healthy tissue, and the irreversible consequences of such operations.
But there are different surgeons, different techniques. And then..., in any case, you need to part with the endometrioid cyst, it will not go away on its own. And it is better to do this while its diameter is small; as the cyst grows, the intraoperative trauma to the ovary will increase. Agree, it is different things to operate on a cyst 2-3cm, 5-6cm or 8-10cm in diameter.
It is with the exclusion of endometriosis that we begin the conversation with all patients with no pregnancy, and we are not mistaken. The situation now is different from the early 2000s. Then, in the first place, as a factor of infertility, were inflammatory diseases of the uterine appendages caused by sexually transmitted infections, and, as a consequence, adhesive deformation of the fallopian tubes. The examination of the patient with infertility began with clarification of the condition of the fallopian tubes. At least, this is what came to mind first of all for most doctors. Then... but not now. A lot has changed since then. Nowadays, few people are embarrassed to use barrier contraception. Now there are laboratories at every step where you can quickly consult, be examined and receive comprehensive treatment recommendations. Finally, pharmacies are flooded with high-quality imported antibacterial drugs. One way or another, after 15 years, the tubo-peritoneal factor of infertility lost its leadership to endometriosis. And this is not just my personal opinion.
In my opinion, even a cursory collection of anamnestic data from a patient is enough to suspect endometriosis as the most likely cause of infertility. The final answer to the question is often given by a simple examination in a chair (see article on the diagnosis and treatment of endometriosis). Let's try to illustrate this thesis with a specific clinical example.
The photo shows a clinical case of endometriosis
The photographs below show a simple form of infiltrative endometriosis of the uterosacral ligaments. So simple that it is rare. However, this is a very typical situation, a typical history of the disease, a typical fate of an individual woman. Several years of infertility (the patient is 30 years old, she has been married for more than 6 years) and all the ordeals that we described above. Apart from infertility, nothing bothers me except painful menstruation, but “what’s unusual about this?”... A short conversation and it turns out that there is also pain during sexual intercourse, and, recently, during bowel movements during menstruation. An examination and... a diagnosis, that is, a guess as to what the cause of infertility is, has been made. What's the secret? — in a targeted study of the proximal parts of the uterosacral ligaments, as the zone of the most likely spread of focal infiltrative endometriosis. The doctor accurately identifies the lump, and the patient feels acute pain radiating into the rectum. During laparoscopy it looks like this.
Endometrioid infiltrate on the left sacrouterine ligament
Endometriosis of the “arch” of the uterosacral ligaments
In this situation, an hour and a half of careful surgery and the chances of spontaneous pregnancy change dramatically. The purpose of the operation is to excise tissue affected by endometriosis. Superficial coagulation will not have any effect.
Endometriosis is a disease that can only be definitively diagnosed and treated during laparoscopic surgery. It is laparoscopy that makes it possible to move from guesswork and assumptions to clarifying the clinical diagnosis and specific therapeutic manipulations. The future fate of the patient depends on the timeliness and quality of the laparoscopic surgery performed. There are not many specialists capable of adequately operating on complex forms of endometriosis, but they exist, and their number is increasing
Endometriosis - what prevents effective treatment
- There is a lack of trained specialists capable of diagnosing endometriosis in a timely manner and performing a full laparoscopic operation at the proper level, especially in the regions. It takes at least five years to train one such surgeon. And this is with a very successful set of circumstances and a “good school”... and not in our country, unfortunately.
- The second reason is the lack of consensus in the approach to treating this disease. The total spread of the myth about the so-called combined two-stage treatment of endometriosis can be called a real disaster. It is assumed that in addition to the first, surgical stage of treatment of endometriosis, a second, no less important stage is required, which involves the use of hormonal drugs that cause artificial menopause after surgery for several months. The hope that the consequences of a mediocre operation can be eliminated by using expensive hormonal drugs deprives most of my colleagues (sincere and not so sincere) of motivation in mastering and implementing this type of surgery at the proper level. (See Section “Development of endometriosis”).
Classification of the disease
In the clinical classification of retrocervical endometriosis, there are four main stages of disease development:
- stage 1 - lesions do not extend beyond the rectovaginal tissue;
- stage 2 - endometrioid tissue grows into the cervix and vaginal wall, small cysts appear;
- stage 3 - pathological lesions penetrate the serous covering of the rectum and the uterosacral ligaments;
- stage 4 - the rectal mucosa and peritoneum of the rectal-uterine space are already involved in the pathological process, adhesions are formed in the area of the uterine appendages.
Causes of retrocervical endometriosis
Retrocervical endometriosis is the spread of endometriotic tissue along the rectovaginal tissue (the space between the rectum and the posterior wall of the vagina and cervix).
The cause of the disease has not been fully established.
According to the embryonic theory, the rudiments of endometrioid cysts in various tissues and organs are formed in the prenatal period as a result of disruption of tissue differentiation processes. Also, the implantation mechanism of the occurrence of retrocervical endometriotic growths is not denied - the reverse flow of menstrual fluid into the uterus and abdominal cavity.
The following risk factors predispose to the development of retrocervical endometriosis are identified:
- Operations and diagnostic manipulations on the cervix and body of the uterus (diagnostic and therapeutic curettage, various methods for examining the patency of the fallopian tubes, abortions).
- Difficult childbirth, accompanied by cervical ruptures.
- Chronic inflammation (vaginitis, cervicitis, endometritis) of various etiologies.
- Diseases accompanied by disruption of the hormonal function of the ovaries (tumors, inflammation of the appendages, polycystic ovaries, pathologies of the hypothalamus and pituitary gland).
- Autoimmune diseases.
- Family history of endometriosis.
Causes of retrocervical endometriosis
This disease has not yet been fully studied, and the exact causes of endometriosis have also not been established. Medical scientists suggest that the following factors are of great importance in the development of the disease:
- retrograde menstruation , when during menstruation a small amount of blood containing the endometrium enters the abdominal cavity through the fallopian tubes during uterine contractions. There, endometrial particles are implanted into various organs
. In healthy women, this phenomenon also occurs, but their immune system immediately suppresses the proliferation of endometrioid tissue; - Another reason for the development of endometriosis, including retrocervical, may be immune disorders . If immunity is reduced, it cannot prevent the proliferation of endometrial cells that enter the abdominal cavity;
- Hormonal factors can also influence the development of the disease , because the endometrium is very sensitive to female sex hormones. Thus, excess estrogen will contribute to the growth of pathological foci;
- a genetic factor as a possible cause of the disease ;
- significantly increase the risk of retrocervical endometriosis and any surgical interventions in the genital organs , including abortion, cesarean section, etc.
Treatment of retrocervical endometriosis
The main goals of treatment for retrocervical endometrioid cysts are: restoration of reproductive function and improvement of the patient’s quality of life. The most effective is considered a combined approach to treatment, i.e. combined use of medical and surgical methods for eliminating endometriosis.
Conservative therapy
The basis of drug therapy for endometriotic growths is the prescription of hormonal drugs. Their long-term use suppresses the production of their own sex hormones in the ovaries. This stops the growth and spread of endometrioid tissue and suppresses its cyclic changes. After surgical removal of pathological growths, hormones are used as a means of preventing relapses. Drugs prescribed for hormonal treatment include:
- Combined oral contraceptives.
- Synthetic progestins.
- Antigonadotropins.
- Gonadotropin releasing hormone agonists.
For the symptomatic treatment of retrocervical endometriosis, anti-inflammatory drugs (Diclofenac, Nimesulide), hemostatic agents (etamsylate, tranexamic acid) and iron supplements are used to treat anemia.
Prevention of adhesions is carried out by prescribing enzyme preparations. Wobenzym and Longidaza prevent the formation of adhesions in the abdominal cavity, reducing the consequences of retrocervical endometriosis for a woman’s reproductive health.
Surgery
When endometrioid cysts are located retrocervically, conservative and radical operations are performed using laparoscopic access. Organ-preserving interventions involve excision of areas of affected rectovaginal tissue and dissection of peritoneal adhesions. Such operations are performed on patients of reproductive age with a non-advanced form of the disease.
In case of total damage to the pelvic organs, radical operations are performed: hysterectomy or total hysterectomy, rectal resection. They do not preserve a woman’s reproductive function, but eliminate the symptoms of the disease, significantly improving the quality of life.
Clinical picture
Retrocervical endometriosis can have a wide variety of clinical manifestations, which become more intense at various stages of development of the pathological process.
Typically, the disease is characterized by the following symptoms:
- intense, sharp pain radiating to the vagina, perineum, thigh, and also to the rectum;
- there is a sharp increase in pain during sexual intercourse, especially if the woman is in a position with her legs raised up, and the partner’s penis reaches the posterior vaginal fornix, where endometriotic lesions are located;
- pain during bowel movements;
- menstruation becomes more abundant and painful, often accompanied by a feeling of nausea, vomiting, and sudden mood swings;
- Many women experience constipation, especially during menstruation, which often leads to intestinal obstruction;
- in some cases, constipation may be replaced by diarrhea;
- As the pathology develops, women experience a false urge to defecate, secretion of mucus from the anus, and during menstruation, blood;
- Some patients report an increased urge to urinate and a feeling of heaviness in the bladder.
At its initial stage, retrocervical endometriosis may be asymptomatic , but pathological manifestations become more pronounced as the disease progresses. Often women feel such severe pain that they can only stay in bed, as any movement becomes extremely painful.
How do the symptoms of retrocervical endometriosis differ from diseases of other localizations?
Common symptoms of endometriosis:
- pain in the lower abdomen, intensifying during menstruation and, in some cases, during sexual intercourse;
- intermenstrual bleeding;
- violation of monthly cycles;
- heavy menstrual bleeding;
- nausea and vomiting;
- severe premenstrual syndrome.
With retrocervical endometriosis, additional symptoms appear:
- pain in the pelvic area no longer radiates down the abdomen, but into the perineum and rectum;
- sometimes the pain covers the outer thigh and perineum;
- urination becomes more frequent;
- bowel movements become painful;
- constipation appears;
- ribbon-like stool comes out along with bloody mucus;
- stool disorders are often observed - diarrhea alternates with constipation;
- gas formation increases.
Diagnosis of endometrioid tissue
- The diagnosis of retrocervical endometriosis is established on the basis of available clinical data, as well as the results of additional diagnostic studies. First of all, colorectal and ovarian cancer should be excluded.
- A vaginal examination is also performed , during which dense nodes with a tuberous structure are palpated. During a mirror examination, the doctor can observe small endometrioid cysts; they look like bluish eyes.
- A fairly informative study of retrocervical endometriosis will be ultrasound , which reveals a heterogeneous compaction under the uterine cervix, smoothness of the isthmus, as well as unclear contours of the rectum.
- , biopsy becomes the leading additional diagnostic method . If there is damage to the rectum, then there is a need for sigmoidoscopy and targeted biopsy.