The mitral valve is located on the left side of the heart between the ventricle and atrium. It consists of valves, atrioventricular ring, papillary muscles and chordae tendineae. The chordae tendineae and papillary muscles act as springs that hold the valves, preventing them from opening into the atrium. All mitral heart defects can be divided into mitral stenosis, insufficiency and prolapse.
How are all heart valves supposed to work?
Normally, the heart contracts rhythmically. In one cardiac cycle, systole (contraction) and diastole (relaxation) of the heart muscle occur. Atrial contractions cause blood to flow through the open valves and into the ventricles. The period of ventricular contractions coincides with the relaxation of the atria; the atrioventricular valves slam shut, preventing blood from flowing backward. Through the open aortic and pulmonary valves, blood is distributed through the vessels of all organs. In diastole, the pressure in the cavities of the heart decreases, which contributes to the filling of the right and left atria with blood, and the cycle begins anew. When the functioning of the valves is impaired, defects develop - insufficiency, stenosis, prolapse of the valves.
Complications
Malfunction of the valve apparatus leads to a change in blood flow in the parts of the heart, which causes a disorder of the circulatory system. Long-term development of the disease provokes stagnation in the pulmonary and systemic circulation.
Complications associated with PPS:
- enlargement of the right ventricle;
- enlargement of the right atrium;
- enlargement of the left ventricle.
Long-term consequences of the development of acquired heart defects:
- failure of cardiac activity, first in a compensated form, and then in a decompensated form;
- heart failure.
Mitral valve insufficiency
Mitral regurgitation is a defect of the mitral valve, leading to abnormal blood flow during heart contraction from the ventricle to the atrium. According to statistics, there is a high frequency of diagnosing this pathology. Very rarely isolated (0.6% intrauterine malformations). Diagnosis of mitral regurgitation at birth must exclude damage to other structures. Stenosis and insufficiency occurring simultaneously in one patient is called combined mitral heart disease. A combination of aortic defects and mitral valve insufficiency is often observed.
Symptoms, signs and chief complaints of patients
The clinical picture of the disease depends on the type of the defect itself, the degree of disturbances in intracardiac and systemic hemodynamics, the duration of the pathological process and the level of problems from other organs and systems.
In the compensation stage, which occurs without signs of heart failure, patients do not complain about their health and may not come to the doctor’s attention for a long time. And only with the development of decompensation the following complaints and signs appear:
- shortness of breath – associated with increased pressure in the pulmonary circulation (PCC);
- hemoptysis - due to sweating of blood cells with pronounced stagnation in the veins of the ICC;
- dull cardialgia;
- interruptions in the functioning of the cardiac system - palpitations, arrhythmias, atrial fibrillation, extrasystoles.
Combined (not combined) mitral valve disease very quickly decompensates, as a result of which it is accompanied by stagnation of blood in the systemic circulation, which clinically manifests itself as swelling of the neck veins, heaviness in the right hypochondrium and enlargement of the liver (hepatomegaly), edema of the lower extremities.
Symptoms
With minimal structural changes in the valve, patients feel well. Pathology is diagnosed when visiting a doctor. With moderate damage, fatigue, palpitations, a feeling of incomplete inhalation/exhalation, blood when coughing, pain in the heart area occur. Some patients experience attacks of cardiac asthma, often at night. With decompensation, heart failure of the right ventricular type develops. Its signs include peripheral edema, cyanosis of the earlobes, fingertips, nose, enlarged liver, ascites formation, and swollen neck veins. The heart muscle may also suffer and manifest itself in the form of rhythm disturbances (atrial fibrillation).
https://youtu.be/GBkImRIfjyY
Causes and risk factors
Reasons for the development of defects:
- inflammation: rheumatic heart disease, infective endocarditis;
- degenerative processes: Marfan syndrome, mitral annulus calcification;
- systemic diseases: systemic lupus erythematosus, rheumatoid arthritis;
- structural changes: rupture of chordae, tear of papillary muscles;
- congenital disorders: deformation of the bicuspid valve due to connective tissue abnormalities.
Risk factors for MP:
- gender (women are more likely to suffer from pathology);
- chronic tonsillitis;
- genetic predisposition (relatives of SLE, rheumatoid arthritis);
- severe concomitant diseases that reduce immunity (HIV, oncology, diabetes).
Forms
There are congenital and acquired failure, as well as organic (changes in its structure) and functional (expansion of the ventricular cavity in other heart pathologies). Taking into account the amount of blood returning to the atria (regurgitation), a certain degree is distinguished:
- 1 (with slight mitral regurgitation) less than 20% of stroke volume;
- 2 (moderate) 20 – 40% of stroke volume;
- 3 (pronounced) 40 – 60% of stroke volume;
- 4 (severe) more than 60% of stroke volume.
Depending on the clinical picture, 3 stages are distinguished - compensation, subcompensation, decompensation.
According to the ICD X (International Classification of Diseases), mitral regurgitation is coded I05.8 for non-rheumatic lesions and I05.1 if the disease is rheumatic in nature.
Forecast
The consequences of a combined defect can be predicted taking into account age, gender, previous diseases, severity of the lesion and other factors.
A mild form of valve damage does not have a significant impact on the quality and life expectancy. If you consult a doctor in time and undergo a course of treatment, reduce the intensity of physical activity, and avoid stressful situations, then you can lead a completely normal lifestyle.
The consequences of the disease will be much worse for children and men. The greatest danger is aortic insufficiency. Mitral regurgitation has a more positive outcome.
The outcome of the pathological condition worsens significantly if a person suffers from diseases of infectious origin, sepsis, rheumatism, tuberculosis.
If you refuse surgery or do not carry out treatment in a timely manner, you cannot count on a favorable prognosis.
Five-year survival is observed in 40% of patients. Only 6% of patients manage to live ten years with this diagnosis.
If a patient has a damaged valve replaced, the chances of survival increase significantly. In this case, 85% of patients live more than five years.
Mitral valve prolapse
Mitral valve prolapse refers to the protrusion of the leaflets during contraction of the ventricles into the atrium. It is more often detected during a preventive examination by a pediatrician of a child, less often in adults. There is a predominance of the development of prolapse in women compared to men. Among the entire population, the frequency of occurrence varies from 15 to 25%.
The causes of primary prolapse may be fetal developmental abnormalities. In case of secondary – as a consequence of past or chronic diseases, it includes:
- cardiodilation;
- sternum injuries;
- hereditary diseases and chromosomal mutations;
- fetal development abnormalities;
- rheumatic lesion
Patients usually have no complaints. But there may be a feeling of lack of air, increased body temperature for no reason, dizziness, fainting, frequent headaches, tachy/bradycardia, chest pain. These symptoms are not specific, but they can help the doctor make the correct diagnosis.
Development mechanism
Typically, defects of the left AV valve are formed due to acute rheumatic fever. After relapses of the disease, the valves are even more affected. Fibrous and sclerotic changes appear, as well as calcification of the valves. The left atrioventricular orifice becomes scarred and narrowed.
All these changes are reflected in hemodynamics. Hypertrophy and expansion of the LA and both ventricles develop. In the pulmonary circulation, stagnation increases and pulmonary hypertension forms. Manifestations of right ventricular failure are formed. Cardiac output becomes lower, which is especially noticeable during physical activity.
Stenosis - what is it, reasons for its development
Mitral stenosis is a heart defect in which the area of the atrioventricular orifice on the left decreases. The valves change, they become thicker or grow together. In 80% of cases, rheumatic mitral valve disease is the main cause of prolapse. Other reasons include:
- atherosclerosis, large thrombus in the heart cavity;
- syphilis;
- infective endocarditis;
- heart injury;
- neoplasms of the heart muscle (myxoma);
- as a complication of rheumatological diseases.
Diagnostics
In order to make a diagnosis of any pathology of the mitral valve, it is necessary to comprehensively evaluate the patient’s complaints, survey data (possibly previous rheumatic heart disease), objective examination (auscultation) and additional studies.
The appearance of a patient who has rheumatic mitral valve disease has the following signs:
- the typical patient has an asthenic physique with undeveloped muscle mass and cold upper extremities;
- cyanosis of the lips, chin, nose, ears, combined with a bright bluish-pink blush on the cheeks and pallor around the eyes (due to dilation of skin vessels and prolonged hypoxemia).
The auscultatory picture of mitral defects is quite bright and a competent specialist who knows this method can easily suspect this pathology.
Results of instrumental examinations
Electrocardiography (ECG) helps to identify thickening or damage to the myocardium, detect changes in the size of cavities, and verify arrhythmias.
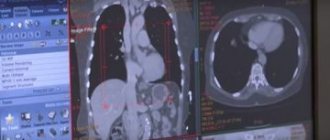
X-ray of the chest cavity is important for diagnosing dilatation of the cavities of the heart and the severity of damage to the bronchopulmonary tree.
However, the “gold standard” for detecting heart defects is echocardiography. The value of ultrasound examination is determined by the fact that it allows not only to identify the degree of narrowing or widening of the atrioventricular opening, to evaluate the anatomy of the valves themselves, but also provides data on intracardiac circulation.
Symptoms
The clinical picture of valve damage appears when the area of its opening changes to less than 2 cm. The presence of stenosis can be suspected by the following symptoms:
- shortness of breath with exertion, with progression of the disease - at rest;
- fatigue;
- pain in the heart area;
- hemoptysis;
- feeling of heartbeat;
- arrhythmia.
In severe cases of the disease, attacks of cardiac asthma develop. They can be provoked by psycho-emotional stress.
The description of the appearance of a patient with an advanced course of the disease is quite specific. It is characterized by flushed cheeks with a bluish coloration of the nails and the tip of the nose. As the disease progresses, signs of right ventricular failure (liver enlargement, ascites, edema) appear.
Reasons to see a doctor
Mitral disease of moderate severity is asymptomatic for many years. Then the complaints appear:
- shortness of breath on exertion, during fever, or during emotional excitement;
- nocturnal attacks of suffocation, forcing the patient to sit up in bed;
- cough streaked with blood, heaviness in the chest;
- dizziness, fainting;
- fast fatiguability.
Complaints with valvular insufficiency:
- gradually increasing weakness, shortness of breath;
- difficulty breathing at night;
- Sometimes blood appears when coughing.
If such symptoms appear, you should consult a cardiologist. Urgent medical care is required for the development of a heart attack, stroke, atrial fibrillation, or acute circulatory failure.
Diagnostic methods and principles of treatment of mitral valves
When examining a patient with mitral valve damage, the doctor performs auscultation. At the same time, he pays attention to the specific auscultatory noise in the heart area. Heart murmur, as a symptom of its damage, is an indication for a comprehensive examination. If mitral valve disease is suspected, the following is performed:
- ECG;
- chest x-ray;
- echocardioscopy;
- consultation with specialized specialists (cardiac surgeon, cardiologist).
Other studies may also be prescribed depending on the degree of valve damage and the presence of other diseases in the patient.
If a defect is detected - mitral regurgitation or stenosis, at the stage of minimal changes, conservative therapy and dynamic monitoring of the patient's condition are prescribed. Drug treatment must be combined with surgical treatment. Therapy uses antiarrhythmic drugs, anticoagulants (to prevent thromboembolic complications), as well as drugs that help eliminate the root cause of the disease.
Isolated and combined mitral heart defects always require surgery - the only question is when. Indications for surgical treatment are:
- signs of heart failure of functional class III – IV, which developed against the background of the defect;
- 2 – 3 stage of regurgitation;
- severe sclerosis, deformation of the valve leaflets;
- ineffective treatment of rheumatic carditis, infective endocarditis.
Among the options for surgical interventions are valve-sparing (comisorotomy for stenosis, comessuroplasty for insufficiency) and valve replacement.
After surgical treatment, the affected valve is sent to the pathological department for examination. In case of insufficiency, the macropreparation contains foci of fibrosis and proliferation of vegetations; in case of stenosis – fibrosis and thickening of the walls of the mitral ring.
For mild mitral valve prolapse, no treatment is required; for severe valve prolapse, beta-blockers are prescribed. These patients undergo annual examination with mandatory cardiac ultrasound.
Prognosis for patients with stenosis
Even mild mitral stenosis gradually progresses due to repeated rheumatic episodes. Subsequent death of patients occurs from thromboembolic complications (heart attack, stroke), as well as against the background of heart failure. Timely surgery improves the survival of such patients.
Mitral insufficiency does not bother the patient for many years, and then slowly progresses. The cause of death was heart failure.
We recommend reading about the complications of myocardial infarction. You will learn about the stages of myocardial infarction, classification of complications, their treatment, and preventive measures. And here is more information about shortness of breath in heart failure.
Prevention and prognosis of the disease
With early detection of mitral valve defects, a favorable course of the disease is observed. Preventive measures are aimed at timely treatment of isolated and combined mitral valve defects, as well as the prevention of diseases leading to its development. The presence of a diagnosed defect requires correction of the work and rest regime, diet and water regime.
Consequently, timely diagnosis of heart defects of the mitral or other valves, as well as their treatment, helps to reduce the number of complications and improve the patient’s life. Be healthy!
https://youtu.be/l-9U6n-nDTM
Clinical guidelines
Doctors are trying to delay the progressive damage to the urinary tract. They compiled a list of measures that will help patients prevent relapses and improve their quality of life.
What do we have to do:
- Avoid hypothermia and intense physical activity.
- Be examined regularly—at least once a year—to monitor symptoms of the disease.
- Carry out preventive measures for recurrent infections with medications prescribed by your doctor.
- Limit the consumption of liquid and table salt.
- If you experience causeless fatigue, shortness of breath, hemoptysis, fever, swelling of the legs, or shortness of breath at night, consult a doctor immediately.
Modern cardiologists are confident that a defect detected in time and not neglected may well be curable , even with the help of such seemingly harmless surgical methods. But the main thing is not the method of treatment, but its result.
How do specialists detect mitral valve disease?
To do this, first of all, doctors listen to the heart using a phonendoscope. Both mitral stenosis and mitral regurgitation are accompanied by a certain sound pattern, on the basis of which the doctor may suspect this disease, even if the patient feels well at that time.
After this, it will be necessary to undergo an echocardiographic examination, which allows not only to identify the defect with a high degree of accuracy, but also to assess the severity of the hemodynamic disorder.
Additionally, chest radiography, ECG, general clinical and biochemical tests of blood, urine, phonocardiogram, etc. are prescribed.
Treatment tactics for isolated MPCs
When the pathology is compensated, it is advisable to reduce intense physical activity. Conservative therapy is necessary to control the symptoms of the disease during preparation for surgical treatment.
The main groups of drugs prescribed for treatment:
- diuretics: prescribed to reduce LA pressure. They alleviate the signs of the disease associated with congestion in the pulmonary circulation;
- beta blockers: reduce heart rate at rest and during exercise, prolong diastole. This helps improve LV filling;
- indirect anticoagulants: reduce the risk of pulmonary embolism;
- antibiotics and antirheumatic drugs: to prevent relapses of provoking diseases and infectious complications;
Drug therapy also has the following goals:
- preventive – prevent the development of complications and relapses of the disease;
- palliative – improve the patient’s quality of life if immediate radical intervention is not possible.
Operation
Surgical treatment for MP:
- Reconstructive plastic surgery on the valve, during which anatomical defects that impede its normal functioning are eliminated. They are performed both minimally invasively (percutaneous balloon valvuloplasty in case of stenosis) and on an open heart (commissurotomy - separation of adhesions in case of valvular stenosis).
Patients who have undergone this type of surgery do not require lifelong anticoagulant therapy. Unfortunately, if the disease is the result of rheumatic lesions, this type of operation is practically impossible.
Causal factors of combined cardiac defects
Various combinations of cardiac anomalies arise due to typical internal and external factors. Any combined type of heart defect appears against the background of:
- rheumatism;
- infective endocarditis;
- atherosclerotic disease;
- congenital and genetic abnormalities;
- degenerative changes in the valve apparatus.
In the vast majority of cases, the main cause of a combination of several cardiac defects occurs with rheumatic inflammation. Congenital combined defects are detected in utero or immediately after the birth of a child, often leading to the death of the baby.
Etiopathogenesis
Mitral valve insufficiency
Mitral valve insufficiency is a common valvular heart disease. This defect occurs in 50% of patients with various heart defects, and in children it is observed much more often than in adults. In its pure form, mitral valve insufficiency is less common; it is usually combined with mitral valve stenosis or other heart defects.
Etiology:
- Rheumatism
- Infective endocarditis
- Myocarditis
- Post-traumatic mitral valve defects.
- Heart tumors
In the initial stage of the rheumatic process, the tissues of the mitral valve leaflets are destroyed and marginal defects are formed, as a result of which the leaflets do not completely close during left ventricular systole. Subsequently, during the sclerotic stage of the rheumatic process, the chords are shortened and fused, which leads to limited mobility of the valve leaflets and the formation of subvalvular stenosis. Often the commissures also become welded together, forming a combined mitral defect.
With mitral valve insufficiency caused by infective endocarditis, there are marginal tissue defects, as well as perforation of the leaflets. A detachment of chords is often detected, and at the ends of the rupture there may be fresh or already calcified vegetation.
Photo. Removed mitral valve. The mitral valve is affected by infective endocarditis. The valve is corroded along the edges, the valve chords are torn off, vegetation is growing.
Ischemia or infarction of the papillary muscles due to coronary heart disease can contribute to sclerosis and, less commonly, rupture of one of the papillary muscles, which causes acute mitral valve insufficiency.
Violation of the structure of collagen and elastin, myxomatous degeneration of the valves are manifested in the lengthening of the chords of the anterior and posterior leaflets, and an increase in the area of the latter. This often leads to spontaneous rupture of the mitral valve chords.
An obligatory component of pathological changes in mitral valve insufficiency is dilatation and deformation of the fibrous ring. Thus, mitral valve insufficiency is usually associated with a complex dysfunction of several of its elements.
Hemodynamic disturbances in mitral valve insufficiency depend on regurgitation of blood into the atrium during left ventricular systole. Backflow into the left atrium appears during the systolic ejection phase and continues into the isometric relaxation phase, since during these periods the pressure in the left ventricle exceeds the pressure in the left atrium. Due to the flow of increased blood volume, the myocardium stretches and, accordingly, the systole of the left atrium becomes more powerful. Due to the poorly defined muscle layer, the atrium cannot work for a long time under increased load. Its dilatation occurs and it begins to function as a cavity with low resistance, accommodating a large volume of blood without a significant increase in phase and average pressure. At the end of the left ventricular filling phase, the volume of the left atrium still remains significantly increased due to the influx of blood from the pulmonary veins and the volume of regurgitation from the left ventricle.
To maintain adequate cardiac output, the left ventricle is forced to eject an increased volume of blood during systole—the effective stroke volume of blood returning to the left atrium. A powerful left ventricle can compensate for mitral valve insufficiency for years.
An increase in pressure in the left atrium leads to its dilatation, which is accompanied by incomplete closure of the mouths of the pulmonary veins and, as a result, stagnation of blood in the pulmonary veins is added to stagnation of blood in the atrium. The increase in pressure in the left atrium is transmitted to the pulmonary veins and pulmonary capillaries. This is largely due to the increase in end-diastolic pressure in left ventricular failure. Pulmonary hypertension with mitral valve insufficiency is caused not only by passive pressure transmission, but also by reflex narrowing of the pulmonary veins.
With mitral valve insufficiency, pulmonary hypertension develops slowly. It occurs during the transition to the stage of decompensation, being a factor that sharply aggravates the patient’s condition.
In later stages of mitral valve insufficiency, an increase in pressure in the pulmonary artery system leads to hypertrophy of the right ventricle, and then to decompensation with the development of relative tricuspid valve insufficiency, liver enlargement, the appearance of peripheral edema, and ascites.
Long-term circulatory disorders lead to persistent changes in the lungs (shortness of breath with minimal physical exertion and at rest, dry cough at night, worsening in a horizontal position), liver, kidneys and other organs.
Mitral valve stenosis
Mitral stenosis, or narrowing of the left atrioventricular orifice, is the most common rheumatic heart disease. It is characterized by fusion of the edges of the mitral valve leaflets. At the same time, cicatricial contraction of the edges of the valve leaflets and valve ring, changes in subvalvular structures, and deposition of calcium masses are possible. The normal area of the mitral orifice is 4-6 cm2.
Isolated mitral stenosis occurs in 1/3 of cases of all mitral valve defects. The defect usually forms at a young age and is more often observed in women.
Valve defects are based on sclerotic processes, which involve the leaflets, annulus fibrosus, chordae and papillary muscles. Mitral valve stenosis begins with gluing of the edges of the leaflets in contact with each other, primarily at their poles adjacent to the fibrous ring, where their mobility is limited. Thus, two commissures are formed, which, spreading from the ends of the valves to the center, cause an increasingly narrowing of the opening.
Photo. Removed mitral valve. Mitral valve stenosis. The effective hole area is less than 0.5 cm2.
The resistance to blood flow created by the narrowed mitral orifice activates compensatory mechanisms that ensure sufficient cardiac performance. Due to blood overflow in the left atrium, the pressure increases several times. Since the left atrium is a rather weak part of the heart, it early stops coping with the increased load. The increase in pressure in it is transmitted to the pulmonary veins, and then to the pulmonary capillaries and terminal branches of the pulmonary artery. Due to the sharp weakening of the muscles of the left atrium, its contraction becomes ineffective. At the same time, due to overstretching of the walls of the atrium, damage and scarring of the conduction systems of the heart as a result of the rheumatic process, the normal rhythm of the heart is often disrupted and atrial fibrillation occurs (atrial fibrillation), contractions of the left atrium become completely ineffective. This leads to stagnation of blood in the pulmonary circulation and even greater expansion of the cavities, which creates conditions for thrombus formation.
Photo. Removed thrombus from the left atrium in a patient with critical mitral valve stenosis.
The formation of blood clots in the left atrium can lead to thromboembolism in the brain with the development of extensive strokes.
As a result of increased pressure in the pulmonary artery, compensatory hypertrophy of the right ventricle and then the right atrium develops. Subsequently, an increase in pressure in the pulmonary artery, as well as the development of myocardial wear syndrome, causes the appearance of signs of right ventricular failure and relative tricuspid valve insufficiency.
Mitral valve replacement is indicated when, in the presence of mitral stenosis or insufficiency, preservation of the native valve is impossible. To perform this operation under artificial circulation, access is made through the left atrium, and the affected mitral valve is removed. After the valve is removed, a mechanical or biological prosthesis of a suitable size is installed in its place. The left atrium is deflated and the left atrium is sutured.
What are the indications for surgical treatment of mitral stenosis?
The operation is indicated for all patients with mitral stenosis with symptoms of heart failure (shortness of breath, peripheral edema, decreased ability to work, fatigue, cardiac arrhythmias, thromboembolism). For asymptomatic mitral stenosis, surgery is indicated for:
- pulmonary hypertension
- episodes of pulmonary edema
- atrial fibrillation (atrial fibrillation)
Indications for surgical treatment of mitral valve insufficiency
- Severe manifestations of the disease
- Severe left ventricular dysfunction Pulmonary hypertension
- Blood regurgitation on the mitral valve of grade 3 or more.
Indications for surgical treatment are assessed individually for each patient after a full comprehensive examination.
Surgical treatment of mitral valve defects consists of replacing it with an artificial prosthetic heart valve or its plastic surgery. There are 2 types of heart valve prostheses, biological and mechanical.
What are acquired heart defects?
The heart consists of two ventricles and two atria located above them.
The heart chambers are separated from each other by valves that release blood from the atria into the ventricles and prevent it from flowing back. Between the right ventricle and the atrium is the tricuspid tricuspid valve, and between the left ventricle and the atrium is the bicuspid mitral valve. Both valves are held in place by threads - chordae tendineae - and close after blood is expelled into the ventricles.
For the smooth functioning of the heart, it is important that there is no regurgitation (backflow of blood), so the valves close tightly and do not allow blood back into the atria. There are two more valves - the aortic valve, which divides the left ventricle and the aorta, and the pulmonary valve, which separates the trunk of the pulmonary artery and the right ventricle.
These valves prevent blood from flowing back into the ventricles.
Aortic valve defects
Combined aortic disease is usually formed against the background of rheumatism or infective endocarditis. Clinical features of a valve defect are the following:
- severe shortness of breath;
- phenomena of venous stagnation in the lungs;
- absence of pronounced manifestations of aortic regurgitation (drop in blood pressure, cold sweat, suffocation);
- dicrotic (two-peak) pulse.
Against the background of the predominance of aortic valve insufficiency, a loud diastolic murmur, weakened 2nd tone and high-amplitude pulse changes are more pronounced. Auscultatory features with predominant aortic stenosis are weakened 1st and 2nd sounds, loud systolic murmur and slow pulse wave.
An experienced cardiologist, when listening to the heart, will be able to distinguish a combined aortic defect with a predominance of stenosis or valvular insufficiency.
Classification
Based on the time of occurrence, they are distinguished:
- congenital;
- acquired MPS.
Based on structural and functional disorders:
- mitral stenosis;
- MK insufficiency;
- MK prolapse.
Experts also distinguish between compensated, subcompensated and decompensated defects (the clinical picture depends on how the heart function “adjusts” to the corresponding changes in the muscle), as well as combined MVP (for example, aortic ones are combined with mitral defects, stenosis is accompanied by valvular insufficiency, etc. .).
Congenital pathologies
The development of the fetal heart occurs in the middle of pregnancy and this process can be negatively affected by many circumstances. The cause of heart defects in newborns can be both genetic abnormalities and disturbances in the normal development of the fetus as a result of exposure to external factors:
- toxic substances;
- deviations during pregnancy;
- maternal smoking or drinking;
- uncontrolled use of medications by the mother;
- radiation;
- lack of vitamins or, conversely, vitamin poisoning;
- viral infections suffered by the mother, for example, rubella.
Substances that are mutagenic and affect the likelihood of developing heart defects in a child include:
- NSAIDs,
- phenols,
- nitrates,
- benzopyrene
Often the cause of the disease is both factors - genetic and external.
Factors contributing to the development of heart defects in the fetus: chronic maternal diseases (diabetes mellitus, phenylketonuria, autoimmune diseases), a large number of abortions in history. Also, as the age of the parents increases, the likelihood of abnormalities in the development of the fetus’s heart also increases.
The incidence of certain birth defects varies by gender. Some congenital heart defects are more common in boys, others in girls, and others occur in both sexes with approximately equal frequency.
Predominantly female congenital pathologies include:
- Fallot's triad,
- atrial septal defect,
- patent ductus arteriosus,
Predominantly male congenital heart disease:
- common arterial trunk,
- coarctation or stenosis of the aorta,
- tetralogy of Fallot,
- transposition of the great vessels.
The most common type of birth defect is a ventricular septal defect. However, an atrial septal defect may also occur.
Often there is such a congenital pathology as patent Botallov duct. This defect leads to the fact that arterial blood is discharged into the pulmonary circulation.
Experts' forecast
Most often, to ensure the survival of a patient with advanced concomitant heart disease, timely and competent surgical intervention is necessary. To give an accurate prognosis for future life, a specialist should take into account the following factors:
- type and severity of pathology;
- patient's age;
- presence of complications.
A combined defect has a more favorable prognosis. A mitral defect often involves serious difficulties in treatment, since in the left chambers the heart muscle does not have the ability to maintain a state of compensation for a long time. The further prognosis of the disease is greatly influenced by the presence of complications, in which a serious hemodynamic disturbance is possible, the load on the heart increases, or a relapse of rheumatism is observed.
Main causes of PPP
The following conditions may act as etiological factors for acquired heart defects in adults and children:
- Bacterial endocarditis. One of the outcomes of this disease, manifested by inflammatory processes in the endocardium, is the formation of heart defects.
- Rheumatism. An acute inflammatory disease of a systemic nature, mainly affecting the articular and cardiovascular systems. The cardiac form of rheumatism is explained by the toxic effect of streptococcal enzymes (the causative agent of this disease) and the formation of autoimmune reactions that affect the endocardium and myocardium.
- Syphilis. One of the manifestations of this systemic disease is damage to the valvular apparatus of the heart and aorta.
- Atherosclerosis. A chronic pathology manifested by the formation of plaques on the walls of blood vessels, causing them to narrow.
- Injuries. The outcome of bruises and wounds of the heart can be formed defects.
- Sepsis. Any generalized infection can lead to disruption of the heart valve apparatus.
Separately, it should be said about acquired heart defects and pregnancy. In the second and third trimesters, expectant mothers have an increased risk of exacerbation of chronic pathologies. Therefore, pregnancy may also be one of the factors that increases the likelihood of the formation of valvular lesions.
Modern treatment methods
In the early stages of the disease, conservative therapy is carried out. Its goal is to prevent various complications and relapses of rheumatic phenomena and prevent infective endocarditis.
https://youtu.be/KPvg2A2pjQk
In the presence of serious pathologies, surgical intervention is necessary. Modern cardiology centers perform a number of operations, the purpose of which is to treat combined heart disease. We are talking about the following procedures:
- plastic cardiac surgery, which involves restoring normal heart functions;
- replacement of the affected valve with a biological prosthesis;
- valve-sparing operations;
- for the left atrium, atrioplasty can be used;
- coronary artery bypass grafting;
- surgery aimed at restoring sinus rhythm.
After surgery, patients undergo a therapeutic course, which depends on the degree of the disease. Sanatorium treatment involving cardiology is recommended.
Preventive measures
With this pathology, the patient is prohibited from significant physical activity and serious sports training. It is necessary to completely give up bad habits and follow all doctor’s instructions. It is advisable to systematically undergo sanatorium treatment, regular classes in specialized gymnastics and walking.
A good preventive measure is general hardening of the body in order to increase immunity and prevent frequent diseases. Even a serious cold puts a certain strain on the heart, so comprehensive wellness is very important to prevent the development of the disease. For patients with a combined defect, it is advisable to eat mainly protein foods, drink fluids in moderation and limit salt intake.
Combined and combined heart defects are serious diseases that require timely detection and competent treatment. Most patients with these problems require surgery. If the disease is at an early stage, then conservative methods can be used.
https://youtu.be/eEkD4-7iJyU
Is it deadly?
This question can only be answered for each specific case.
Of course, in some cases of congenital or acquired defects, medicine is not able to help the patient. However, often a person lives with the disease for decades and does not even know it. Sometimes only surgery can help, and sometimes conservative treatment will be sufficient.
According to severity, myocardial defects are divided into those that do not have a serious effect on hemodynamics, defects of moderate severity and pronounced ones.
The presence of most defects is grounds for disability.
The consequences of vices can be:
- heart failure,
- bacterial endocarditis,
- chronic pneumonia,
- pulmonary failure,
- myocardial infarction,
- stroke,
- angina pectoris
- dyspnea,
- cyanosis,
- anemia,
- rhythm disturbances,
- thromboembolism.
Many of these complications can lead to death.
In addition, almost any myocardial defect, even compensated, leads to the heart wearing out prematurely, and therefore to a reduction in life expectancy. If surgery is performed in a timely manner and the patient has successfully completed the rehabilitation course, then the likelihood of serious complications is reduced.
Combined defects
There are different combinations of pathologies that develop in the heart valves. Typically, the disease affects the mitral and aortic valves, resulting in their simultaneous insufficiency, or stenosis develops in one valve and insufficiency in the other.
Combined heart valve defects have a mutually enhancing or, conversely, weakening effect. For example, with sufficiently severe aortic stenosis, mitral regurgitation will manifest itself in a more severe form. Pronounced mitral stenosis mitigates the signs of aortic insufficiency.
Combined aortic disease is characterized by narrowing of the aortic ostium and valvular insufficiency. The patient develops ischemia of the brain and heart. Headaches and heartaches appear. The cause of the disease is most often infective endocarditis.
To determine a more accurate clinical picture, it is necessary to undergo an examination. The diagnostic results will show exactly what pathological processes occur in the heart valves.
Diagnostic procedures
The initial picture of the disease is based on a conversation between the patient and the doctor. The specialist is interested in what symptoms the patient experiences after physical activity, and also monitors the patient’s condition at rest.
An experienced specialist can already distinguish at the listening stage which defect is more pronounced: stenosis or valve insufficiency.
Before starting treatment, you will need to identify the source of the disease, find out what exactly led to the development of the pathology: rheumatism or another disease.
Diagnosis is carried out using the following methods:
- palpation;
- external examination for the presence of cyanosis (blue discoloration of tissues), swelling of the legs, shortness of breath;
- 24-hour ECG monitoring to identify the degree and type of cardiac arrhythmia;
- Echo-CG will help determine the condition of all valves;
- physical stress tests under the supervision of a cardiologist-resuscitator;
- using X-rays, they determine whether there is pulmonary congestion, whether myocardial hypertrophy is present, the type of defect is diagnosed, and a chest photograph is taken in two projections;
- phonocardiography records systolic and diastolic murmurs in the heart, registers cardiac tone;
- cardiac output is measured using echocardiography;
- cardiac catheterization makes it possible to detect concomitant ailments and measure pressure in the atria and ventricles;
- laboratory tests show the presence of sugar, cholesterol, total protein levels in the blood;
- Blood and urine tests are prescribed to identify inflammatory processes.
Is it possible to suspect mitral valve disease at home?
If the condition of an adult or child with mitral valvular disease is not impaired, then it is difficult to suspect the disease on your own, but you should pay attention to existing complaints or behavioral characteristics in order to promptly show such a person to a specialist.
In children, the presence of mitral valve disease can be noticed immediately after birth, as well as during periods of most intensive growth, for example, in the first year of life or in adolescence.
Babies latch on weakly, suck sluggishly, and their fingertips may turn blue. Having become a little older, such children prefer not to play outdoor games at all or often squat down and rest. A cough, especially at night and not going away with treatment with conventional means, some retardation in growth and physical development may also indicate a defect.
In adolescence, exercise tolerance during physical education, especially running and other athletics exercises, worsens; there is an increased heart rate, increased heart rate, shortness of breath, cough, increased fatigue and an increased need for physical rest.
In adults, mitral disease can be suspected by a constant blush on the cheeks (“mitral blush”), shortness of breath, night cough and periodic attacks of suffocation (the picture may vaguely resemble an attack of bronchial asthma with the only difference that there is no whistling and narrowing of the lumen of the bronchi). The appearance of swelling in the legs is another serious reason to immediately consult a doctor.