The causative agent of typhoid fever is one of the salmonellas - Salmonella typhi. This is a bacterium that is quite resistant to environmental factors: it can survive at room temperature in food (meat and dairy), water, and on household items. It quickly dies under the influence of boiling, any disinfectant solutions, or ultraviolet radiation.
There are microbes that have much in common with Salmonella typhi - these are paratyphoid pathogens Salmonella paratyphi A, B, C. The clinical picture also has many similarities, therefore in domestic practice it is customary to combine them under the term “typhoid-paratyphoid disease” .
The causative agent of typhoid fever is widespread everywhere. The highest incidence rate is observed in countries with tropical and subtropical climates (Asia and Africa). In countries of the European region, single (sporadic) cases of the disease occur.
How is typhoid fever transmitted?
The predominant route of transmission of the causative agent of typhoid fever is food; contact and water are also possible.
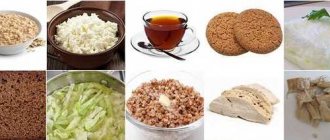
In the implementation of the food route of transmission of typhoid fever, the following products play the greatest role:
- milk and everything made from it that does not undergo heat treatment before use (ryazhenka, kefir, cottage cheese, sour cream);
- meat, offal, minced meat, jellied meat and jelly;
- vegetables and fruits that have not been thoroughly washed.
The water route of transmission is relevant in regions with a low level of sanitary culture, where mixing of water for domestic purposes and sewage waste is possible. The possibility of the typhoid pathogen entering well water and bodies of standing water cannot be ruled out.
The contact route of transmission occurs through direct contact with a patient with typhoid fever or a carrier. This can occur in families through household contacts, as well as in public catering establishments where a person (the source of infection) may work.
The greatest danger to others is not the sick person (he is receiving treatment in a hospital), but the carrier. Such a person contains and releases Salmonella typhi into the environment, but does not show any signs of illness. The pathogen is released into the environment through feces and urine; carriage can last for several days or weeks.
After suffering from the disease, stable immunity is formed throughout life. Only patients with a weakened immune system may develop repeated episodes of the disease.
Forms of the disease
Typhoid fever (Typhys abdominalis typhoid fever) is an acute infectious pathology caused by the bacterium Salmonella typhy, which affects the endothelial lining of blood vessels and lymphoid formations of the small intestine. Clinically it is characterized by a specific syndrome of general infectious intoxication, a syndrome of gastrointestinal tract damage (enteritis), roseola exanthema (rash), enlargement of the liver, spleen and intra-abdominal lymph nodes, as well as bronchitis.
Etiology
kingdom - Bacteria
family - Enterobacteriaceae
genus - Salmonella
subspecies - Enterica
serovar - Typhy
The term "Typhy" (from the Greek τῦφος) means smoke, fog.
These bacteria are gram-negative rods that do not form spores. Their structure contains from 8 to 14 flagella, are mobile, grow on simple nutrient media mixed with bile.
Their antigenic structure is very complex. It consists of:
- O-antigen (lies on the surface of the microorganism, is a lipid-polysaccharide complex, thermolabile, boiling for about two hours does not lead to destruction; is responsible for species specificity - serogroups);
- H-antigen (flagellate, thermolabile);
- Vi-antigen (included in O-antigen, thermolabile, is a virulence antigen that contributes to infection of the body);
- K-antigen (protein-polysaccharide complexes responsible for the ability of bacteria to invade macrophages and further reproduce in them).
Capable of L-transformation - partial or complete disappearance of the cell wall, as a result of which the bacterium gains the ability to tolerate unfavorable conditions for itself.
Stable in the external environment, they remain on linen for up to 80 days, in feces - up to 30 days, in toilets - up to 50 days, in tap water (without sufficient chlorination) - up to 4 months, in soil - up to 9 months, in milk - up to 3 months, in vegetables - up to 10 days. In water when heated to 50°C they live for 1 hour, when heated to 60°C - 30 minutes, in boiled water they die instantly. When frozen, they live up to 60 days; in 0.4% bleach and modern disinfectants they remain viable for up to 10 minutes.[1][2][5]
Epidemiology
Anthroponosis. Ubiquitous (widespread) infection, but mainly common in warm countries. The annual incidence of typhoid fever is more than 20 million people, of which up to 200 thousand die.
The primary source of infection is people (patients and carriers). Snails and oysters that become infected in contaminated (virus-contaminated) water sometimes become an unintentional source of typhoid bacteria.
The transmission mechanism is fecal-oral (water, food, contact and household routes).
The body's susceptibility index (its ability to respond to the introduction of a pathogen by developing a disease or carriage) is 40-50%.
Seasonality: summer-autumn (in hot countries all year round).
Immunity is type-specific, long-lasting, but a secondary disease cannot be ruled out after a long time.[2][4]
If you notice similar symptoms, consult your doctor. Do not self-medicate - it is dangerous for your health!
Based on the nature of the clinical picture, the disease is divided into:
- typically;
- atypical (erased, abortive, outpatient, also includes rare forms - pneumotyphoid, meningotyphoid, nephrotyphoid, colotyphoid, typhoid gastroenteritis).
The pathology can be acute and occur with exacerbations and periods of relapse.
The severity of the infection may be mild, moderate, or severe. Depending on the presence of complications, the disease can be uncomplicated or complicated. Complications of infection may include:
- specific (the occurrence of intestinal perforation with profuse bleeding, shock, etc.);
- nonspecific (the occurrence of pneumonia, parotitis, cholecystitis, thrombophlebitis, orchitis, etc.)
Symptoms
In the typhoid clinic, there are symptoms of a general nature and reflecting changes only in the digestive canal. Only a specialist can fully evaluate all clinical symptoms.
We recommend reading:
Probiotics and prebiotics: definition and list of drugs
Typhoid fever begins gradually - 7-10 days, and sometimes even more, pass before specific clinical manifestations appear. This time is called the prodromal period or the period of initial clinical manifestations. At this time the patient notes:
- increasing weakness, which makes it difficult to live a normal life;
- headache, which is practically not relieved by conventional analgesics, has a bursting, aching character without clear localization;
- insomnia (difficulty falling asleep, waking up early);
- temperature rise often to low-grade levels (37-37.5°C).
After this, a period of clinical manifestations begins. Specific clinical signs force the patient to seek medical help, and the doctor is helped to correctly make a preliminary diagnosis.
Among the symptoms of the height of the period, the most significant are:
- persistent fever, lethargy and constant drowsiness;
- pale skin and isolated roseate rashes on the skin of the abdomen;
- loose stools without pathological impurities (blood, mucus, pus), which is replaced by constipation;
- dyspeptic signs (deterioration of appetite up to its complete absence, nausea, vomiting, diffuse abdominal pain of moderate intensity);
- Some patients have a cough, pain in the heart and chest.
During an objective examination, some specific symptoms are noted, but they are understandable only to a specialist.
Signs of improvement in the condition of a typhoid patient are:
- decrease in temperature (gradual, over several days);
- disappearance of insomnia;
- improvement in general condition (decreased weakness, feeling of increased strength);
- normalization of appetite;
- normalization of stool (frequency of appearance and consistency).
An atypical course of typhoid fever may be observed - an acute violent onset and rapidly increasing clinical symptoms. The patient may also be bothered by symptoms from the respiratory system: nasal congestion, cough with sputum.
Possible complications
Specific complications of typhoid fever are:
- intestinal bleeding;
- perforation of the intestinal wall;
- typhoid peritonitis;
- formation of secondary metastatic foci;
- Zenker muscle necrosis;
- bone marrow damage;
- damage to the heart sac (endocarditis, myocarditis).
Only a specialist can diagnose complications of typhoid fever. Intestinal bleeding and perforation of the intestinal wall are very serious processes that can lead to the death of the patient, especially if the diagnosis was made late.
The formation of secondary lesions - in the brain, lungs, kidneys - is not so dangerous for the patient’s health, but it delays the recovery process. The formation of a new focus of typhoid bacillus can provoke a new deterioration in the patient’s condition.
We recommend reading:
Methods of rehydrating the body for dehydration: oral and parenteral agents
Zenker's necrosis is a rare but serious complication. The muscle tissue of the legs, less often the arms, undergoes decay without rotting. The limb permanently loses its functional abilities.
Damage to the bone marrow under the influence of typhoid toxin is manifested by a decrease in the number of white and red blood cells. A significant change in the cellular composition of the blood leads to serious disorders of all types of metabolism.
Danger of acute infection for humans
Although paratyphoid fever causes fewer complications, they are possible in severe cases of the disease. The consequences of infection are associated with damage to the nervous system in the form of depression, and less commonly, violent delirium.
Since the intestines are affected during salmonella infection, minor bleeding is possible, and there are rare cases of perforation of the walls of the colon. Paratyphoid B and its septic forms cause complications when metastases of purulent foci appear in the joints, cartilage, periosteum, urinary tract, muscles, and sometimes appear in the brain area. Such forms of the disease are acute, or develop into blood poisoning, pyaemia, which lasts for years.
Complications of paratyphoid fever include:
- jaundice;
- hemorrhagic colitis;
- mental damage;
- cardiac dysfunction;
- meningitis.
Septic forms of complications are dangerous due to their duration. And although they end in complete recovery, cholecystitis, abscesses of the kidneys, and spleen can develop against their background. Serious danger can only be avoided through timely diagnosis and treatment of the disease.
Diagnostics
The diagnosis and treatment of typhoid-paratyphoid diseases is carried out by an infectious disease specialist. It is usually recommended to carry out specific therapy in a hospital setting.
The examination includes specific and nonspecific research methods. The materials for analysis are blood, urine and feces.
Nonspecific research methods (general and biochemical blood tests) help the doctor assess the patient’s condition and also suspect complications.
Specific methods make it possible to identify the pathogen in the human body and confirm the diagnosis of typhoid fever or paratyphoid fever.
The test for typhoid fever is taken for the first time before treatment begins, that is, before the patient begins to receive antibiotics. Blood, urine and feces are donated for testing. After completing a course of antibiotic therapy, the patient again donates the same biological fluids to monitor the effectiveness of therapy.
Mandatory tests for typhoid fever include:
- bacteriological blood test (hemoculture) – if Salmonella typhi is detected, then this is a 100% confirmation of the diagnosis;
- bacteriological examination of stool (coproculture) - can confirm the diagnosis of typhoid fever or carrier state;
- bacteriological examination of urine (urine culture) - can confirm the diagnosis of typhoid fever or carrier state;
- serological reactions (RPGA or Widal reaction, as well as reaction with virulence antigen).
Only a doctor can evaluate the results of laboratory tests.
Since patients with typhoid infection who work in catering establishments, schools and kindergartens pose a particular danger to others, this group of people must be examined.
For the study, human blood is taken, bacteriological culture is performed and a pure culture is isolated. After 4 days, a positive or negative result is obtained, which is entered in the health book.
We recommend reading:
Enterobacteriaceae in a child’s stool: is it dangerous and how to treat it?
General principles of treatment
Typhoid fever can be cured only if all medical prescriptions are followed. Trying to take medications on your own can only cause harm and cause complications. With uncomplicated typhoid fever, the prognosis is favorable.
Antibiotic ineffectiveness may be a problem, especially if the patient comes from Southeast Asian countries. If there is no result from using first-line drugs (chloramphenicol succinate), the patient should be prescribed reserve antibiotics.
Complex therapy of typhoid fever includes:
- bed rest for the entire period of elevated temperature;
- diet (treatment table No. 1);
- antibiotics;
- infusion solutions to reduce intoxication;
- enzyme agents to improve digestion processes;
- immunomodulators.
It is better to reduce the temperature during typhoid fever not with medications, but with physical methods (rubbing with alcohol, applying cold to the main vessels).
Treatment of typhoid fever is long-term; complete recovery may take 1-2 months.
Monitoring of contact persons, that is, those who directly interacted with a typhoid patient, continues for at least 25 days. In addition, a bacteriological examination of the feces and blood of such people is carried out.
How is the disease treated?
A favorable outcome of paratyphoid infection is associated with proper patient care, diet, and timely administration of medications.
It is important to adhere to bed rest, especially the first week after body temperature has stabilized. Only after seven to eight days of normal body temperature are they allowed to sit, and after three days - to walk.
The patient should be at rest in a comfortable bed. Much attention is paid to hygiene of the oral cavity and body skin.
Nutrition is organized as gentle as possible in relation to the intestines. Food products should not cause the development of fermentation and putrefactive processes, but sufficient caloric content should not be forgotten.
The patient's diet must include steamed meat dishes, pureed soups, dairy products, vegetable and fruit juices. Vegetables with coarse fiber, such as cabbage and radish, are excluded from the diet. It is harmful to eat fatty fish, meat, sausages, and canned food.
In severe cases of the disease, they are fed only liquid food - mucous decoctions of cereals, rosehip tea, weak meat broth. The presence of diarrhea leads to the exclusion of dairy products from the diet. After stabilization of the patient's condition, solid food is gradually included.
The following medications are prescribed:
- chloramphenicol;
- ampicillin;
- biseptol;
- nitrofuran and its analogues;
- glucose or Ringer's solution to detoxify the body;
- in severe cases - corticosteroids.
The occurrence of complications requires specific therapy, sometimes urgent surgery. Only a doctor knows how paratyphoid fevers of different groups are treated, so self-medication is unacceptable and will lead to serious consequences.
General principles of prevention
The vaccines developed for the prevention of typhoid fever do not provide 100% protection; immunity is short-lived and weak. The main way to protect yourself is to comply with sanitary and hygienic rules.
To prevent typhoid fever and paratyphoid fever, you should:
- wash your hands thoroughly;
- follow the rules for preparing and storing food;
- drink only boiled water;
- At the first sign of discomfort, contact a specialist.
Typhoid fever is a serious disease, but quite manageable if you seek medical help in a timely manner.
In continuation of the topic, be sure to read:
- The most common infectious bowel diseases
- Details about salmonellosis: pathogen, transmission routes, signs and treatment
- The causative agent of shigellosis, its symptoms and treatment
- How is rotavirus intestinal infection manifested and treated?
- Intestinal flu: symptoms and treatment in adults
- Intestinal infection: symptoms and treatment methods (diet, medications)
- Intestinal tuberculosis: first signs, diagnosis and treatment
- Botulism: how does the disease manifest itself and what contributes to infection?
- Dysentery: how is the disease manifested and treated?
- Norovirus: how is the infection transmitted, manifested and treated?
Pathogen carrier
Recently cured patients are considered to be carriers of the bacilli. After recovery, a person remains infectious to others for a long time.
Vaccinated people are also carriers of the harmful microorganism.
In rare cases, the disease is hidden. The patient does not have severe symptoms. Treatment is carried out at home, without going to doctors and aggravating the general condition. As a result, family members and other people get sick. Most often, infection occurs through food and common household items.