Retinal detachment is a serious disease, or more precisely, a condition characterized by the separation of the retina of the eye from the vascular layer. This phenomenon leads to a significant decrease in vision up to the onset of complete blindness. According to statistics, 72 percent of all cases of absolute vision loss are caused by retinal detachment.
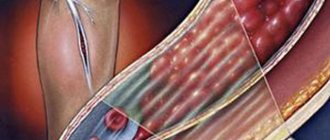
The retina of the eye provides a person with vision. It displays everything we see, after which the information is delivered to the brain along the optic nerve. In a normal healthy eye, the retina is tightly adjacent to the choroid, which provides it with nutrition and moisture. If it is damaged for one reason or another, a person can become completely blind in a short time if he does not seek professional help in time.
When the retina is detached in one or more places, vitreous fluid enters the tear areas, aggravating and accelerating the process. Accordingly, some parts of the retina are deprived of blood supply, atrophy and die. It is total retinal detachment that causes blindness.
What is the retina and why is it important?
Let's imagine the eye in a sagittal, that is, sagittal, section. The surface of the eye is covered by a transparent membrane called the conjunctiva. Above the pupil, the conjunctiva becomes the cornea. Under the conjunctiva is the sclera - it is white, and under the cornea is the iris, in the center of which is the pupil. Behind the pupil is the lens, and behind it is the vitreous body.
It fills most of the intraocular space, and between it and the sclera is the retina, or retina. Its function is the perception of light rays collected and refracted by the cornea and lens. In other words, this one is responsible for the coordinated work of the visual analyzer, converting the received light impulses into electrical ones, which are subsequently transmitted to the cortical analyzer along the optic nerve.
The retina consists of an unevenly distributed number of two types of nerve cells - rods and cones. The former are responsible for light perception, the ability to distinguish the outlines of objects in the dark, as well as navigate in space. They are located relatively evenly over the entire surface of the retina, but still their number is greater at the periphery. Cones are responsible for the difference between colors, their shades and visual acuity in general. This type of nerve cell is focused in the central part of the retina, since this is the area where refracted light rays are projected.
Between the sclera and the retina there is a thin choroid, which provides nutrition to the peripheral part of the visual analyzer. Detachment of the retina from the choroid of the eye entails a violation of its trophism, which means necrotization and loss of the ability to transform and transmit further light impulses. In other words, a person simply loses his vision.
Types of pathology
Depending on the stage of the disease, there are:
- Primary retinal detachment, in which fluid from the liquefied vitreous body penetrates into the gap;
- Secondary, in which a neoplasm occurs between the retina and the choroid (tumors, diabetic retinopathy, hemorrhages or inflammatory infiltrate).
According to the level of mobility, pathology is:
- Mobile;
- Rigid.
Diagnosis of retinal detachment requires the patient to remain in bed for two days, after which the position of the retina is checked. If it is completely adjacent, then it is considered to be mobile, but if not, then it is rigid.
The form of internal manifestation of the disease also determines the typology:
- High retinal detachment - accumulation of fluid in the form of a bubble;
- Flat – folded relief.
Depending on the extent of distribution of retinal detachment, there are:
- Local – within one quadrant;
- Common – localization in two quadrants;
- Subtotal – localization in 3 quadrants;
- Total retinal detachment is a complete detachment from the vascular wall.
Causes of retinal detachment
The reasons that determine the development of such a serious pathological process are usually divided into groups, and therefore several etiological types of retinal detachment are distinguished.
- Traction, the vast majority of cases of which are associated with pathology of the vitreous body. Closely adjacent to the retina, the vitreous body can create tension in some of its areas during the formation of connective tissue cords or the sprouting of blood vessels. Similar changes in the vitreous body occur in particular with diabetic retinopathy, and therefore diabetics should regularly visit an ophthalmologist for preventive purposes.
- With rhegmatogenous retinal detachment, it ruptures in a place where its normal structure is transformed or thinned. Transformation of areas often occurs due to dystrophic changes, which may not be diagnosed before the rupture appears. A person simply begins to feel the symptoms accompanying this pathology, without the slightest suspicion about their nature. For this reason, rhegmatogenous detachment is also called primary or idiopathic, that is, one whose cause cannot be accurately determined. The fluid produced by the vitreous body falls under the area of detachment, and due to disruption of trophic processes, the retina in this place dies, and along with it the patient’s vision “dies”. A rupture in dystrophically altered areas can occur with excessive physical activity, an attempt to lift something heavy, when making sudden movements, or even at rest.
- Secondary retinal detachment that occurs due to existing diseases of the functional structures of the eye. These include infectious and inflammatory diseases of the eye, neoplasms, thrombosis, retinopathy and hemorrhage.
- Traumatic retinal detachment. This type of pathology is provoked by trauma, and subsequent detachment can occur both at the time of injury and within hours/months/years after the action of the traumatic factor. This category also includes detachments that occur as a result of surgery.
- Serous (exudative) retinal detachment, which occurs during the accumulation of fluid behind the retina. The retina itself does not undergo ruptures or dystrophic changes.
It is impossible to say reliably about the connection between retinal detachment and the following factors, however, it has been noted that they often accompany the resulting pathology. These include:
- Elderly age. People over sixty years of age have an increased risk of developing the condition compared to younger people.
- High grade mopia. Up to half of the cases of retinal detachment in the world are accompanied by high degrees of myopia.
- Previous eye surgeries. Statistics show forty percent of cases of pathology occurring in response to eye surgery.
- The presence of hypertension, and especially hypertensive crises.
These risk factors should alert their owners to the occurrence of such a serious pathology and encourage patients to carefully monitor their own health so as not to miss the initial signs of retinal detachment.
Treatment
For retinal dissection, treatment is performed surgically. The purpose of the operation is to restore lost contact between the layers of the retina and block the resulting gaps.
Extrascleral methods
Operations are performed on the surface of the sclera, without penetrating the eyeball. Filling is usually performed on young patients with phakic eyes (who have not had their lens removed before). This method is chosen for simple detachments and ruptures of the retina closer to the anterior pole of the eye.
Types of episcleral filling:
- circular;
- sectoral;
- radial.
Scleral buckling is not recommended in the presence of proliferative vitreoretinopathy, large tears and rhegmatogenous detachments. In all these cases, doctors prefer vitrectomy.
Endovitreal methods
Treatment by vitrectomy involves removing the vitreous humor that fills the cavity of the eyeball. After this, the person is briefly injected with special substances that press down the retina and return it to its place. As a vitreous substitute, the patient is injected with liquid silicone, air or other substances intended for this purpose.
Laser methods
Treatment of retinal dissection with a laser is carried out only in the case of fresh defects of small size. Peripheral laser coagulation allows you to solder the mesh and prevent its further detachment. The method is contraindicated when the lesion is localized in the macula. Read more about laser coagulation of the retina →
Signs of retinal detachment
Retinal detachment requires everyone to know its symptoms, not just those who are most at risk for it. So, let's remember them.
- Black dots appear before your eyes, which prevent you from concentrating on the object in question and do not disappear after rest or sleep.
- At the very beginning of detachment, the patient may notice the appearance of flashes in the eyes, which appear in the form of glare, lightning, spots of light.
- Also at this stage, patients note the curvature of straight lines, the oscillation of the objects in question, their trembling and blurriness.
- A progressive decrease in visual acuity appears, the time frame of which is very narrow: with a massive detachment, a person can lose vision in just a few hours.
- A black spot, veil or line appears. This blackness is the area of detachment that no longer receives and transmits light impulses further for processing to the central organ of the nervous system - the brain. The localization of the blind area in the visual field is determined by the localization of the area of retinal detachment. This symptom progresses to complete loss of vision as the patient delays.
Important! When a dark veil appears at a doctor’s appointment, it is necessary to clarify from which side its spread began.
- Retinal detachment, the symptom of which is a narrowing of the field of vision, is called marginal or peripheral. In such a situation, vision begins to disappear “from the edges”. After sleep and in the morning, this symptom decreases somewhat, which the patient mistakes for an improvement in the clinical condition.
- A symptom of retinal detachment in some cases is the loss of letters, words or sections of text from the field of view when reading. This indicates that the central part of the retina has been captured by the pathological process.
The insidiousness of this pathology is that, despite its seriousness, it does not cause pain. With this course of the disease, a person may not rush to see a doctor, “because it doesn’t hurt,” attributing the occurrence of retinal detachment and its symptoms to overwork, nervous shock and other life circumstances. Instead of immediately going to the ophthalmologist, such patients spend precious hours sleeping and resting, believing that everything will go away on its own in the morning.
And if in the morning, after a long stay in a horizontal position, the retina “falls” into place, fitting more tightly to the choroid and the symptoms of the disease decrease, a person may completely refuse to visit the doctor, citing positive dynamics.
| However, you should remember: if the first (or at least similar to the listed) symptoms occur, you should contact an ophthalmologist immediately, because there are no conservative methods for treating retinal detachment. |
The only effective treatment method is surgery, and the sooner it is performed, the greater the patient’s chances of returning full vision.
How does retinal detachment manifest?
The onset of detachment can be determined by characteristic symptoms. Patients most often complain of metamorphopsia (curvature of straight lines) and photopsia (light flashes). When a retinal vessel ruptures, a large number of floaters and black dots appear in the field of vision.
During direct retinal detachment, there is a presence of a veil before the eyes, a veil or a dark shadow. Vision rapidly deteriorates, although in the morning it may improve slightly and the field of vision expand. The black curtain obscures part of the field of vision, spreads to the entire retina, and the person goes blind.
Diagnosis of retinal pigment epithelium detachment
Despite the fact that in ophthalmological practice, retinal detachment with its symptoms is an emergency condition, before starting treatment for this condition, it is necessary to conduct a comprehensive medical examination of the patient.
- An examination using an ophthalmoscope will allow you to assess the location, shape and size of the pathological process. The presence of retinal tears is confirmed or denied.
- Conduct research using contact and non-contact lenses.
- In case of chronic retinal detachment, electrophysiological research methods are used to assess the functional capabilities of the eye and at the same time make a prognosis regarding the restoration of vision in the patient.
- If there are concomitant eye diseases that make examinations with lenses or an ophthalmoscope difficult, ultrasound examination is used.
- Perimetry and assessment of visual acuity are carried out, which makes a proper contribution to determining the magnitude and localization of the pathological process.
- Additionally, intraocular pressure is measured, which may be reduced in comparison with a healthy eye.
Benefits of treating retinal detachment at the Excimer Clinic
- All operations and procedures aimed at treating retinal detachment at the Excimer ophthalmology clinic are carried out in a convenient “one-day” mode for patients, without hospitalization .
- An obligatory component of quality treatment is the use of the wide capabilities of the latest generation microsurgical equipment. It is this equipment that allows our specialists to act effectively and achieve results even in situations of complex retinal problems.
- The qualifications and vast practical experience of our doctors allow us to perform microsurgical interventions at the highest professional level. We regularly exchange current experience in the treatment of retinal diseases with Russian and foreign colleagues and offer patients of our clinic all the best and most effective of what modern ophthalmology is proud of.
Retinal detachment: symptoms in an ophthalmoscope
Normally, examination of the fundus with an ophthalmoscope using plus lenses gives a red reflex. This is the name given to the reflection of light from the inner surface of the eye, and it is indeed red. This color is due to the translucency of blood vessels through the retina, which, as mentioned above, serves as a source of powerful blood supply and nutrition to the retina.
When it is detached, the red reflex from the fundus disappears, leaving behind a gray or whitish color. This is the picture with massive or complete detachment. Detachment of a small height is evidenced only by a change in the clarity of the visible vessels, their course or size. However, an experienced ophthalmologist will notice such minor changes.
A high-height retinal pigment layer detachment is defined as a tall bubble filled with a grayish or white cloudy liquid that can fluctuate when the eyes move. Old detachments leave behind rough areas of the retina that are subject to wrinkling, folding and scarring.
Using an ophthalmoscope, the doctor can determine the presence of a rupture. The rupture looks even redder against the general background of the fundus due to better visibility of the choroid. If the pathological process was diagnosed at a stage when further treatment will give positive results, the doctor can make a prognosis regarding the prospects for treatment and progression of the disease based on one ophthalmoscopy.
Diagnostics
How to determine retinal detachment? Pathology can be suspected by the presence of characteristic symptoms, namely the appearance of lightning, flashes of light and blurred vision. To confirm the diagnosis, the following studies are performed:
- Determination of visual acuity with and without correction, measurement of visual fields and intraocular pressure. Such an examination allows you to obtain general information about the condition of the visual analyzer and identify indirect signs of retinal detachment. With the disease, intracranial pressure decreases slightly, visual acuity decreases, and scotomas appear—black or colored defects in the field of vision.
- Fundus examination . It is performed using an ophthalmoscope or a slit lamp with a high-diopter lens. Before the examination, the patient is instilled with drops that dilate the pupil (Tropicamide, Cyclomed). Since retinal detachment is clearly visible to the doctor during ophthalmoscopy, he can immediately confirm or refute the diagnosis.
- Optical coherence tomography (OCT) . This method allows not only to see the retina, but also to obtain a layer-by-layer image of it. When a detachment occurs, the tomogram shows a separation of the retina and its protrusion into the vitreous body.
It is very important to find out in a timely manner why retinal detachment occurs. Identifying and eliminating the cause of the pathology significantly increases the chances of recovery and helps to avoid recurrence of the disease. For this purpose, the patient may be prescribed consultations with related specialists and tests.
Retinal detachment: is it possible to return vision?
There is no clear answer to this question. In order to find out the prognosis of treatment results in each specific case, you must personally visit the doctor. Remember: the sooner you see a doctor about treatment, the more results it will give.
There is only one method of treating retinal detachment, and it is surgical. But there are already two types of it, and they are divided into extrascleral, that is, those that are produced through the sclera, and endovitreal, where the vitreous body acts as the point of access to the diseased area.
The principle of both types of surgery is to block the gap, as well as bring the retina closer to the choroid. Both serve to restore adequate trophism of the retina, which is the key to the return and preservation of vision.
Of course, such a threatening problem should be addressed to medical institutions that have a sufficient level of qualifications and an impeccable reputation. Undoubtedly, every person wants to receive the most friendly attitude, close attention and an acceptable price for services.
In Moscow, the multidisciplinary medical center named after Svyatoslav Fedorov fully meets these requirements. Constantly improving the qualifications of doctors, European standards of treatment and attentive nursing staff - this is what awaits you when you contact our medical center.
Remember, retinal detachment does not tolerate either diagnostic or therapeutic failures. Save your vision with us!
Surgical methods for treating retinal detachment
Retinal detachment requires immediate treatment. A long-term pathological process will provoke persistent hypotension, cataracts, iridocyclitis, eye subatrophy and blindness. The main goal of therapy is to bring the layers of the retina together and block breaks. When treating detachment, it is important to bring the photoreceptor layer closer to the pigment epithelium and limit the rupture to foci of chorioretinal inflammation. This is a local sterile inflammation that glues the retina to the choroid and stops the progression of the disease.
At-risk groups:
- a high degree of myopia and astigmatism, which provoke thinning and rupture of the retina;
- age from 45 years;
- heavy loads and high risk of injury in athletes;
- diabetes mellitus, causing diabetic retinopathy and hemorrhages;
- heredity.
Surgical intervention for detachment can be extrascleral (on the surface of the sclera) and endovitreal (from inside the eye). The best treatment option is vitrectomy. This is a procedure to remove the vitreous and replace it with silicone or gas to ensure that the detachment adheres tightly to adjacent layers.
Possible surgeries for detachment
- Extrascleral filling. The operation is performed in the presence of ruptures that do not require exposure from inside the eye. The seal is installed externally.
- Vitreoretinal surgery. It is used for old detachments, when careful cleansing and straightening of the retina is required. Special silicone is injected through pinhole punctures using long instruments.
- Cryocoagulation of ruptures, as well as subclinical detachments.
The goal of treatment is to block the retinal tear. The sooner the operation is performed, the more reliable the result will be and the better vision will be restored. Doctors give the most favorable prognosis for detachments that do not affect the central zone. If the pathology has managed to close the center of the retina, even after a successful operation it is not possible to completely restore vision.
Since retinal detachment is a consequence of a tear, it is necessary to undergo regular preventive examinations and detect them on time. Laser coagulation techniques are used to treat ruptures.
Detachments that were treated incorrectly or unsuccessfully must be operated on within a year, while the eye still perceives light. Surgical treatment of retinal detachments is carried out painlessly, safely and quickly. The operation is carried out using the latest equipment and only highly qualified specialists. Outpatient procedures take from 40 minutes to 1.5 hours, taking into account the complexity of the operation and complications.
Retinal detachment can be corrected through surgery, but not in every case it is possible to restore the integrity of the retina and full vision. Even after successful treatment of severe detachment, vision rarely returns completely. Only in some cases is it restored to its original level.
After surgical treatment there are no restrictions on visual stress, but for a month the patient is prohibited from visiting the bathhouse, sauna and swimming pool. Physical activity should be minimized for a period of one month to a year, depending on the severity of the condition.
After surgery to eliminate detachment, refractive errors (myopia, astigmatism) often increase. Sometimes relapses occur and repeated surgery is required, which often turns out to be ineffective. The success of surgery for detachment is determined by the timeliness of treatment. A long-term pathological process, as a rule, ends with irreversible changes in the retina and the death of visual neurons.
Endovitreal treatment of retinal detachment
Endovitreal surgery involves intervention from the cavity of the eyeball. The doctor makes three incisions in the sclera (approximately 1 mm each), through which he gains access to the vitreous body and retina. This procedure is called sclerotomy. Instruments, a light source, and a solution are introduced through the incisions to maintain the tone of the eye. The most commonly used is a vitreotome - a 1 mm cylinder in which a knife is hidden that cuts the intraocular tissues. If necessary, the doctor may use other instruments.
Expanding gases, silicone oil or perfluoroorganic compounds are used to straighten and press the retina to the membranes. After the introduction of a special substance, laser coagulation of the retina can be performed.
Indications for vitrectomy for detachment:
- big sizes;
- long retinal detachments along the dentate line;
- proliferative vitreoretinopathy, presence of folds;
- posterior retinal tear;
- combination of rupture with hemophthalmos.
During endovetral intervention, the vitreous body is removed (transciliary vitrectomy). Sometimes prolonged tamponade of the cavity with silicone oil or gas is required. The gas bubble will resolve within 2-4 weeks, shrinking and being replaced by intraocular fluid. Silicone oil takes a little longer to remove (2-3 months).
For rhegmatogenous detachment, the doctor removes the vitreous body and the posterior hyaloid membrane. To relieve traction, cords and membranes are removed. During surgery, a bubble of “heavy water” is created in the fundus of the eye, which presses on the retina. Excess fluid is removed through the gap, and laser coagulation of the affected areas is performed. After this, the “heavy water” is replaced with saline solution, and the incisions are sutured. When proliferative vitreoretinopathy of the tissue occurs with an old detachment and it is impossible to smooth it out, loosening peripheral incisions (retinotomy) are required.
Extrascleral treatment of retinal detachment
With endovitreal access, the operation is performed from inside the eye, and with extrasleral intervention, the rapprochement of the retina and pigment epithelium is achieved by indenting the sclera (filling). During the operation, the doctor creates an indentation shaft that blocks the rupture, and the accumulated fluid is gradually absorbed into the epithelium and choroid.
Before such an operation, bed rest is required so that the detachment bubbles decrease as the subretinal fluid is absorbed. This makes it easier to detect the break. After the operation, bed rest is also prescribed, at least for a day.
Scleral filling
When filling the sclera, the layers of the retina are brought together by pressing the sclera from the outside. In the projection of the rupture, a silicone strip or filling of the required size is attached to the sclera. The strip is literally sewn on. Under its pressure, the sclera is pressed inward, pressing the choroid to the retina. In this position, the accumulated fluid begins to dissolve.
Filling stages:
- Determining the location of the rupture, marking this zone on the sclera. For these purposes, a diathermocautery is used, with the tip of which the doctor applies pressure, creates a shaft and marks the location of the projection of the rupture on the sclera.
- Cutting out the filling and suturing it to the sclera in the projection area. The position of the filling will depend on the type of pathology, location and number of breaks. There are radial, sectoral and circular fillings.
- If there is a large amount of fluid, it must be removed through an opening to the sclera (drainage).
- Additionally, air or gas can be introduced into the vitreous body. While the bubble dissolves (several days), vision will remain poor.
- Applying sutures to the conjunctiva.
If there is a large accumulation of subretinal fluid, it is drained through a puncture in the sclera. When filling, soft silicone sponges are used. It is easy to cut out a filling from silicone according to the required parameters.
The type of filling is determined by the doctor, taking into account the type and location of the rupture. There are radial, sectoral and circular fillings. In some cases, they resort to cerclage (circular indentation with silicone thread or braid). The circlage is created in the equator area of the eye.
Possible complications after filling:
- Early: infection of the eyeball and orbit, vascular detachment, glaucoma, dysfunction of the extraocular muscles, ptosis, strabismus.
- Late: exposure of the filling, changes in the central area, refractive errors, cataracts.
- Consequences: lack of detachment adhesion, relapse.
Restoration of vision after filling occurs gradually. This process usually takes several months.
Ballooning of the sclera
The operation involves temporarily placing a catheter with a balloon to the sclera (in the area of projection of the rupture). Liquid is pumped into the balloon, its volume increases, creating the effect of indentation of the sclera, similar to a filling operation.
Ballooning creates conditions for the resorption of subretinal fluid and successful delineation laser coagulation of the retina. The balloon is removed after the formation of adhesions between the retina and adjacent tissues. Ballooning is low-traumatic and is used for various pathologies of the visual system.
Laser coagulation for detachment
After extrascleral operations, diathermal, laser or photographic coagulation is possible. The effect can be consolidated by cryopexy along the boundaries of the detachment from the side of the cavity through the pupil (transpupillary) or the sclera (transscleral). Additional exposure provokes the formation of adhesions around the break and reliable fixation of the retina.
Laser treatment for detachment allows you to create adhesions between the retina and the lining of the blood vessels. The doctor uses laser coagulators to create microburns. This operation is effective for preventing detachment, limiting existing lesions (flat detachments) and additional coagulation after surgery.
Laser coagulation of the retina is performed under local anesthesia. A Goldmann lens is placed on the eye, which focuses laser radiation on a specific area of the fundus of the eye. Adhesions form within two weeks.
Possible complications of laser coagulation:
- exudative detachment;
- vascular detachment;
- degenerative changes in the central region.
Cost of retinal detachment surgery:
| № | Service name | Price in rubles | Make an appointment |
| 2011074 | Introduction of drugs of the 3rd degree of complexity into the vitreous cavity | 65 000 | Sign up |
| 2011073 | Introduction of drugs of the 2nd degree of complexity into the vitreous cavity | 22 500 | Sign up |
| 2011072 | Introduction of drugs of the 1st degree of complexity into the vitreous cavity | 18 500 | Sign up |
| 2011071 | Peripheral vitrectomy 3rd category of complexity | 12 000 | Sign up |
| 2011070 | Peripheral vitrectomy 2nd category of complexity | 10 000 | Sign up |
| 2011069 | Peripheral vitrectomy of 1st category of complexity | 8 000 | Sign up |
| 2011068 | Microinvasive revision of the anterior chamber | 12 000 | Sign up |
| 2011075 | Intraoperative administration | 6 000 | Sign up |
| 2011066 | Reconstruction of the anterior chamber | 6 000 | Sign up |
| 2011065 | Removal of perfluoroorganic liquids from the vitreous cavity | 7 500 | Sign up |
| 2011064 | Removing liquid silicone from the vitreous cavity | 10 000 | Sign up |
| 2011063 | Circular retinotomy or retinectomy | 14 000 | Sign up |
| 2011062 | Retinotomy and retinectomy | 7 500 | Sign up |
| 2011061 | Injection of gas into the vitreous cavity | 10 000 | Sign up |
| 2011060 | Injection of liquid silicone into the vitreous cavity | 15 000 | Sign up |
| 2011059 | Introduction of perfluoroorganic liquids into the vitreous cavity | 12 500 | Sign up |
| 2011058 | Circular peripheral endolaser coagulation of the retina | 13 750 | Sign up |
| 2011057 | Endolaser coagulation of the retina, delimiting (one quadrant) | 6 000 | Sign up |
| 2011056 | Endodiathermocoagulation | 7 500 | Sign up |
| 2011055 | Removal of epiretinal membranes or posterior hyaloid membrane of the third category of complexity | 48 000 | Sign up |
| 2011054 | Removal of epiretinal membranes or posterior hyaloid membrane of the second category of complexity | 39 750 | Sign up |
| 2011053 | Removal of epiretinal membranes or posterior hyaloid membrane of the first category of complexity | 30 500 | Sign up |
| 2011067 | Endodrainage of subretinal fluid | 6 000 | Sign up |
| 2011052 | Unscheduled revision of the vitreal cavity | 35 000 | Sign up |
| 2011051 | Revision of the vitreous cavity of the third category of complexity | 27 500 | Sign up |
| 2011050 | Revision of the vitreous cavity of the second category of complexity | 23 500 | Sign up |
| 2011049 | Revision of the vitreous cavity of the first category of complexity | 17 000 | Sign up |
| 2011048 | Vitreoretinal surgery for complicated conditions (2-stage) of the highest category | 175 050 | Sign up |
| 2011047 | Vitreoretinal surgery for complicated conditions (2-stage) of the third category | 135 050 | Sign up |
| 2011046 | Vitreoretinal surgery for complicated conditions (2-stage) of the second category of complexity | 99 950 | Sign up |
| 2011045 | Vitreoretinal surgery for complicated conditions (2-stage) of the first category of complexity | 70 350 | Sign up |
| 2011042 | Vitrectomy for complicated conditions of the second category | 75 000 | Sign up |
| 2011041 | Vitrectomy for complicated conditions of the first category of complexity | 69 500 | Sign up |
| 2011039 | Vitrectomy for uncomplicated hemophthalmos or vitreous opacities of the second category | 53 750 | Sign up |
| 2011038 | Vitrectomy for uncomplicated hemophthalmia or vitreous opacities of the first category | 45 000 | Sign up |
| 2011037 | Removal of a silicone filling implanted in another medical institution | 20 750 | Sign up |
| 2011036 | Removal of a silicone filling within a period of more than 6 months. after the first operation | 15 550 | Sign up |
| 2011035 | Pneumoretinopexy for retinal detachment | 18 500 | Sign up |
| 2011034 | Additional extrascleral filling in case of detachment | 24 050 | Sign up |
| 2011033 | Combined extrascleral filling for detachment | 54 000 | Sign up |
| 2011032 | Circular extrascleral filling for detachment | 40 350 | Sign up |
| 2011031 | Local extrascleral filling for retinal detachment | 31 500 | Sign up |
| 2011030 | Extrascleral ballooning for retinal detachment | 26 500 | Sign up |
| 2011028 | Set of disposable consumables for vitreoretinal surgery | 48 000 | Sign up |
| 2011027 | Introduction of drugs into the vitreous cavity (Eylea, Lucentis, Ozurdex) | 46 000 | Sign up |
| 2011040 | Vitrectomy for uncomplicated hemophthalmia or vitreous opacities of the third category | 65500 | Sign up |
| 2011043 | Vitrectomy for complicated conditions of the highest category of complexity | 105 900 | Sign up |
| 2011044 | Vitrectomy for complicated conditions of the third category of complexity | 120 750 | Sign up |
Making an appointment Today: 16 registered
Retinal detachment during pregnancy and childbirth
The risk of retinal detachment is especially high in pregnant women with high degrees of myopia. For women who have a detached retina, as well as those who are at high risk of developing the pathology, doctors often recommend delivery by cesarean section. The operation eliminates the period of pushing, which avoids undesirable consequences.
All pregnant women should have regular eye exams with an ophthalmologist. Timely examinations allow us to notice defects in the fundus in time and take appropriate precautions.
The most effective and safe method of treating and preventing the disease is laser coagulation. If the condition of the fundus improves after the procedure, the woman is allowed to give birth naturally.
Symptoms
Clinical signs of retinal detachment are quite characteristic.
The precursors of detachment are the so-called light phenomena: “flashes”, “sparks”, “zigzags of lightning”. These manifestations of photopsia indicate irritation of the photosensitive cells of the retina, which is caused by traction from the vitreous body. They are especially noticeable when your eyes are closed. Often floaters appear in the field of vision. The patient may observe many pronounced “black dots” and “soot flakes”, as well as floating “lace” or a black “veil” in front of the eye. Their appearance is associated with damage to the retinal vessels when it ruptures, followed by hemorrhage into the vitreous body.
All these symptoms indicate the onset of retinal detachment. In rare cases, retinal detachment occurs completely asymptomatically, and it is very difficult to detect it at the initial stage.
Features of the occurrence of lesions during pregnancy
During pregnancy, the risk of tissue degeneration increases many times over. This is due to hormonal changes in the body, as well as the stress that a woman often experiences during this period. Additional factors can increase the likelihood of a problem occurring:
- Toxicosis;
- Myopia (especially progressive or moderately progressive);
- High blood pressure.
If myopia is present, a pregnant woman should undergo a routine examination for destructive changes within two weeks after the start of pregnancy. At this stage, the ophthalmologist must record visual acuity and perform an ophthalmoscopy. A follow-up appointment may be scheduled for the third trimester.
If the medical examination reveals an increased risk of retinal detachment, the doctor will consider terminating the pregnancy. Cesarean section during childbirth also helps reduce the likelihood of complications.
Causes
schematic drawing of the structure of the eye
Note that the reasons in this case can be various factors; we list the most common ones:
- retinal tear;
- illiterate surgical intervention;
- head and eye injuries;
- tumor-like formations of the organs of vision;
- contact with the retina of the contents of the vitreous body;
- diseases of the organs of vision - uevitis, retinitis, chorioretinitis;
- dystrophic pathologies of the retina;
- diabetes;
- severe and prolonged toxicosis during pregnancy;
- hypertension.
Convergent strabismus in children can occur at an early age.
The primary form of detachment is always caused by a direct rupture of the retina. In addition, the retina sometimes becomes thinner due to age or disease, which also leads to its perforation.
The problem can arise due to mechanical injuries, damage to the head, eyes. Detachment can be complete or partial: it is clear that the first option is much more dangerous and more difficult to tolerate, and is more difficult to treat.
Doctors today also know provoking factors that could theoretically lead to retinal detachment. This:
- myopia;
- alcoholism;
- cataract and astigmatism;
- fundus pathologies;
- regular eye strain;
- history of diabetes mellitus;
- intoxication;
- viral eye diseases;
- pathological pregnancy;
- complicated genetic factor;
- poor personal hygiene.
diagram of retinal detachment and rupture
Retinal detachment can take different forms:
- be rhegmatogenous or primary;
- have a traumatic origin (can only be treated with urgent surgery);
- be exudative or secondary (a symptom of the underlying disease).
Most often, this pathology affects one eye, and only 15% of patients have a risk of developing bilateral detachment.
Causes of pathology
The main factor contributing to the development of this disease is damage to the retina. As a result of the rupture, vitreous fluid enters under the surface of the retina, which leads to separation of the choroid and retina.
Retinal disinsertion
Causes of ruptures:
- the development of an inflammatory process affecting the vascular or iris. Inflammation may be chronic or protracted;
- high degrees of myopia (myopia), which, in turn, can lead to atrophy of some areas of the patient’s eye;
- mechanical damage to the organs of vision as a result of injury;
- intense physical activity (weight lifting, strong falls, jumping, etc.);
- development of other ophthalmological pathologies, including hemorrhage, diabetic retinal disease, infection).
There are many causes of retinal detachment
Retinal detachment is a dangerous pathological abnormality that often leads to poor vision. Incorrect treatment can lead to serious complications, so it is important to identify the disease in time.
Signs of the disease
Symptoms appear early and are easily recognized. The main precursors of the disease are:
- Decreased vision.
- Loss of vision.
- The appearance of spots in the field of vision (photopsia).
- Deterioration of lateral vision.
- Curvature of even objects (metamorphopsia).
Important! Retinal detachment is not accompanied by pain.
At the first stage, glare or flashes appear in front of the eyes, and the clarity of vision is impaired. Symptoms occur in bright light. At the next stage, dots appear before your eyes. They are felt constantly, regardless of the light level. At the third stage, patients are bothered by clouding of the picture. If a detachment occurs, a shadow appears and a sharp decrease in vision.
Surgical treatment
The essence of any surgical intervention is to attach the detached retina to the pigment layer containing blood vessels in order to restore the blood supply to the retina. It is performed by pressing the sclera at the site of detachment.
By access path there are:
- Extrascleral interventions
Filling the sclera with silicone sponges of various shapes depending on the type of detachment. The operation is performed on the surface of the sclera by creating an area of scleral depression. Ballooning of the sclera is a temporary suturing of a special catheter with a balloon to the sclera in the area of projection of the retinal tear.
By increasing the size (inflating) of this balloon, an indentation shaft is formed and the same effect occurs as when filling the sclera. After the maturation of the adhesions of the retina to the underlying tissues, the balloon is removed.
- Endovitreal interventions
The operation is performed from the inside of the eyeball; the main type of such intervention is vitrectomy - removal of the vitreous body. Indications for such intervention: giant retinal tears, hemorrhage into the internal media of the eye.
After removal of the vitreous, tamponade of the eye is performed with silicone oil balanced with saline. solution, gas-air mixtures to create fusion of the retina with the underlying tissues.
Postoperative period, recommendations for patients
After treatment for retinal detachment, patients need care. A bandage is applied. This helps prevent the penetration of microbes and secondary infection.
The bandage needs to be changed regularly. It must be sterile. The eyelids are treated with an antiseptic solution. Soon the bandage can be replaced with sterile gauze.
It is fixed with adhesive tape on the forehead. There may be temporary pain after surgery. To eliminate it, NSAIDs or analgesics are used. Drugs such as Ketanov and Ketorol are often prescribed. After the operation is performed, you must remain in bed. All patients should avoid lifting heavy objects.
It is allowed to lift objects weighing no more than 5 kg. It is necessary to prevent stressful situations and mental overload. After eye surgery is performed, it is necessary to temporarily prevent water, soap and gels from coming into contact with the damaged area.
The doctor prescribes a drug from the group of glucocorticoids or antibiotics. The most commonly used drugs are Indocollir, Tobrex, Floxal, Tobradex.
If a person has a history of diabetes, then corticosteroid-based drops are used. These include Diprospan and Kenalog. After discharge, you must visit an ophthalmologist to assess the condition of the visual analyzer.
In the first weeks after surgery, a person will need to wear glasses or contact lenses. Most often, vision returns to normal within a few months. In weakened people, this period increases.
To avoid accidents, it is not recommended to drive a car after surgery. It is necessary to limit fluid intake. It is recommended to follow a salt-free diet and completely abstain from alcoholic beverages.
Daily washing should be done with the head tilted back, this will prevent water from getting into the operated eye. If water gets in, the eye is washed with an aqueous 0.02% solution of furatsilin or a 0.25% aqueous solution of chloramphenicol.
A blindfold is required to protect against dust and bright light. Drug therapy in the postoperative period consists of antibiotics to prevent infectious complications and anti-inflammatory drugs to reduce swelling and intraocular pressure.
Visual acuity will finally be established two to three months after surgery, but in the early postoperative period temporary glasses or lenses are needed to avoid eye strain.
Preventive measures
As for the prognosis for this disease, it depends on many factors:
- patient's age;
- severity of pathology;
- correctness and timeliness of treatment, etc.
As such, prevention of this disease is general. It is very difficult to specifically prevent retinal detachment, since this pathology can be caused by many factors: you cannot foresee all of them.
General recommendations are as follows:
- regular visits to the ophthalmologist’s office for preventive examination of the visual organs;
- timely treatment of myopia;
- prevention and treatment of head and eye injuries;
- refusal to drink alcohol and smoke;
- avoiding strenuous sports that could theoretically lead to injury;
- timely treatment of chronic diseases, especially diabetes and hypertension.
As a measure that can help reduce the risk of this problem, we can recommend consuming natural honey on a regular basis. This product contains a high content of vitamins and microelements that are beneficial for vision; honey will help the whole body as a whole.
People with a history of chronic diseases such as diabetes, retinal dystrophy, myopia, and head injuries should regularly visit an ophthalmologist, as they are at risk. Heavy physical activity and eye strain are contraindicated in this case.
Diagnostic methods
If retinal detachment is suspected, the patient undergoes the following diagnostic measures:
- Determination of visual acuity and refraction. A significant decrease in visual acuity that cannot be corrected is characteristic of central retinal detachment.
- Perimetry and campimetry. Allows to identify narrowing of visual fields, the presence of absolute or relative scotomas. Based on the location of the scotoma, the location of the detachment can be approximately determined.
- Measuring intraocular pressure. As a rule, this pathology is characterized by a slight decrease in IOP.
- Direct and indirect ophthalmoscopy, bioophthalmoscopy with a Goldmann lens. The examination is carried out after preliminary medicinal dilation of the pupil. Allows you to see in the fundus a picture characteristic of a detachment - a raised portion of the retina, its grayish tint and wavy surface. Dystrophic changes, ruptures and hemorrhages may also be visible.
- Ultrasound examination (b-scan). It is carried out in cases where ophthalmoscopy cannot be performed or the data obtained was insufficient (for example, with cataracts, severe clouding of the cornea).
To clarify the diagnosis, optical coherence tomography, fluorescein angiography, electroretinography, CT or MRI may be prescribed.
If the detachment was preceded by a traumatic brain injury, additional consultation with a neurologist or other specialists may be required.
Classification
When studying the problem, it is worth deciding which category the disease belongs to, since the likelihood of recovery depends on a full-fledged study in the right direction. According to the source of occurrence, retinal dissection is divided into four types:
- Traumatic. Violations occur due to physical damage to the head through bruise, blow, fall or foreign object entering the eye cavity,
- Exudative or serous. The anomaly comes as a result of the destructive activity of another disease of the entire body. Among them: syphilis, toxoplasmosis, choroidal melanoma and many others,
- Traction. A common cause of detachment, since the “culprits” for the detachment of the layer from the vitreous body are the adhesions between them. Tension and deformation of tissues leads to destructive processes,
- Rhegmatogenous. The most common cause is age-related changes, which begin to appear at the age of forty and are often found in older people. The problem manifests itself in the form of breaks in the neuronal layer, due to which the area transmitting the picture does not communicate with the one that sends it to the brain. As a result, this type of retinal detachment occurs in 0.01 of the population.
There is also a classification according to the degree of distribution:
- total, the entire surface is peeled off,
- subtotal, no more than three quadrants are affected,
- common, up to two,
- local or partial, point changes.
Consequences
If retinal detachment occurred before pregnancy, but the woman did not pay attention to it, then pregnancy can greatly aggravate the situation and lead to tissue death. In this situation, unfortunately, even surgical intervention will not help and the possibility of restoring visual acuity is very small.
Pregnancy does not become an obstacle to eye surgery. The operation is usually safe for the baby. Laser coagulation of the retina is often performed, since for a pregnant woman this is the most convenient and fastest method of treatment.
Natural childbirth with retinal detachment is prohibited. At a later stage, the expectant mother is placed in a perinatal center so as not to miss the initial contractions, as this process causes straining, which can contribute to further injury to the retina. This precaution is taken to preserve vision.
If you are planning a pregnancy and you already know that you have retinal detachment, be sure to consult a doctor in order to know the current state of your vision.
IMPORTANT! You should plan a pregnancy only after one year after retinal surgery.
Reviews
Since laser surgery is most often used in the treatment of retinal detachment, the majority of reviews on the Internet are about this method of eliminating the pathology. Here are examples of reviews from those who have undergone this operation.
Olga, 43 years old, Rostov-on-Don: “Six months ago, my vision began to deteriorate sharply. Since my work involves a computer—I’m an accountant—I immediately noticed a deterioration in visibility. I went to the doctor and was diagnosed with retinal detachment. The ophthalmologist told me that I came in on time, since the disease progressed very quickly, just a couple more months, and I could say goodbye to my vision. Fortunately, I had surgery on time - they used a laser. My vision recovered quickly—in two weeks I was already able to work. I recommend this method of treatment because it is now the most effective and helps even with severe cases of retinal detachment.”
Natalya, 38 years old, Saratov: “My husband had retinal detachment last year. He was diagnosed during an annual medical examination - he himself would have put off going to the doctor until the last minute. Laser surgery was prescribed, since this pathology cannot be treated with medication. The intervention was successful, the husband managed to save his vision, and he also recovered quite quickly. I advise everyone to regularly visit an ophthalmologist and not be afraid to undergo laser surgery: this is the fastest and most effective way to restore vision.”
Why is retinal detachment dangerous?
The peeling process can last up to several years, and the person will not even suspect it. Phenomena such as “floaters” before the eyes, temporary blurred vision, light flashes are attributed by many to fatigue after work and do not turn to an ophthalmologist. Meanwhile, light-sensitive receptors die off. In 15% of cases, when detachment occurs, it also occurs in the second eye. And even surgical intervention is not a guarantee of the return of visual functions - this method can only stop the development of detachment or stratification, but not restore lost cells.
In advanced cases, these retinal pathologies result in complete blindness. That is why it is so important not to delay a visit to an ophthalmologist when symptoms appear in order to prevent irreparable consequences.
Traditional medicine against retinal detachment
Comprehensive measures make the treatment of retinal detachment more effective, so ophthalmological treatment is recommended to be combined with traditional medicine. She offers preventive methods and measures for the treatment of retinal avulsion that facilitate healing. Before using them, the patient must visit an ophthalmologist and obtain his permission to do so.
- Antihypertensive compounds reduce blood pressure (blood pressure) in the eyes.
- Antidiabetic drugs relieve symptoms of diabetes.
- Berries, vegetables, fruits and herbs, rich in vitamins and antioxidants, have a beneficial effect on the mesh tissue.
Let us list the most effective remedies from the arsenal of traditional medicine.
Blueberries and blueberries. They contain a lot of antioxidants, so they increase visual acuity. These berries will also be useful for visual impairments - myopia, retinal tears, glaucoma. Blueberries and blueberries can be eaten fresh or taken in capsule form.
Mistletoe. It is a strong antihypertensive agent that reduces eye pressure. To prepare the decoction, you need to infuse one teaspoon of the herb in 200 ml of boiling water. You should drink one glass of the product twice a day.
Blackberries. They contain a lot of vitamin C, which relieves inflammation. In addition, blackberries relieve swelling and reduce blood pressure inside the eyes.
Hawthorn flowers and leaves. They restore blood flow and normalize its pressure. To prepare the tincture, infuse one teaspoon of hawthorn flowers and leaves in 200 ml of boiled water. The decoction is drunk one glass twice a day.
Elder. This plant has anti-inflammatory properties. To prepare the decoction, boil two tablespoons of elderberry in one liter of water. The product is used as a lotion on the eyes.
Fennel. The seeds of this vegetable improve blood flow. Relieves inflammation and normalizes blood pressure. A decoction should be made from them - 40 grams of seeds per liter of boiling water. The product is used as compresses on the eyes.
Medicinal eyebright. This plant stops inflammatory processes. To prepare the decoction, you need to boil two tablespoons of the herb in half a liter of water. The product is used as a lotion on the eyes.
The favorable outcome of therapy largely depends on the location of the retinal detachment.
Prevention of retinoschisis and retinal detachment
Prevention of these diseases consists of regularly visiting a doctor, especially after 40 years, to check the fundus, peripheral vision, etc. If myopia is severe, high physical activity, extreme and traumatic sports should be avoided. With eye and head injuries, the risk of retinal detachment increases several times, and this may not happen immediately, but over a period of time. If this happens, then visiting an ophthalmologist for a check-up should become the norm. Patients with glaucoma need to monitor intraocular pressure and take medications on time.
Only a careful and careful attitude to eye health will help maintain good quality vision for many years. Regular visits to the doctor will help to detect many diseases in time and take appropriate measures.
Prevention
There are no specific methods for preventing retinal detachment. However, by adhering to certain rules, you can diagnose the pathological process in time:
- if the first symptomatic manifestations occur, seek medical help;
- in case of injuries to the visual apparatus, visit an ophthalmologist;
- in the presence of any infectious processes in the area of the visual organs, carry out timely treatment;
- if you are nearsighted or farsighted, you must visit an ophthalmologist at least once a year;
- avoid sudden lifting of heavy objects;
- beware of blows to the head;
- It is not recommended to overstrain the visual apparatus;
- control physical activity.
It is impossible to completely prevent detachment using prophylaxis, but it will be possible to notice the pathological process in time.
What is a retinal detachment?
Retinoschisis (as this pathology of the retina is called in medicine) is the division of the retinal layers into outer (choroidal) and inner (vitreal). Fluid accumulates between them and cysts form. Retinoschisis occurs as a result of developmental defects or dystrophic changes in the retinal membrane. In Europe, the incidence of the disease is approximately 5% in the population over 30 years of age. It is also inherited. The main problem of retinoschisis is its asymptomatic course; it is diagnosed accidentally or already in an advanced stage when complications arise.
Surgery
Since retinal detachment cannot be treated with medication (no injections, tablets or drops will help), the doctor is forced to prescribe surgery. Moreover, it needs to be done as soon as possible - the sooner the operation is performed, the greater the chances of successful treatment. This is the only way to save the patient’s damaged eye.
Scleral filling
The main task of surgical intervention is to determine the location of the retinal tear and ensure reliable adhesion between the membranes (between the retina and the choroid). For this purpose, different methods can be used, starting with retinopexy and ending with local filling. It all depends on the type and severity of the disease. Let's consider each of the methods separately.
Table. Surgical treatment of retinal detachment.
| Type of surgical therapy, photo | Description |
| Retinopexy | During the procedure, the doctor uses special surgical micronails made of sapphire. They are needed to securely attach the torn retina. This method is used in severe cases. That is, with large retinal tears. |
| Laser coagulation | One of the most common methods of treating retinal detachment. As a rule, laser photocoagulation is used to prevent an increase in the area of damage, as well as to fix thin areas of retinal tissue. |
| Vitrectomy | Another method of surgical treatment of retinal detachment, which involves removing the affected vitreous body. Then a special medical preparation (gas, perfluorocarbon compound, liquid silicone or solution) is injected in its place, engrafting the retina to the surface of the choroid. The injected drug affects the retina from the inside. |
| Circular filling | This method of treatment is used in rare cases when numerous breaks have appeared or in cases of complete detachment of the retina. Circular filling is a rather complex procedure. |
| Local filling | Unlike the previous method, local filling is used in medicine much more often. As a rule, it is used for partial retinal detachment. The procedure involves exposing the affected area to cold or a laser beam. |
Doctors often use several treatment methods at once. This may depend on the number and location of the tears, the size of the detachment and the time that has passed since the onset of the pathology. Also, certain methods can be carried out in several stages.
Recovery after surgery
Retinal detachment in children
Without pathogenic precursors, the highest percentage by source of occurrence is eye injury. The child does not immediately notice the changes, but over time begins to complain about a partial lack of ability to see from a certain side. Often the baby calls it a “black curtain” or “screen”, which appeared after distortion of the picture, metamorphosis of the image, or immediately after sleep. It is possible to restore vision; just as in treating adults, surgery will be required.