Croup in children (stenotic laryngitis) is a clinical syndrome that occurs as a complication of certain infectious and inflammatory diseases of the upper respiratory tract and is manifested by inspiratory shortness of breath, barking cough, and hoarseness.
Source: uzi-center.ru
Croup is most often observed in children under 6 years of age. This is due to age-related features of the structure of the larynx (loose submucosal tissue, cone-shaped) and its innervation.
Causes
Croup in children develops against the background of infectious and inflammatory diseases accompanied by damage to the mucous membrane of the pharynx and trachea, for example, with influenza, adenovirus infection, measles, scarlet fever, chicken pox, diphtheria.
True croup develops as a result of swelling of the vocal folds (cords). The only example of this pathology is diphtheria stenotic laryngitis.
Obstruction of the respiratory tract during croup develops gradually, in stages and is associated with the direct effect on the mucous membrane of infectious agents and their waste products. Its final stage is asphyxia.
The pathological mechanism of development of croup in children is based on the following processes:
- reflex spasm of the muscles that narrow the larynx (constrictors);
- swelling of the inflamed mucous membrane of the larynx;
- hypersecretion of viscous thick mucus.
Obstruction of the respiratory tract that occurs with croup in children makes it difficult to breathe, resulting in an insufficient amount of oxygen entering the lungs for normal breathing. In turn, this leads to hypoxia – oxygen starvation of all organs and tissues of the body.
The general condition of children with croup directly depends on the severity of obstruction. In the initial stages, compensation for the resulting difficulty in breathing is carried out due to more intense work of the respiratory muscles. A further decrease in the lumen of the larynx is accompanied by a compensatory breakdown and the appearance of paradoxical breathing, in which the chest expands on exhalation and narrows on inhalation. The final stage of croup in children is asphyxia, which leads to death.
Causes of false croup
The causes of false croup (acute laryngeal stenosis) can be divided into several groups.
1. The main reason is the peculiarities of the anatomical structure of the larynx in children under 8 years of age.
- the shape of the larynx is cone-shaped; - easily excitable muscular system around the larynx; - short vocal cords; - soft structure of the laryngeal walls, which can lead to their compression by neighboring muscles.
Closer to the age of eight, the structure of the larynx changes, and the likelihood of laryngostenosis becomes very low.
2. Complications of diseases such as:
- influenza, parainfluenza; - measles, chicken pox; - scarlet fever; - pertussis infection; - herpes; - laryngitis; — ARVI; - enlarged adenoids; - chlamydia; — post-vaccination manifestations; - mycoplasmosis.
3. False croup caused by bacteria.
- staphylococcus; - streptococcus; - Pneumococcus.
4. Children at risk for various reasons.
- excess weight; — birth trauma or hypoxia; - presence of rickets; - congenital anomalies of the larynx; - hereditary or individual predisposition to allergic reactions; - children who often suffer from acute respiratory infections; - children who have a reduced level of immunity due to long-term use of certain medications; — the presence of a chronic inflammatory process; - hormonal imbalances in the body.
An unexpected attack of severe coughing, stress or a loud cry can lead to a reflex narrowing of the laryngeal lumen.
Kinds
Croup in children, depending on the level of damage to the larynx, is divided into true and false. True croup develops as a result of swelling of the vocal folds (cords). The only example of this pathology is diphtheria stenotic laryngitis. With false croup in children, inflammatory swelling of the mucous membrane of the subglottic (subglottic) area of the larynx of non-diphtheria etiology is observed.
According to the etiology of the underlying disease, false croup in children is divided into the following types:
- viral;
- bacterial;
- fungal;
- chlamydial;
- mycoplasma
With timely initiation of treatment for croup in children, the prognosis is favorable, the disease ends in recovery.
According to the severity of obstruction, the following degrees of croup in children are distinguished:
- Compensated stenosis.
- Subcompensated (incomplete compensation) stenosis.
- Decompensated (uncompensated) stenosis.
- Terminal phase (asphyxia).
According to the nature of the clinical course of croup in children, it can be uncomplicated or complicated. Complicated is characterized by the addition of a secondary bacterial infection.
Diphtheria, or true croup, according to the degree of prevalence of the inflammatory process, in turn, is divided into non-extended (limited to the vocal cords) and widespread (descending) croup, in which the infectious process affects the trachea and bronchi.
Summary for parents
Croup is a life-threatening condition for a child. Diphtheria vaccinations are reliable protection against true croup. Parents should not frivolously refuse them, thereby exposing the child to the risk of developing diphtheria with its serious complications, one of which is croup.
With false croup, the situation is more complicated, since it is quite difficult to completely protect a child from viral infections. When false croup develops, parents should not panic, but be able to provide first aid. There is no need to refuse hospitalization of the child, even if the emergency doctor managed to cope with the attack at home - no one can exclude the development of false croup again. In a hospital setting, assistance will be provided on time and in full.
About the treatment of croup in children in the program “Dr. Komarovsky’s School”:
Elena Malysheva in her program also talks about false and true croup in children:
Signs of croup in children
The clinical picture of croup in children includes the following symptoms:
- Noisy breathing (stridor). It is observed in croup of any etiology. The sound accompaniment of the act of breathing is associated with the vibration of the vocal cords, arytenoid cartilages and epiglottis. As laryngeal stenosis increases, the sonority of respiratory sounds decreases, which is associated with a decrease in tidal volume.
- Dyspnea. This is a mandatory symptom of croup in children. With subcompensated stenotic laryngitis, shortness of breath is inspiratory in nature, that is, the child experiences difficulty at the moment of inhalation. The transition of the disease to the decompensated stage is characterized by the appearance of mixed inspiratory-expiratory shortness of breath (both inhalation and exhalation are difficult). Increased body temperature and rapid breathing during croup in children are accompanied by significant loss of fluid with the development of respiratory exicosis.
- Dysphonia (change in voice). The development of this symptom of croup in children is associated with inflammatory changes in the vocal cords. With true croup, hoarseness of the voice gradually increases until it completely loses its sonority (aphonia). With false croup, aphonia never occurs.
- Barking rough cough. Its occurrence is explained by incomplete opening of the glottis against the background of spasm. Moreover, the stronger the swelling, the quieter the cough.
Croup in children can be complicated by the development of sinusitis, conjunctivitis, otitis media, pneumonia, bronchitis, and meningitis.
Actions to take if you suspect croup
The main decision of any adult is to immediately contact a specialist. Before the doctor arrives, you can try to learn what to do for your baby’s croup on your own. Although it is impossible to refuse the invitation of a specialist, treatment of false croup must be carried out by a doctor .
How to treat croup
Before a professional arrives, it is recommended:
- Give the baby an antipyretic drug.
- Eliminate nasal congestion using vasoconstrictor drops or sprays (Nazivin, Vibrocil, Otrivin).
- Provide fresh and moist air. To do this, it is recommended to hang wet towels and use an air freshener. You can wrap the child in a blanket and bring it to an open window or even take it outside (in an apartment to the balcony).
- Start giving an alkaline warm drink , which uses raspberry or linden tea, Borjomi, milk to which soda is added.
- Provoking a cough will help expand the lumen of the larynx. It is performed using artificial irritation of the root of the tongue or nasopharynx with a sterile spoon.
- The removal of sputum will be facilitated by inhalation, including the use of a nebulizer.
- You can steam your child’s feet in hot water. In this case, moderately hot liquid with the addition of mustard is used. The temperature can be checked by dipping your wrist into the container.
Continuing attempts at self-treatment often ends in serious complications , which ultimately lead to long-term treatment in a hospital. Self-therapy of false croup at home can only be performed after consultation and receipt of a program of procedures and a list of medications. When croup is suspected in a child, first aid can be provided by ambulance.
Diagnostics
Diagnosis of croup in children does not cause any difficulties and is carried out by a pediatrician or otolaryngologist based on the characteristic clinical picture of the disease, medical history, physical examination and laryngoscopy. If necessary, the child is consulted by an infectious disease specialist (diphtheria croup), a phthisiatrician (larynx tuberculosis), and a pulmonologist (bronchopulmonary complications).
When auscultating the lungs in children with croup, whistling dry rales are heard. The worsening of the disease is accompanied by the appearance of moist rales of various sizes.
When performing laryngoscopy, the degree of stenosis of the larynx, the extent of the pathological process, and the presence or absence of fibrinous films are determined.
To verify the pathogen, laboratory diagnostic methods are used: bacteriological culture and microscopy of throat swabs, serological tests (RIF, ELISA, PCR). In order to determine the severity of hypoxia, the acid-base state of the blood and its gas composition are determined.
If complications are suspected, lumbar puncture, radiography of the paranasal sinuses and lungs, rhinoscopy, otoscopy, and pharyngoscopy are prescribed.
Croup in children requires differential diagnosis with the following diseases:
- laryngeal tumors;
- bronchial asthma;
- epiglotitis;
- retropharyngeal abscess;
- foreign body of the larynx;
- whooping cough;
- congenital stridor.
Differential diagnosis of diphtheria croup and croup of other etiologies:
| Sign | True diphtheria croup | False croup |
| Voice | Increasing hoarseness of voice, turning into persistent aphonia | Hoarseness is inconsistent, there is no aphonia |
| Cough | Dry, rough, barking, dull, losing sonority, up to complete aphonia | Rough, barking, without losing sonority |
| Raids | Dirty white, difficult to remove, leaving a bleeding surface after plaque removal | Superficial, easy to remove |
| Cervical lymph nodes | Enlarged, swollen on both sides, slightly painful, swelling of the tissue around the nodes | Enlarged, very painful, no swelling. Individual lymph nodes are palpated |
| Development of stenosis | Laryngeal stenosis develops gradually, initially noisy breathing, turning into an attack of suffocation. Doesn't go away on its own | Stenosis occurs suddenly, often at night. The inhalation is loud and can be heard from a distance. Sometimes stenosis resolves spontaneously |
Differential diagnosis of true and false croup in children
The first symptoms of both true and false croup in children appear 2-3 days from the onset of the underlying disease. The clinical picture of true croup in children is characterized by a gradual increase in respiratory disorders.
Children with compensated forms of croup are subject to hospitalization in the department of acute respiratory infectious diseases of an infectious diseases hospital.
During the course of the disease, several stages are clearly visible:
- Dysphonic. There is hoarseness of the voice, there are no signs of obstruction.
- Stenotic. Against the background of increasing obstruction of the larynx, the child develops breathing difficulties and signs of hypoxia appear.
- Asphyxial. Almost complete obstruction of the larynx occurs. Severe hypoxia causes the development of hypoxic coma and death.
With false croup in children, the attack occurs suddenly and mainly at night. During the day, the condition of patients changes significantly.
With true croup, the vocal cords themselves swell in children, and therefore the sonority of the voice gradually decreases until complete aphonia (silent crying, screaming). Although false croup is accompanied by hoarseness of the voice, aphonia never develops with it. When crying and screaming in children with false croup, the sonority of the voice is preserved.
With true croup in children, laryngoscopy reveals swelling and hyperemia of the laryngeal mucosa, a decrease in its lumen, and the presence of diphtheria films. Diphtheria plaques are difficult to remove, with the formation of small ulcers underneath. The observed laryngoscopic picture with false croup is different. It is characterized by:
- redness and swelling of the mucous membrane;
- accumulation of thick sputum;
- laryngeal stenosis;
- easily removed plaque.
A bacteriological examination of a throat smear allows a final differential diagnosis between false and true croup in children. When diphtheria bacilli are isolated from the test material, the diagnosis of true croup is beyond doubt.
Diagnosis of false croup
In addition to the differential diagnosis of false croup from true croup, diphtheria, described above, when making a diagnosis, it is necessary to differentiate the condition of laryngeal stenosis from an attack of bronchial asthma.
With laryngostenosis, inhalation is difficult and exhalation is inaudible; with asthma, inhalation is free, but exhalation is difficult and occurs with strain and whistling.
Also, to make a diagnosis, in addition to a thorough examination by a pediatrician and otolaryngologist, taking an anamnesis, listening to the lungs, microlaryngoscopy, culture of sputum and material from the pharynx, blood tests for PCR, and ELISA are often necessary.
Treatment of croup in children
Children with compensated forms of croup are subject to hospitalization in the department of acute respiratory infectious diseases of an infectious diseases hospital. In sub- and decompensated forms, treatment of children should be carried out in specialized emergency departments under the supervision of an otolaryngologist and resuscitator.
Prevention of true croup is based on mass vaccination of children against diphtheria in accordance with the national immunization calendar.
Treatment of croup in children is based on the following principles:
- children are placed in rooms with an air temperature of no more than 18 °C;
- for true croup, anti-diphtheria serum is prescribed intravenously or intramuscularly;
- antibiotic therapy - indicated for children with true croup or false croup complicated by a secondary bacterial infection;
- inhalation therapy - carried out only for children with a preserved cough reflex;
- prescription of a short course of glucocorticosteroids (duration 2-3 days);
- antiallergic treatment - antihistamines should be prescribed with extreme caution to children with a pronounced hypersecretory component of inflammation);
- detoxification therapy (intravenous administration of solutions of electrolytes, glucose) – aimed at reducing the severity of intoxication syndrome, correcting water and electrolyte disorders caused by respiratory exicosis;
- for a dry non-productive cough, antitussive drugs are prescribed, and for a wet cough, mucolytics are prescribed;
- prescribing antispasmodics to eliminate reflex spasm of the pharyngeal constrictor muscles;
- sedative therapy for severe agitation of the child;
- when signs of hypoxia appear, oxygen therapy is performed (inhalation of humidified oxygen through a face mask or nasal catheters, placing the child in an oxygen tent);
- If conservative treatment of croup in children accompanied by severe respiratory failure is ineffective, tracheal intubation or tracheostomy is performed.
Source: 17nov.ru
How an attack is stopped
To relieve an attack of false croup, corticosteroid hormones (usually dexamethasone) are used, which are administered intramuscularly or orally, as well as inhalations with the hormone budesonide or adrenaline. Budesonide has fewer side effects and can be used starting from six months.
Inhalation with pulmicort (budesonide) is done by a doctor or the parent himself - as a rule, in families where an attack occurred, an inhaler with a hormonal drug is already available.
In most cases, the attack goes away soon after inhalation. If the team does not have an inhaler or drug, or the inhalation turns out to be ineffective - it should be assessed after at least 15 minutes - the child may be given an injection of prednisolone or dexamethasone. It is worth considering that the effect of the injection is also not immediate.
If the attack does not go away even after the above steps, hospitalization is necessary.
After an attack, doctors recommend inhalation with pulmicort (budesonide) for the next 2-3 days. Inhalation is carried out before bedtime.
Prevention
Prevention of true croup is based on mass vaccination of children against diphtheria in accordance with the national immunization calendar.
Specific prevention of false croup has not been developed. To reduce the risk of its occurrence it is necessary:
- avoid contact of children with people who have signs of acute infectious and inflammatory diseases of the respiratory tract;
- strengthen the body's defenses (following a daily routine, proper nutrition, regular walks in the fresh air, hardening procedures);
- vaccinate against influenza, measles, mumps, and chickenpox.
Video from YouTube on the topic of the article:
Classification of croup
Stenosing laryngotracheobronichtis is divided into two forms: false and true croup. In turn, they are distinguished as follows:
| True croup | False croup |
| Catarrhal form. Main symptoms: barking cough and hoarseness of voice | Compensated stenosis: shortness of breath only during physical exertion, mild wheezing |
| Stenotic: loss of voice, noisy and difficult breathing, bluish skin in the nose area | Subcompensated stenosis: shortness of breath appears at rest, dry wheezing, tachycardia, loss of sleep |
| Asphyxial: limbs turn blue, blood pressure drops, fainting, convulsions. | Decompensated stenosis: severe shortness of breath, barking cough, tachycardia, drowsiness, dry wheezing |
| Terminal stage of stenosis: noisy and shallow breathing, bradycardia, convulsions, asphyxia |
The division of the disease into two types was made in 1826 by a French physician. Diphtheria croup became known in the time of Homer. Today, thanks to vaccines, this type is very rare. But false viral croup, which develops against the background of an infectious disease, is more common.
Treatment of the disease
Medical treatment of false croup is determined by the severity of the disease, the presence of concomitant pathologies and the risks of complications.
It includes distraction therapy, alkaline inhalations, sedatives, antihistamines and antispastic drugs, and in the case of concomitant infections, antibiotics.
In case of fourth degree laryngeal stenosis, intubation or tracheostomy is indicated. But these are extreme measures, which are very rarely reached. Drug treatment is usually sufficient.
Very often, false croup entails complications such as sinusitis, otitis media, tonsillitis, bronchitis, pneumonia, and even purulent meningitis. Therefore, in no case should you neglect preventive measures to prevent the occurrence of the disease.
With subglottic laryngotracheitis, taking antihistamines helps relieve swelling of the mucous membrane and loose tissue of the larynx
Diagnosis
The diagnosis of the disease is made by an otolaryngologist or pediatrician.
First, the doctor examines the child and performs auscultation (listening) of the lungs. In order to establish what form of the disease is present—true or false croup—laboratory tests are prescribed:
- bacterial culture of the mucous membranes of the larynx;
- blood test PCR and ELISA to exclude the presence of mycoplasma and chlamydia;
- radiography;
- examination of the larynx - microlaryngoscopy;
- inoculation on Sabouraud's medium to exclude fungal infection.
First aid
False croup in children (symptoms and treatment of pathology in relation to the stage of the disease) is characterized by a sudden attack in the evening or at night. A sick baby suddenly wakes up from horror caused by the inability to breathe and tries to cry.
You can hear a bubbling sound in the sternum, the breathing rate is disturbed, hoarseness of voice occurs, and a dry cough (resembling barking). If these attacks occur, you must immediately call the resuscitation team. Without urgent treatment, swelling of the larynx increases, and the child may suffocate.
The actions of parents before the arrival of doctors are aimed at relieving stenosis:
- It is necessary to ensure the supply of oxygen and enrich the air with water as much as possible. During the cold season, you can wrap your baby in a blanket and take him out to the open balcony. If this is not possible, you need to turn on cold water in the bathroom. You should be in the room with the child and calm him down.
- You cannot scare a minor with a hospital and doctors. Fear can intensify spasm of the larynx. It is advisable to distract your son or daughter by telling stories. The baby needs to breathe deeply. You should inhale through your nose, exhale through your throat.
- To thin the sputum, the child should be given a large amount of liquid, preferably alkaline.
- Force the minor to drink an antihistamine (Kestin, Zyrtec, Suprastin) to relieve swelling of the larynx.
- Carry out alkaline inhalation with saline solution, mineral water using a compression inhaler (nebulizer).
If a child suffers from frequent laryngitis, it is necessary to purchase ampoules of Dexamethasone, Prednisolone, Pulmicort, Berodual in advance.
In case of an attack, the first 2 drugs are administered by injection. Pulmicort, Berodual are taken orally using a compressor inhaler.
If an attack occurs, parents need to calm down and not succumb to panic. The life of a baby depends on the actions of adults. The main task of first aid is to saturate the air as much as possible with oxygen and moisture, improving the child’s breathing rate.
Drug treatment of illness in children: what drugs are used?
We found out what croup is. How to treat it? What medications are used? In order to relieve spasms of the larynx, the child can be given the painkiller “No-shpu”. Antihistamines are indicated to reduce laryngeal edema. At high temperatures, antipyretics such as Nurofen or Panadol are used. If the temperature rises above 38 degrees, Paracetamol and Ibuprofen should be given.
You should not give your child antitussive medications without a doctor’s prescription.
Since false croup is caused by a viral infection, antibiotics are not used in its treatment. The doctor prescribes antibacterial and antifungal drugs if the disease is caused by a fungal or bacterial infection.
For severe swelling of the larynx, the doctor prescribes the following medications:
- "Prednisolone."
- "Prednisone."
- "Hydrocortisone."
- "Dexamethasone."
- "Budesonide."
Antihistamines are also used (Suprastin, Diphenhydramine, Fenistil), and antitussives are also prescribed (Codeine, Thermopsis, Prenoxdiazine, Okseladin).
If possible, it is better to take antitussives in the form of syrups. Lozenges, lozenges, and aerosol preparations help relieve the condition. Sedatives are also prescribed: tincture of motherwort, valerian, medications with bromine.
True and false
So what is croup? What types are there? There are two types of this disease - true and false. Both diseases manifest themselves in the same way. But the causes of croup (true and false) differ. In both cases, swelling of the larynx develops and a characteristic cough appears.
False croup occurs as a consequence of viral respiratory diseases. Sometimes it is caused by pathogenic bacteria such as streptococcus or staphylococcus. Much less commonly, it can be caused by chlamydia or mycoplasma, as well as fungal bacteria.
The cause of true croup is a severe airborne infection, diphtheria. The causative agent of this disease is diphtheria bacillus.
Therapy at home
Treatment of croup at home consists of relieving and localizing attacks and relieving swelling in the larynx. It is necessary to exclude factors that provoke the manifestation of attacks. Provide access to fresh air and do not give the child food that may irritate the inflamed larynx. Citrus fruits, honey, and raspberry jam should not be given. Plenty of warm drinks are recommended.
The air in the room where the sick child is located should be cool and humid, not higher than +19°C. Additionally, you can use humidifiers.
It is worth giving your child warm milk with Borjomi mineral water or soda. This drink thins mucus and moisturizes the laryngeal mucosa. To do this, take one part mineral water and two parts milk. Instead of Borjomi, you can use any other alkaline water. Mineral inhalations using a nebulizer are useful.
To relieve attacks, you should do mustard foot baths. To do this, you need to dissolve mustard powder (2 tablespoons) in warm water and keep your feet in the water for 5-10 minutes. If the temperature is above 37.5°C, warming up the legs is contraindicated.
Warm compresses on the chest and larynx and cups on the back are useful. Treatment at home is possible only in cases of false croup at the initial stage and in children over 3 years of age. In other cases, the child requires hospitalization. Treatment is carried out in a hospital under the supervision of doctors. And at stages III or IV of the disease, hospitalization in the intensive care unit is provided.
Symptoms
Signs of false croup appear on the second or third day of a viral infectious disease of the upper respiratory system.
The main signs characterizing croup:
- characteristic barking/croaking cough, constantly recurring;
- shortness of breath and noisy breathing, especially in a restless state;
- hoarse voice.
During coughing attacks, the child shows severe anxiety. Secondary symptoms of croup are heavy sweating, increased breathing and pulse, increased body temperature, and possible nausea.
Due to increased respiratory failure, all signs intensify, the child’s skin on the face and body turns blue, wheezing is heard when inhaling, severe agitation is replaced by a lethargic state, and body temperature rises.
Possible complications after the disease
False croup, diagnosed at the first stage, is quickly cured and has no complications. After starting therapy at this phase of the disease, the child recovers quickly.
If the syndrome is diagnosed at the second and third stages, without proper treatment, a bacterial infection may develop. As a result, a purulent film appears on the larynx, and the infection spreads further along the respiratory tract, affecting nearby organs. May develop:
- pneumonia;
- sinusitis;
- meningitis;
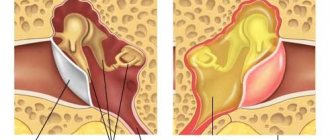
- otitis;
- acute tracheobronchitis.
Stages of croup
In medicine, there are 4 stages of false croup. They are classified according to the degree of stenosis (narrowing) of the larynx:
- Compensated stenosis. At this stage, the child’s condition is calm, breathing is slightly rapid, consciousness is clear, and slight blue discoloration around the mouth may be observed. When breathing, a visible retraction of the jugular fossa and skin on the ribs occurs. From time to time a characteristic cough appears.
- Compensated stenosis. The patient's condition worsens. Consciousness remains clear, but the child shows anxiety, especially during attacks. Breathing and pulse noticeably increase in frequency, strong skin tension in the area of the ribs, collarbones and larynx. When inhaling, a whistle appears, hoarse sounds, a croaking cough, and the voice becomes hoarse. Cyanosis appears in the nasolabial area.
- Decompensated stenosis. Breathing is shallow, pulse increases rapidly, consciousness is confused, skin turns blue. Coughing attacks become more frequent.
- Asphyxia. A very serious condition. The patient is unconscious, the skin is bluish due to lack of oxygen, the pulse is very rapid, interspersed with slowdowns. Breathing is shallow and rare. In this condition, the child may have convulsions and loss of consciousness; with severe asphyxia, death is possible.
How to help a child if false croup develops, Komarovsky
Often, parents who are caught off guard by a nighttime coughing attack in their child begin to panic, not knowing how to alleviate the baby’s condition. There are several recommendations on how to reduce the intensity of the main signs that distinguish false croup; Komarovsky advises doing this:
- ensure an influx of fresh cool air (open the windows, take the baby out onto the balcony or street);
- let steam into the bathroom and let the child breathe moist air;
- hold the baby’s legs and arms under warm water for a few minutes, allowing them to warm up;
- place mustard plasters on the soles of the feet to allow blood to flow out of the larynx and reduce swelling;
- drip any vasoconstrictor into the nose;
- Give the child a little milk with alkaline mineral water or soda.
Another important rule is that if a night attack does not lose its intensity, immediately call emergency help.