In this article you will learn: what is pulmonary hypertension. The causes of the development of the disease, types of increased pressure in the vessels of the lung, and how the pathology manifests itself. Features of diagnosis, treatment and prognosis.
Author of the article: Yachnaya Alina, oncologist surgeon, higher medical education with a degree in General Medicine.
Article publication date: 07/01/2017
Article updated date: 05/29/2019
Pulmonary hypertension is a pathological condition in which there is a gradual increase in pressure in the pulmonary vascular system, which leads to increasing insufficiency of the right ventricle and ultimately ends in the premature death of a person.
| Normal mean pulmonary artery pressure (mmHg) | Mean pressure for pulmonary hypertension (mm Hg) |
| 17–23 | More than 25 – at rest More than 30 – under load |
When the disease occurs in the circulatory system of the lungs, the following pathological changes occur:
- Narrowing or spasm of blood vessels (vasoconstriction).
- Reduced ability of the vascular wall to stretch (elasticity).
- Formation of small blood clots.
- Proliferation of smooth muscle cells.
- Closure of the lumen of blood vessels due to blood clots and thickened walls (obliteration).
- Destruction of vascular structures and their replacement with connective tissue (reduction).
In order for blood to pass through the changed vessels, the pressure in the trunk of the pulmonary artery increases. This leads to increased pressure in the cavity of the right ventricle and leads to disruption of its function.
Such changes in blood flow manifest themselves as increasing respiratory failure in the early stages and severe heart failure in the final stages of the disease. From the very beginning, the inability to breathe normally imposes significant restrictions on the patients’ daily life, forcing them to limit themselves in exercise. The decrease in resistance to physical labor worsens as the disease progresses.
Pulmonary hypertension is considered a very serious disease - without treatment, patients live less than 2 years, and most of this time they require help with personal care (cooking, cleaning the room, shopping for groceries, etc.). With therapy, the prognosis improves somewhat, but the disease cannot be completely cured.
Click on photo to enlarge
The problem of diagnosing, treating and monitoring people with pulmonary hypertension is dealt with by doctors of many specialties, depending on the cause of the disease, these can be: therapists, pulmonologists, cardiologists, infectious disease specialists and geneticists. If surgical correction is necessary, vascular and thoracic surgeons are involved.
Causes and forms of pathology
Pulmonary arterial hypertension - what is it? This is the name for a disease caused by pathological changes in the pulmonary system, in which there is a sharp increase in intravascular pressure above 35 mm Hg. Art.
Primary pulmonary hypertension is an incompletely studied form of the disease. The reason for the development of the idiopathic form of the pathology is genetic disorders of the vessels of the pulmonary system. The body produces small amounts of substances that are responsible for the dilation and constriction of blood vessels. Primary hypertension can be caused by excessive platelet activity, which leads to blockage of blood vessels.
Secondary pulmonary hypertension develops as a result of various chronic diseases - congenital heart disease, thrombotic lesions of the arteries in the lungs, Pickwick syndrome, cardiac and pulmonary diseases, bronchial asthma.
Chronic thromboembolic pulmonary hypertension is caused by blockage of blood vessels. The disease is characterized by rapid progression, acute respiratory failure, decreased blood pressure, and hypoxia.
Factors contributing to the development of the disease:
- taking amphetamine, cocaine, antidepressants and appetite suppressants;
- pregnancy, hypertension, HIV, pathological changes in the liver;
- oncological diseases of the hematopoietic system;
- increased pressure in the collar area;
- hyperthyroidism;
- frequent climbs to the mountains;
- compression of blood vessels in the lungs by a tumor, deformed sternum or due to obesity.
Important! Studies by foreign scientists have proven that primary pulmonary hypertension is caused by certain antibiotics and hormonal oral contraceptives. Pathology often develops in smokers.
Treatment
The goal of treatment is to control the course of the underlying pathology and prevent possible consequences. Treatment of pulmonary hypertension is carried out in a hospital.
Supportive and restorative therapy is provided. Limiting physical activity and preventing infectious diseases is mandatory. It is recommended to prescribe diet No. 10. Severe and acute pulmonary hypertension cannot be treated at home. The main thing is to prevent progression of the disease and maintain a low functional class.
For treatment use:
- Oxygen therapy (oxygen breathing) – is carried out with increasing hypoxia, when the partial pressure of oxygen is lower than 55-60 mm Hg. Art.
- Anticoagulants are used to reduce the risk of thrombosis. For these purposes, Warfarin is often prescribed. This is an indirect anticoagulant that prevents the formation of blood clots. Antiplatelet agents are prescribed for the same purpose.
- Diuretics - to reduce the load on the right side of the heart. Diuretics help reduce venous blood pooling in the systemic circulation and reduce right ventricular volume overload, relieving shortness of breath and reducing edema.
- Calcium channel blockers are one of the most effective treatments for PH. Most often among representatives of this group of drugs they resort to the use of Nifedipine or Diltiazem. Half of the patients, after long-term use of these drugs, experienced a decrease in symptoms and overall health improved. In this case, it is important to monitor the average level of blood pressure for further correction of treatment. Treatment begins with small doses, then they are gradually increased.
- Endothelin receptor antagonists help block the action of endothelin, which causes pulmonary vasoconstriction.
- Prostaglandins dilate narrowed pulmonary vessels, prevent platelet aggregation and the subsequent development of thrombosis in PH.
- PDE-5 inhibitors affect the blood vessels of the lungs. A representative of this group, Sildenafil, dilates the blood vessels of the lungs and inhibits the growth of smooth muscle cells. It is effective in the treatment of PH caused by rheumatic diseases and congenital heart disease, and in idiopathic PH.
- Guanylate cyclase stimulators have a vasodilator and antiplatelet effect, due to which they are used for the treatment of chronic thromboembolic PH and pulmonary arterial hypertension.
- Cardiac glycosides help improve myocardial contractility.
Prescriptions are carried out purely individually, depending on the characteristics of the course of the disease, the state of the body and the patient’s tolerance of certain drugs.
To select the appropriate drug, an acute vasoreactivity test is performed. What it is? This is a study that shows an assessment of the severity of PH, hemodynamic disturbances, if any, and helps to predict the effectiveness of the therapy.
How does the disease manifest itself?
Moderate pulmonary hypertension develops slowly; at the initial stage, the symptoms of the disease are not pronounced. The main clinical sign of the disease is cor pulmonale. The pathology is characterized by hypertrophic changes in the right parts of the heart.
What signs should you see a doctor for:
- The main manifestation of the disease is shortness of breath, which worsens even with minor physical exertion.
- Cardiopalmus. The cause of tachycardia is respiratory failure, lack of oxygen in the blood.
- Pain syndrome. Compressive pain occurs behind the sternum and in the region of the heart. With strong physical exertion, fainting is possible.
- Dizziness, weakness, fatigue.
- Accumulation of fluid in the peritoneum (ascites), severe swelling and blueness of the limbs, bulging veins in the neck. These symptoms develop against the background of chronic right ventricular failure - the heart muscle of the right ventricle cannot cope with the load, which leads to disturbances in the systemic circulation.
- An enlarged liver leads to heaviness and pain under the right ribs.
- Nausea, flatulence, vomiting are caused by accumulation of gases in the intestines. Weight loss with normal, nutritious nutrition.
The fingers thicken in the upper phalanges, the nails become like watch glass. As the pathology develops, sputum mixed with blood appears, which signals the onset of pulmonary edema. The patient suffers from attacks of angina pectoris and arrhythmia. At the terminal stage of the disease, active tissue begins to die.
Important! Pulmonary hypertension is a hereditary disease caused by a genomic defect.
Classification
There are several classifications of pulmonary hypertension: pathophysiological and clinical.
Pathophysiological classification
According to the pathophysiological features, hypertension of the pulmonary circulation is:
- precapillary (this includes PH of lung diseases);
- postcapillary (this includes PH in diseases of the left heart).
Full clinical classification
According to clinical data, 5 main groups are distinguished.
- Pulmonary arterial hypertension:
- idiopathic PH;
- hereditary pulmonary hypertension;
- caused by toxins and medications;
- combined with the following diseases: connective tissue diseases, portable hypertension, HIV, schistosomiasis, congenital heart defects (CHD), chronic hemolytic anemia.
- persistent pulmonary hypertension in newborns;
- veno-occlusive pulmonary disease and/or pulmonary capillary hemangiomatosis.
- Hypertension of the pulmonary circulation as a consequence of diseases of the left heart:
- diastolic dysfunction;
- systolic dysfunction;
- valve disease.
- PH as a consequence of hypoxia and/or lung pathology:
- chronic obstructive pulmonary diseases;
- diffuse diseases of the interstitial tissue of the lungs;
- lung diseases, which are accompanied by changes in the lumen of the bronchi;
- breathing disorders during sleep;
- disturbance of gas exchange in the alveoli;
- chronic exposure to high altitude;
- lung malformations.
- Chronic thromboembolic PH:
- PH with unclear and/or multifactorial mechanisms:
- hemolytic diseases: myeloproliferative diseases, removal of the spleen;
- systemic pathologies: sarcoidosis, pulmonary histiocytosis, lymphangioleiomyomatosis, neurofibromatosis;
- metabolic disorders: Gaucher disease, thyroid disorders, glycogen storage disease;
- other diseases: mediastinitis with the process of fibrin deposition in the mediastinum, obstruction caused by a tumor, chronic renal failure, segmental pulmonary hypertension.
Functional classification of PH
PH is divided into 4 classes:
| DESCRIPTION | CLASS |
| Patients have no restrictions on physical activity. Ordinary stress on the body does not lead to weakness, dizziness, shortness of breath, or chest pain. | I |
| There is a slight limitation in physical activity. In the absence of stress, symptoms do not appear. Normal stress leads to shortness of breath, dizziness, weakness, and chest pain. | II |
| Marked limitation of physical activity. At rest there are no symptoms. Minor physical activity leads to weakness, shortness of breath, dizziness, and chest pain. | III |
| Inability to withstand physical activity without symptoms. At rest, the patient feels chest pain, shortness of breath, dizziness, and weakness. Symptoms appear at the slightest physical exertion. | IV |
Degrees of the disease
Depending on the degree of development of the pulmonary heart and hypoxia, 3 degrees of pathology are distinguished.
Pulmonary hypertension stage 1. In the transient form there are no clinical or radiological manifestations. At this stage, primary symptoms of respiratory failure may appear.
Pulmonary hypertension 2 degrees. With a stable stage of the disease, shortness of breath begins to develop and cor pulmonale begins to form. When listening, you can hear the initial manifestations of increased pressure in the pulmonary artery.
At the third stage, the liver becomes enlarged, swelling appears, the skin changes color, and the veins in the neck begin to swell greatly.
Classification of the disease
Based on severity, there are 4 stages of PH:
The first stage is not accompanied by loss of muscle activity. Hypertensive patients maintain the usual rhythm of life without feeling dizzy, fainting, weakness, painful sensations in the sternum, or severe shortness of breath. At the next stage, the patient's physical capabilities are limited. The calm state does not cause any complaints, but with a standard load, shortness of breath, loss of strength, and loss of coordination appear. At the third stage of the development of the disease, all of these symptoms appear in hypertensive patients even with little activity. The last stage is characterized by severe symptoms of shortness of breath, pain, and weakness even in a calm state.
Diagnostics
Signs of pulmonary hypertension are often not very specific, therefore, based only on complaints and external examination, it is difficult to correctly establish the main cause of the disease. Only with the help of a thorough diagnosis can you see all the pathologies and malfunctions in the body. A consultation with a pulmonologist and cardiologist is necessary.
How is the diagnosis performed:
- Collecting an anamnesis - determining, from the patient’s words, the time of deterioration of the condition, how the disease manifests itself, what may be associated with the appearance of unpleasant symptoms.
- Lifestyle analysis – presence of bad habits, hereditary diseases, working conditions.
- Visual inspection - blue discoloration of the skin, changes in the shape of the fingers and the condition of the nails. The doctor notes whether there is swelling or changes in the size of the liver. Be sure to carefully listen to the lungs and heart with a phonendoscope.
- ECG - it is used to determine changes in the size of the right chambers of the heart.
- An X-ray of the chest area shows an increase in the size of the heart.
- Catheterization (pressure measurement) of the artery.
The most informative type of diagnosis is echocardiography. Signs of pulmonary hypertension on cardiac ultrasound appear in the form of right ventricular hypertrophy. Indicators less than 4 mm indicate the absence of pathology. If the thickness of the ventricular walls exceeds 10 mm, this indicates the development of pulmonary hypertension.
Diagnosis of pulmonary hypertension
Most often, hypertensive patients come for consultation with complaints of constant shortness of breath, which complicates their usual life. Since primary PH does not have any special signs that make it possible to diagnose PH during the initial examination, the examination is carried out comprehensively - with the participation of a pulmonologist, cardiologist and therapist.
Methods for diagnosing PH:
Primary medical examination with recording of anamnesis . Pulmonary hypertension is also due to a hereditary predisposition, so it is important to collect all the information about the family history of the disease. Analysis of the patient's lifestyle . Bad habits, lack of physical activity, taking certain medications - everything plays a role in establishing the causes of shortness of breath. A physical examination allows you to assess the condition of the neck veins, skin tone (cyanotic in case of hypertension), liver size (in this case, enlarged), the presence of swelling and thickening of the fingers. An ECG is performed to detect changes in the right side of the heart. Echocardiography helps determine the speed of blood flow and changes in the arteries. A CT scan using layer-by-layer images will allow you to see the expansion of the pulmonary artery and concomitant diseases of the heart and lungs. Catheterization is used to accurately measure pressure in blood vessels. A special catheter is passed through a puncture in the thigh to the heart, and then to the pulmonary artery. This method is not only the most informative, it is characterized by the minimum number of side effects. Testing “6 min. walking" shows the patient's response to additional stress to establish the class of hypertension. Blood test (biochemical and general). Pulmonary angiography by injecting contrast markers into the vessels allows you to see their exact pattern in the area of the pulmonary artery. The technique requires great caution, since manipulations can provoke a hypertensive crisis.
To avoid mistakes, PH is diagnosed only as a result of studying data from a comprehensive vascular diagnostics. Reasons for visiting the clinic may be:
The appearance of shortness of breath with habitual exertion. Pain in the sternum of unknown origin. Constant feeling of persistent fatigue. Increasing swelling of the lower extremities.
Conservative treatment methods
After a thorough diagnosis, drug treatment should be started immediately. The goal of therapy is to eliminate or correct the main manifestations of the disease and prevent the development of concomitant diseases.
Drugs of choice for pulmonary hypertension:
- Calcium channel blockers – Prazosin, Nifedipine. These medications are prescribed at an early stage of the disease. Verapamil is not recommended for the treatment of hypertension, since the therapeutic effect of the drug is rather weak.
- Drugs that thin the blood - Aspirin, Cardiomagnyl.
- Diuretic medications - Lasix, Furosemide.
- Digoxin is a cardiac glycoside. The drug is indicated for atrial fibrillation to normalize the heart rhythm.
- Anticoagulants – Warfarin, Heparin. Medicines are used to prevent blood clots.
- Prostaglandins and their analogues - Treprostinil, Epoprostenol. Medicines to normalize pressure in the pulmonary artery.
- Bosentan – slows the development of pulmonary hypertension.
- Medicines that improve metabolic processes in cells - Riboxin, Potassium Orotate.
For several years, scientists have been conducting research on the effectiveness of using Sildenafil in the complex therapy of pulmonary hypertension. Sildenafil citrate is the main component of Viagra and is designed to eliminate erectile dysfunction.
The drug was used on patients for 12 weeks. In control groups that received 20–80 mg of the drug, the scores improved significantly.
Prevention
To prevent pulmonary hypertension, smoking cessation is important. If possible, possible risk factors should be excluded. It is important to treat any diseases that can lead to pulmonary hypertension in a timely, correct and complete manner.
When a pathology is diagnosed, prevention is necessary to reduce the risk of complications. It is important not only proper drug treatment, but also lifestyle. The patient needs physical activity: it should be regular, but moderate. Any psycho-emotional stress should be avoided.
Watch a video about the causes, signs and treatment methods of pulmonary hypertension:
Pulmonary hypertension is dangerous due to its complications and long-term course without pronounced symptoms. Pathology can be diagnosed using an integrated approach. In most cases, conservative treatment is sufficient, but sometimes surgery is required.
How to treat in adults
If the patient's hemoglobin level exceeds 170 g/l, the neck veins bulge - bloodletting is performed. Oxygen inhalations, which must be done in courses, give positive results.
The progression of the disease can be reduced through surgery. They use the bypass method - they create an artificial oval window between the atria, which reduces high pulmonary hypertension. This allows the patient to live longer, and the prognosis for the course of the disease improves significantly.
Organ transplantation is also used - to eliminate the pathology, it is enough to transplant 1 lung. But after 5 years, many patients begin to experience rejection.
Important! In later stages of disease, a heart and lung transplant is possible. It is not advisable to carry out such an operation at the beginning of the development of pathology.
Potential Complications
Among the negative consequences it should be noted:
Heart failure. The right half of the heart does not compensate for the resulting load, this aggravates the patient’s situation. PE – pulmonary artery thrombosis, when the vessels are blocked by blood clots. This is not just a critical condition - there is a real threat to life. A hypertensive crisis and a complication in the form of pulmonary edema significantly reduces the patient’s quality of life and often leads to death. PH provokes acute and chronic forms of heart and lung failure, which threaten the life of hypertensive patients.
Pulmonary hypertension in children
This pathology indicates the inability to adapt to blood circulation in the lungs outside the womb and occurs in 0.1–0.2% of newborns. Most often, the disease is diagnosed in children who were born by caesarean section. The disease is detected in the first 3 days after birth.
Against the background of hypertension, the pressure in the vessels of the lungs begins to rise sharply, and the heart experiences increased stress. To avoid heart failure, the body begins to reduce pressure in the lungs - reducing the volume of circulating blood, dumping it into the foramen ovale in the heart or into an open arterial stream. Such actions lead to an increase in venous blood and a decrease in oxygen content.
Reasons for the development of pathology:
- suffered prenatal stress - hypoxia and glycemia can cause a spasm in the pulmonary artery in a newborn, as well as sclerotic changes in the walls of the vessel;
- delayed maturation of vascular walls - spasms often occur in such vessels;
- the presence of a congenital diaphragmatic hernia - with this disease, the lungs and blood vessels remain underdeveloped and cannot function fully;
- premature closure of the fetal ductus arteriosus, which leads to increased pulmonary blood flow;
- congenital cardiac and pulmonary malformations.
Hypertension in a newborn can occur against the background of intrauterine infection or sepsis. The cause may be polycythemia, an oncological disease in which the number of red blood cells sharply increases.
Important! Some medications that a woman took during pregnancy - antibiotics, aspirin - can cause pathology in a child.
A newborn with pulmonary hypertension has heavy breathing, shortness of breath begins, while inhaling, the chest collapses inward, the skin and mucous membranes turn blue. Without timely qualified assistance, 4 out of 5 babies with pathologies die within the first three days after birth.
Treatment of PH
In the first stages, the disease responds to the proposed therapy. Key guidelines when choosing a treatment regimen should be:
Identifying and eliminating the cause of the patient’s poor health; Reduced pressure in the blood vessels of the lungs; Prevention of blood clots in the arteries.
Recommendations may include medications:
Drugs that relax vascular muscles are especially effective in the early stages of PH. If treatment is started before irreversible processes occur in the vessels, the prognosis will be favorable. Blood thinning medications. If the blood viscosity is strong, the doctor may prescribe bloodletting. Hemoglobin in such patients should be at a level of up to 170 g/l. Oxygen inhalations, which relieve symptoms, are prescribed for severe shortness of breath. Recommendations for eating low-salt foods and water intake up to 1.5 l/day. Control of physical activity - loads that do not cause discomfort are allowed. Diuretics are prescribed when PH is complicated by pathology of the right ventricle. When the disease is advanced, drastic measures are resorted to - lung and heart transplantation. The method of such an operation for pulmonary hypertension is only being mastered in practice, but transplantation statistics convince us of their effectiveness. The only drug in Russia for the treatment of PH is Tracleer, which reduces pressure in the pulmonary arteries by inhibiting the activity of indothelin-1, a powerful vasoactive substance that provokes vasoconstriction. Oxygen saturation in the lungs is restored, the threat of a sharp oxygen deficiency with loss of consciousness disappears.
Pathology during pregnancy
Important! Pulmonary hypertension is diagnosed in women of childbearing age almost 2 times more often than in men.
The cause of the development of the disease during pregnancy may be a heart defect or a genetic predisposition to hypertension.
The first signs of the disease in pregnant women:
- the appearance of shortness of breath even at rest;
- cough of non-productive origin;
- weakness and fatigue;
- frequent respiratory diseases.
In the second and third trimester, pain appears in the area of the heart and sternum, moist rales in the lungs, and swelling. In the absence of necessary therapy, spontaneous termination of pregnancy is possible.
Women who have pulmonary vascular pathologies are advised to avoid pregnancy. If pregnancy is interrupted, the risk of death is 7%. If a woman does not want to terminate her pregnancy, she will have to spend the entire time until the baby is born in a hospital. The hospital will provide oxygen therapy to prevent blood clots.
The mortality rate among women giving birth is very high (reaches 40%), regardless of the therapy performed during pregnancy. Most deaths occur directly during delivery or in the first week after birth.
Signs of PH
The first clinical symptoms of PH appear only after the pressure in the pulmonary vessels has doubled. The key sign of the disease is shortness of breath, with its own characteristics that make it possible to distinguish it from signs of other diseases:
Manifests itself even in a calm state; With any load, the intensity increases; In a sitting position, the attack does not stop (if compared with cardiac dyspnea).
The remaining symptoms of PH are also common to most patients:
Fatigue and weakness; Fainting and heart rhythm disturbances; Endless dry cough; Swelling of the legs; Painful sensations in the liver associated with its growth; Chest pain from dilated artery; Hoarse notes in the voice associated with pinched laryngeal nerve.
As you can see, the signs of PH are not so specific that an accurate diagnosis can be made without a comprehensive examination.
Traditional methods of treatment
Even traditional medicine cannot completely eliminate pulmonary hypertension. Therapy will be effective only if the cause of the disease can be eliminated. Treatment with folk remedies is aimed at reducing symptoms.
- Brew 225 ml of boiling water and 5 g of ripe rowan, leave for an hour. Take 110 ml three times a day. Duration of therapy is 1 month.
- You can get rid of arrhythmia with fresh pumpkin juice. You need to drink 100 ml of the drink per day.
- Also, for treatment and prevention, you need to eat 4 juniper berries daily. You can also make an infusion from them. Pour 25 g of fruit into a thermos, pour 260 ml of boiling water, leave overnight. Divide the medicine into 4 servings, drink 1 day before.
- Adonis helps eliminate the main manifestations of the disease and relieves pulmonary edema. Brew 220 ml of boiling water, 3 g of raw materials, leave for 2 hours. Take 30 ml before meals.
Garlic
Peel and chop 2 fresh heads of garlic, place the mixture in a glass container, pour in 230 ml of vodka. Infuse for 15 days in a dark, cool room. Take the tincture 5 times a day. A single dose is 20 drops - the medicine must be diluted in 15 ml of warm water or milk. The duration of therapy is 21 days.
If you are intolerant to alcohol, make a medicine from 3 large heads of garlic and 3 crushed lemons. Pour the mixture into 1 liter of boiling water, close the container, and leave for a day. Take 3 times a day, 15 ml.
Herbs
An alcohol tincture is prepared from calendula inflorescences. Pour 160 ml of vodka into 60 g of raw material and leave for a week. Take 25 drops three times a day for 3 months.
Here are more recipes:
- Grind 22 g of dried birch leaves, pour 420 ml of boiling water, put in a cool, dark room for 2 hours. Take 105 ml four times a day. The duration of treatment is 15 days.
- Brew 245 ml of boiling water and 6 g of toadflax herb, leave for an hour in a closed container. Take 35 ml 36 times a day.
- Grind the corn silk into powder. Add 100 ml of fresh honey to 50 g of powder, take 5 g of medicine before meals 3-5 times a day.
Important! Non-traditional methods of treatment must be used only in combination with medications.
Why does PH develop?
The reasons for the development of PH have not yet been fully determined. For example, in the 60s in Europe there was an increase in the number of cases associated with excessive use of contraceptives and weight loss products. Spain, 1981: complications in the form of muscle damage that began after the popularization of rapeseed oil. Almost 2.5% of the 20,000 cases were diagnosed with pulmonary arterial hypertension. The root of the evil turned out to be tryptophan (an amino acid) present in the oil; this was scientifically proven much later.
Impaired function (dysfunction) of the pulmonary vascular endothelium: the cause may be a hereditary predisposition or the influence of external damaging factors. In any case, the normal balance of nitric oxide metabolism changes, vascular tone changes towards spasm, then inflammation, the endothelium begins to grow and the lumen of the arteries decreases.
Increased endothelin content (vasoconstrictor substance): caused either by an increase in its production in the endothelium, or by a decrease in the breakdown of this substance in the lungs. It is noted in the idiopathic form of PH, congenital heart defects in children, and systemic diseases.
Impaired synthesis or availability of nitric oxide (NO), decreased production of prostacyclin, additional excretion of potassium ions - all deviations from the norm lead to arterial spasm, proliferation of the muscular wall of blood vessels and endothelium. In any case, the final development is a violation of blood flow in the pulmonary artery system.
Nutrition rules
A diet for pulmonary hypertension involves limiting the diet of salt and animal fats. It is also necessary to reduce the amount of fluid consumed. The basis of nutrition should be plant foods, animal products should contain a minimum amount of fat.
Lifestyle:
- preventing exacerbation of autoimmune diseases - timely vaccination against influenza, rubella, and other infectious diseases;
- dosed physical activity - at the initial stages of the disease, special physical therapy is prescribed, at the last stage, physical activity is minimized or completely limited;
- protection from pregnancy - increased stress on the heart with pulmonary hypertension can lead to death;
- consultations with a psychologist to restore neuropsychic balance - patients with hypertension often experience depressive states and suicidal thoughts.
To prevent the development of the disease, you need to eliminate all bad habits. With regular physical activity, blood circulation improves, which prevents the formation of blood clots. The diet should be complete and balanced.
Diagnosis of pulmonary hypertension
Diagnosis of precapillary PH (associated with COPD, arterial pulmonary hypertension, chronic thrombosis:
Pulmonary artery pressure: average ≥ 25 mm Hg at rest, more than 30 mm Hg during exertion; Increased pulmonary artery wedge pressure, blood pressure inside the left atrium, end-diastolic ≥15 mm, pulmonary vascular resistance ≥ 3 units. Wood.
Postcapillary PH (for diseases of the left half of the heart):
Pulmonary artery pressure: average ≥25 (mm Hg) Initial: >15 mm Difference ≥12 mm (passive PH) or >12 mm (reactive).
ECG: overload on the right: enlargement of the ventricle, expansion and thickening of the atrium. Extrasystole (extraordinary contractions of the heart), fibrillation (chaotic contraction of muscle fibers) of both atria.
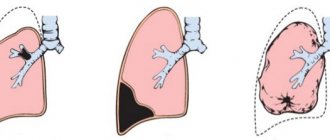
X-ray examination: increased peripheral transparency of the lung fields, the roots of the lungs are enlarged, the borders of the heart are shifted to the right, the shadow of the arch of the dilated pulmonary artery is visible on the left along the cardiac contour.
photo: pulmonary hypertension on x-ray
Functional breathing tests, qualitative and quantitative analysis of the composition of gases in the blood: the level of respiratory failure and the severity of the disease are revealed.
Echo-cardiography: the method is very informative - it allows you to calculate the average pressure in the pulmonary artery (MPAP) and diagnose almost all heart defects. PH is recognized already in the initial stages, with MPAP ≥ 36 – 50 mm.
Scintigraphy: for PH with blocking of the lumen of the pulmonary artery by a thrombus (thromboembolism). The sensitivity of the method is 90 - 100%, specific for thromboembolism is 94 - 100%.
Computer (CT) and magnetic resonance imaging (MRI): at high resolution, in combination with the use of a contrast agent (with CT), they allow you to assess the condition of the lungs, large and small arteries, walls and cavities of the heart.
Inserting a catheter into the cavity of the “right” heart, testing the vascular response: determining the degree of PH, blood flow problems, assessing the effectiveness and relevance of treatment.
Predictions and consequences
Without proper treatment, the average life expectancy for pulmonary hypertension is 2.5 years. The disease progresses from the primary stage to the secondary stage, the signs of the disease worsen, and the condition noticeably worsens.
Against the background of insufficient oxygen supply to the tissues, severe and frequent shortness of breath develops, which occurs even in a calm state. Hypoxia leads to an increase in blood viscosity - blood clots appear, which can clog the vessels in the lungs.
Average pulmonary artery pressure is an important factor in life expectancy. If the indicators remain consistently above 30 mmHg. Art. and do not decrease under the influence of medications - life expectancy is about 5 years.
Important! Positive prognoses can be made if therapy with calcium channel blockers leads to an improvement in the patient’s condition, and the signs of the disease gradually recede. In this case, only 5% of patients live less than 5 years.
Pulmonary hypertension often leads to disability. With this disease, many types and working conditions are contraindicated - heavy physical labor, mental work with high nervous overload and heavy speech load. People with this diagnosis are prohibited from working in rooms with high humidity, strong changes in temperature and pressure.
If you have pulmonary hypoxia, you should not work in hazardous industries - dust, irritating gases, poisons and other allergens can worsen the patient's condition.
Causes of pulmonary hypertension
PH can be a solo (primary) form of the disease, or develop after exposure to another underlying cause.
The causes of PH are not fully understood. For example, in the 60s of the last century in Europe there was an increase in the disease caused by the uncontrolled use of oral contraceptives and diet pills.
In Spain, a similar surge was noted due to the popularization of rapeseed oil. Of the 20 thousand cases, 2.5% were diagnosed with PH. Later, scientists named the amino acid tryptophan as the reason for the boom.
If endothelial function is impaired, the prerequisite may be a genetic predisposition or exposure to external aggressive factors. In each case, this leads to disruption of the metabolic processes of nitric oxide, changes in vascular tone (the appearance of spasms, inflammation), proliferation of the internal walls of blood vessels with a simultaneous reduction in their lumen.
The increased concentration of endothelin (a substance that constricts blood vessels) is explained either by increased secretion in the endothelium or by a decrease in its breakdown in the lungs. The sign is characteristic of idiopathic PH, congenital childhood heart defects, and systemic diseases.
The production or availability of nitric oxide is disrupted, the synthesis of prostacyclin is reduced, the excretion of potassium is increased - any deviation provokes arterial spasm, proliferation of arterial walls, and impaired blood flow in the pulmonary artery.
The following factors can also increase pressure in the pulmonary arteries:
Cardiac pathologies of various origins; Chronic lung diseases (such as tuberculosis or bronchial asthma); Vasculitis; Metabolic disorders; PE and other pulmonary vascular problems; Long stay in high mountains.
If the exact cause of PH is not established, the disease is diagnosed as primary (congenital).
Disability
Is there any disability for pulmonary hypertension? Yes, to obtain it you need to pass a special commission. Documents you must provide:
- chest x-ray;
- spirography;
- blood acid-base and blood gas results;
- echocardiography.
What disability group can be assigned for pulmonary hypertension? With a strongly progressive underlying disease, which causes limited ability and the inability of the patient to care for himself independently, the inability to move is determined by disability of the first degree.
If unstable or insignificant improvements are observed during therapy, the patient has limitations in independent care and movement - disability group II is assigned. Sometimes the patient is recommended to work at home or in specially created conditions.
When determining disability group III, a person can engage in light physical labor even in industrial conditions, mental work with moderate mental and emotional overload.
The disease code for primary pulmonary hypertension in the International Classification of Diseases (ICD 10) is 127. Secondary is 128.8.
Pulmonary hypertension is a serious disease with a high mortality rate. You can avoid illness by giving up bad habits and timely consultations with doctors, even with a slight deterioration in your health.
Main forms of PH
Primary, idiopathic pulmonary hypertension (from the Greek idios and pathos - “a peculiar disease”): is fixed by a separate diagnosis, in contrast to secondary PH associated with other diseases. Variants of primary PH: familial PH and hereditary predisposition of blood vessels to dilation and bleeding (hemorrhagic telangiectasias). The cause is genetic mutations, the frequency is 6–10% of all cases of PH. Secondary PH: manifests itself as a complication of the underlying disease.
Systemic connective tissue diseases - scleroderma, rheumatoid arthritis, systemic lupus erythematosus.
Congenital heart defects (with blood shunting from left to right) in newborns, occurring in 1% of cases. After corrective blood flow surgery, the survival rate of this category of patients is higher than that of children with other forms of PH.
Late stages of liver dysfunction, pulmonary-hepatic vascular pathologies in 20% give a complication in the form of PH.
HIV infection: PH is diagnosed in 0.5% of cases, survival rate within three years drops to 21% compared to the first year – 58%.
Intoxication: amphetamines, cocaine. The risk increases three dozen times if these substances were used for more than three months in a row.
Blood diseases: with some types of anemia, PH is diagnosed in 20–40%, which increases mortality among patients.
Chronic obstructive pulmonary disease (COPD), the cause is prolonged inhalation of particles of coal, asbestos, shale and toxic gases. It often occurs as an occupational disease among miners and workers in hazardous industries.
Sleep apnea syndrome: partial cessation of breathing during sleep. Dangerous, detected in 15% of adults. The consequence may be PH, stroke, arrhythmias, and arterial hypertension.
Chronic thrombosis: noted in 60% after survey of patients with pulmonary hypertension.
Lesions of the heart, its left half: acquired defects, coronary disease, hypertension. About 30% is associated with pulmonary hypertension.
Hypertensive crises in the vessels of the “small circle”
A crisis course often accompanies pulmonary hypertension associated with heart defects. A sharp deterioration in the condition due to a sudden increase in pressure in the pulmonary vessels is possible once a month or more often.
Patients note:
- increased shortness of breath in the evening;
- feeling of external compression of the chest;
- severe cough, sometimes with hemoptysis;
- pain in the interscapular region radiating to the anterior sections and sternum;
- cardiopalmus.
Upon examination, the following is revealed:
- patient's agitated state;
- inability to lie in bed due to shortness of breath;
- pronounced cyanosis;
- weak rapid pulse;
- visible pulsation in the area of the pulmonary artery;
- swollen and pulsating neck veins;
- excretion of copious amounts of light-colored urine;
- involuntary defecation is possible.
Externally, the crisis looks like an attack of sudden suffocation, cyanosis and tachycardia. Unlike cardiac asthma, it lasts several hours and is accompanied by pain in the heart area, impaired inhalation and exhalation, and pulsation in the epigastrium. An attack of bronchial asthma is characterized by an increase in the number of dry wheezes during auscultation.
Cardiac output
Cardiac output (CO) (along with CO, the concept of “cardiac minute volume” - MCV) is often used. If ventricular filling is maintained at a sufficient level, then the magnitude of cardiac output at any stroke volume depends on the heart rate (HR). Calculation formula: SV or MOS = (SV • HR) l/min. Thus, CO is a function of stroke volume and heart rate. An increase in CO during tachycardia requires more efficient diastolic filling of the heart.
As the heart rate increases, the relative time of diastole decreases compared to the duration of systole. However, in a normally functioning heart, which contracts within 170 beats/min, its filling does not decrease due to shortening of diastole.
In an intact heart, during tachycardia, the process of relaxation of the heart muscle is accelerated, which ensures faster and more complete filling of the heart with blood during shortened diastolic periods. This effect is partially mediated through stimulation of p-receptors by catecholamines, which increase the relaxation of cardiomyocytes due to the accelerated removal of intracellular Ca2+ from them. With excessive tachycardia (more than 170 beats/min), such complete diastolic relaxation may not occur, and therefore a further increase in CO.
Pulmonary hypertension 1, 2 degrees - treatment, symptoms and prognosis
Heart problems occur for various reasons. An increase in pressure in the pulmonary artery is one of them. This disorder at stages 1 and 2 has almost no symptoms and signs, but requires mandatory treatment - only in this case there will be a positive prognosis for a person’s life.
What it is
Contrary to the name, the disease “pulmonary hypertension” does not involve problems with the lungs at all, but with the heart, when the blood pressure of the pulmonary artery and the vessels coming from it increases. Most often, the pathology is provoked by other heart problems; in rare cases, it is considered as a primary pathology.
For this part of the circulatory system, normal pressure is up to 25/8 millimeters of mercury (systolic/diastolic). Hypertension is indicated when the values rise above 30/15.
Analyzing medical statistics, we can say that pulmonary hypertension is rare, but even its 1st degree is very dangerous, which must be treated, otherwise the life prognosis is unfavorable and a sharp rise in pressure can result in the death of the patient.
Photo 1. Pulmonary artery in normal conditions and with hypertension
The causes of the disease are a decrease in the internal diameter of the vessels of the lungs, since the endothelium, which is the inner vascular layer, grows excessively in them. As a result of impaired blood flow, the supply of blood to distant areas of the body and limbs deteriorates, which has certain symptoms and signs, which we will discuss below.
The heart muscle, receiving appropriate signals, compensates for these shortcomings by starting to work and contract more intensely. When such a pathological problem exists, the muscle layer in the right ventricle thickens, which leads to an imbalance in the functioning of the entire heart. This phenomenon even received a separate name - cor pulmonale.
Pulmonary hypertension can be detected using an electrocardiogram, but for an early stage the changes will be insignificant and may be missed, therefore, for accurate diagnosis and timely treatment, older people need to know what pulmonary hypertension is, its signs and symptoms. Only in this case can the disease be identified and treated in a timely manner, maintaining a good prognosis for life.
ICD-10 code
Pulmonary hypertension according to the international classification of diseases ICD-10 belongs to class I27 .
Causes
To date, the exact cause of the disease has not been identified. Improper endothelial growth is often associated with internal imbalances in the body, due to improper nutrition and intake of elements such as potassium and sodium. These chemicals are responsible for the narrowing and dilation of blood vessels; if they are deficient, vascular spasm may occur.
Another common cause of pulmonary hypertension is a hereditary factor. The presence of pathology in one of the blood relatives should be the reason for a narrow examination and, if necessary, treatment at an early stage, when symptoms have not yet manifested.
Often, disturbances appear in other heart diseases - congenital heart disease, obstructive pulmonary disease and others. In such cases, pulmonary hypertension is diagnosed as a complication and it is necessary to act primarily on its root cause.
The proven reason is the consumption of special amino acids that affect the growth of endothelium. Several decades ago, it was noted that consumption of rapeseed oil, which contains these amino acids, led to an increase in cases of the disease. As a result, studies were conducted that confirmed that rapeseed has a high concentration of tryptophan, which causes moderate pulmonary hypertension and increases the risk of severe consequences.
In some cases, the reasons are the use of hormonal contraceptives, drugs for sudden weight loss and other drugs that lead to disruption of the internal functionality of the human body.
Symptoms depending on the degree
Finding out about pulmonary hypertension at an early stage is a great success, since in most situations there are no obvious symptoms. However, if you take a closer look and listen to yourself, you can detect some signs of moderate hypertension.
The main symptom is decreased physical capabilities, when a person constantly feels general weakness, for which there are no obvious reasons. Often, when undergoing an examination, the disease in question is discovered at different stages. Let's look at the different degrees of pulmonary hypertension, what symptoms they differ in, what they threaten and what treatment they require.
- The first degree ( I) is expressed by a rapid pulse, the presence of physical activity is perceived relatively easily, no other symptoms are observed, which complicates the diagnosis.
- In the second degree ( II) , the patient already clearly feels a loss of strength, suffers from shortness of breath, dizziness and chest pain.
- In a patient with the third degree ( III), a comfortable state occurs only during inactivity; any physical activity causes an exacerbation of the symptoms of shortness of breath, fatigue, etc.
- The fourth degree ( IV) is considered the most severe. Pulmonary hypertension of this stage is accompanied by chronic fatigue, observed even after waking up at night, all signs are present even at rest, blood may be coughed up, fainting occurs, and the neck veins swell. With any load, all symptoms sharply worsen, accompanied by cyanosis of the skin and possible pulmonary edema. A person, in fact, turns into a disabled person who has difficulty even basic self-care.
Pulmonary hypertension of the 1st degree is distinguished only by a rapid heartbeat; an experienced doctor can detect it on an ECG and send it for additional testing of the pulmonary vessels. Stage 2 pulmonary hypertension is characterized by more obvious symptoms, which cannot be ignored and it is important to visit a cardiologist or therapist without delay.
It is very important to detect violations as early as possible. It is difficult to do this, but, ultimately, the prognosis of life depends on this, and how long the patient will live.
Diagnostics
The process of making a diagnosis is no less important, since it is very easy to miss the disease at an early stage of development. Pulmonary hypertension is first visible on the ECG. This procedure serves as the starting point for the detection and treatment of this disease.
The cardiogram will show abnormal functioning of the cardiac myocardium, which is the first reaction of the heart to problems of a pulmonary nature. If we consider the diagnostic process as a whole, it consists of the following stages:
- ECG, which shows overload in the right ventricle;
- X-ray showing the pulmonary fields along the periphery, the existence of a displacement of the border of the heart from the norm in the right direction;
- Carrying out breath tests to check what the exhaled carbon dioxide consists of;
- Echocardiography procedure. This is an ultrasound of the heart and blood vessels, which allows you to measure the pressure in the pulmonary artery.
- Scintigraphy, which allows you to examine in detail the necessary vessels using radioactive isotopes;
- If it is necessary to clarify X-ray images, more accurate CT or MRI are prescribed;
- The feasibility of future treatment is assessed using catheterization. Using this method, information about blood pressure in the desired cavities is obtained.
Treatment of pulmonary hypertension
Detecting pathology is a difficult task, but treating hypertension is no easier. The effectiveness of treatment is largely determined by the stage of development; in the first stages, there are methods of conservative therapy with the help of drugs; in case of serious development, when the prognosis is poor, there is a threat to life and it is impossible to be cured with drugs, surgery is prescribed.
The treatment is carried out by a cardiologist . Once symptoms are detected and confirmed, the first step is to reduce the likelihood of severe consequences that accompany pulmonary hypertension. To do this you need:
- If there is a pregnancy, refuse further pregnancy, since the mother’s heart during such a period is subjected to severe overload, which threatens the death of both mother and child.
- Eat limited food, do not pass it on, follow a diet with reduced consumption of fatty and salty foods. You also need to drink not much - up to one and a half liters of liquid per day.
- Do not overdo physical activity, unloading the already overloaded cardiovascular system.
- Get the necessary vaccinations to protect against diseases that can indirectly worsen the disease.
Psychologically, the patient also needs additional help, since treatment and subsequent life often have to be completely changed in order to avoid risky situations. If this disease is a secondary complication of another pathology, then the main disease requires treatment first of all.
Conservative treatment of pulmonary hypertension itself sometimes lasts for several years, when it is necessary to regularly take a complex of prescribed medications that suppress the progression of endothelial proliferation. During this period, the patient should take:
- Antagonists that suppress the process of pathological cell division.
- Drugs that prevent the formation of blood clots in blood vessels and reduce their spasm.
- Use oxygen therapy, the purpose of which is to saturate the blood with oxygen. With moderate pulmonary hypertension, the procedure is not required, but with severe pulmonary hypertension, it is necessary constantly.
- Means for thinning the blood and accelerating its flow.
- Drugs with a diuretic effect.
- To normalize the heart rate, glycosides are prescribed.
- If necessary, medications are taken to expand the arterial lumen, which lowers blood pressure.
- Treatment with nitric oxide is carried out when the effectiveness of other methods is low. As a result, the pressure indicator in the entire vascular system decreases.
Surgery
Surgery is used in conditions where pulmonary hypertension is caused, for example, by cyanotic heart disease, which cannot be treated by other means.
As a surgical therapy, balloon atrial septostomy is performed, when the septum between the atria is cut and expanded with a special balloon. This allows oxygenated blood to flow into the right atrium, which reduces the symptoms and severity of pulmonary hypertension.
In the most severe cases, a lung or heart transplant may be required. Such an operation is very complex, has a lot of limitations, and there are great difficulties in finding donor organs, especially in Russia, but modern medicine is able to carry out such manipulations.
Prevention
Preventive measures to prevent pulmonary hypertension are very important. This is especially true for people in risk groups - if they have a heart defect, if there are relatives with the same disease, after 40-50 years. Prevention consists of maintaining a healthy lifestyle, in particular it is important:
- Quit smoking, as tobacco smoke is absorbed by the lungs and enters the bloodstream.
- In hazardous occupations, for example, miners and construction workers, they constantly have to breathe dirty air saturated with microparticles. Thus, it is imperative to comply with all labor protection standards for this type of activity.
- Strengthen the immune system.
- Avoid psychological and physical overload that affects the health of the cardiovascular system.
It is impossible to say exactly how long people with this disease live. With a moderate degree and compliance with all recommendations of the cardiologist, pulmonary hypertension has a positive prognosis.
Author: site editor, date March 28, 2018
Classification of pathology
Taking into account the etiology and mechanisms of the appearance of hypertension, several forms of pathology have been identified.
Idiopathic
Occurs in patients who have no changes in the lungs, heart, blood vessels, and there are no known factors for increased risk of hypertension in the branches of the pulmonary artery. It often has a rapidly progressive course and is fatal. It is very rare - one case per million population per year.
Hereditary
More than half of the patients with a family history of pulmonary hypertension turned out to be carriers of genes responsible for the formation of growth factor receptors and bone marrow proteins. These proteins stimulate the proliferation of cells in the muscle layer of blood vessels and the destruction of the inner lining of the arteries. Also hereditary forms include hemorrhagic telangiectasia - the appearance of arteriovenous malformations in the skin, liver, and lungs.
Precapillary
Due to hypertrophy of the muscle fibers of the arteries, a reflex spasm of small vessels occurs. It happens with lung diseases, chest pathology, blockage of blood vessels, during a long stay in a high-mountain climate, the Arctic.
Capillary
Compression of the capillaries occurs with pathological expansion of the respiratory tract. Occurs in bronchial asthma, emphysema, compaction of lung tissue, pneumosclerosis (replacement of partitions between alveoli with scar tissue fibers).
Post-capillary
Associated with diseases of the left chambers of the heart, impaired outflow of arterial blood due to incompetence of the sphincters of the veins carrying blood to the left atrium.
Arteriovenous
Diagnosed with congenital defects of valves and great vessels, if there is a discharge of blood into the right sections, overflow of the pulmonary circulatory system.
Causes
Pulmonary hypertension in most cases develops secondary, against the background of other heart diseases.
So far, scientists have not been able to establish the causes of the development of such a rare disease as idiopathic pulmonary hypertension. It is assumed that its occurrence may be caused by gene mutations, autoimmune diseases or the use of oral contraceptives.
Secondary pulmonary hypertension is a pathological condition that can be provoked by various chronic diseases of the lungs, blood vessels, heart and some other systems and organs. Most often, this complication is provoked by the following ailments:
- heart failure;
- myocardial infarction;
- cardiac ischemia;
- myocarditis;
- congenital and acquired heart defects (mitral stenosis, septal defects, etc.);
- diseases accompanied by pulmonary embolism;
- neoplasms of the lungs and heart;
- chronic inflammatory and obstructive processes in the lungs and bronchi (tuberculosis, pneumosclerosis, emphysema, sarcoidosis);
- vasculitis localized in the pulmonary artery area;
- pulmonary-hepatic vascular pathologies and late stages of liver dysfunction;
- disorders of the structure of the chest and spinal column (kyphoscoliosis, ankylosing spondylitis, Pickwick syndrome in obesity, errors about thoracoplasty);
- blood pathologies: chronic hemolytic anemia, myeloproliferative diseases, condition after splenectomy.
In addition, pulmonary hypertension can be provoked by a number of acute diseases and conditions:
- respiratory distress syndrome, caused by an autoimmune or toxic lesion and leading to an insufficient amount of surfactant on the lobules of lung tissue;
- severe diffuse pneumonitis, accompanied by a strong allergic reaction to inhaled odors of perfumes, paints, flowers, etc.;
- taking certain medications and exposure to toxins (toxic rapeseed oil, Aminorex, amphetamines, Fenfluramine, L-tryptophan, cocaine, cytostatics, etc.);
- taking traditional medicine or food products.
Statistics indicate that those most likely to develop pulmonary hypertension are HIV-infected people, drug addicts, people taking medications to suppress appetite, patients with arterial hypertension and pregnant women.
Pulmonary hypertension in newborns can be caused by the following conditions:
- general hypoxia;
- diaphragmatic hernia;
- meconium aspiration;
- continued fetal circulation.
Pulmonary hypertension with mitral stenosis and atherosclerosis
The disease varies in severity. Mitral stenosis contributes to the occurrence of atherosclerotic lesions of the pulmonary artery in 40% of patients due to increased pressure on the vessel wall. Functional and organic mechanisms of hypertension are combined.
The narrowed left atrioventricular passage in the heart is the “first barrier” to blood flow. If there is narrowing or blockage of small vessels, a “second barrier” is formed. This explains the failure of surgery to eliminate stenosis in the treatment of heart disease.
By catheterization of the heart chambers, high pressure inside the pulmonary artery is detected (150 mm Hg and above).
Vascular changes progress and become irreversible. Atherosclerotic plaques do not grow to large sizes, but they are sufficient to narrow small branches.
X-ray of cor pulmonale shows bulging of the pulmonary artery arch
What causes primary hypertension?
Primary pulmonary hypertension is also called idiopathic, isolated. The prevalence of the pathology is 2 people per 1 million inhabitants. The definitive reasons remain unclear.
It has been established that women make up 60% of patients. Pathology is detected both in childhood and in old age, but the average age of identified patients is 35 years.
In the development of pathology, 4 factors are important:
- primary atherosclerotic process in the pulmonary artery;
- congenital inferiority of the wall of small vessels;
- increased tone of the sympathetic nerve;
- vasculitis of the pulmonary vessels.
The role of the mutating bone protein gene, angioproteins, their influence on the synthesis of serotonin, and increased blood clotting due to the blocking of anticoagulant factors has been established.
A special role is given to infection with the herpes virus type eight, which causes metabolic changes leading to the destruction of arterial walls.
The formation of thrombotic masses leads to blockage of the lumen of the arteries
The result is hypertrophy, then expansion of the cavity, loss of right ventricular tone and the development of failure.
Forecast
Without treatment, the average survival time for patients is 2.5 years. Treatment with Epoprostenol increases the lifespan to five years in 54% of patients. The prognosis of pulmonary hypertension is unfavorable. Patients die from increasing right ventricular failure or thromboembolism.
Patients with pulmonary hypertension due to heart disease and arterial sclerosis live up to 32–35 years of age. The crisis course aggravates the patient’s condition and is regarded as an unfavorable prognosis.
The complexity of the pathology requires maximum attention to cases of frequent pneumonia and bronchitis. Prevention of pulmonary hypertension consists of preventing the development of pneumosclerosis, emphysema, early detection and surgical treatment of congenital defects.
What it is?
Pulmonary hypertension is a type of hypertension characterized by increased pressure in the arteries of the lungs. The result of the pathology is a narrowing of the lumen in the lung vessel due to the abnormal structure of the arteries of the respiratory organs. It is more typical for women of the middle age group. Men are three times less likely to be diagnosed with this pathology.
The disease manifests itself almost asymptomatically in the initial stages of its course. A person may not even be aware of its presence until the disease manifests itself with symptoms such as hypertensive crisis, pulmonary edema, and hemoptysis. That is, when the degree of development of the disease is high, the patient seeks medical help, which significantly complicates treatment.
With pulmonary hypertension of the 1st degree, there is no shortness of breath and pain in the chest, there are no unpleasant sensations during normal walking, and there are none during other moderately active actions of the body. Excessive fatigue and weakness are not observed.
Hypertension is classified according to several parameters:
- Tipu
- Current
- Severity of the disease
At the diagnostic stage, the main factor indicating the presence of this pathology is increased pulmonary pressure in a calm and active state of the body. It is measured in millimeters of mercury. The parameters are established by ICD-10 (International Classification of Diseases) and should be no more than 25 (at rest) and 35 (during certain physical activities). The ICD 10 code for pulmonary hypertension (127.0) is established only for diseases of the primary type.
Primary pulmonary hypertension
The primary and secondary types of the disease can only be determined by exclusion. Secondary pulmonary hypertension appears as a result of acquired diseases, that is, it is the result of the negative impact of other diseases on the circulatory system.
Causes of hypertension:
- Chronic inflammatory processes such as tuberculosis, liver cirrhosis, pneumosclerosis
- Neoplasms in the heart muscle or respiratory tract
- Blood clots
- Pathologies in the structure of the spine or chest
- Congenital heart defect
The list of causes of idiopathic pulmonary hypertension includes:
- Autoimmune pathologies
- Heredity
- Development of atherosclerosis in arterial branches
- Increased sympathetic nerve tone
- Congenital defects of pulmonary capillaries in the fetus
- Pulmonary vasculitis
- Oral contraceptives
- Herpes virus type No. 8
Most often, specialists find it difficult to determine the mechanism of development of primary pulmonary hypertension. Let us recall that ICD 10 assigns code 127.0 to primary pulmonary hypertension.
Symptoms of the primary type of hypertension include:
- Shortness of breath varies in nature - from minimal to significant, appearing during heavy exertion or at rest. As a rule, there are no asthma attacks.
- Fainting and dizziness, lasting up to 5 minutes. Appear during significant physical exertion.
- Painful sensations of various types in the chest area. Duration ranges from a few minutes to several hours. Typically, taking medications that have a positive effect on vasodilation does not relieve pain.
- Dry cough, which can appear both during exercise and at rest.
- Interruptions in the functioning of the heart muscle.
- Sputum with blood during expectoration (single or continuous).
Degrees of development and forms of flow
Depending on the severity of the course, several degrees of development are distinguished. At each stage, the disease manifests itself more clearly, limiting the patient in certain actions.
The first degree (average systolic pressure in the range of 25-45 mm Hg) – subtle symptoms with preservation of physical activity. Absence of dizziness and shortness of breath with a traditional lifestyle.
Second degree (average systolic pressure 45-75 mm Hg) – there is respiratory failure with persistently elevated blood pressure. Chest pain and dizziness, the first signs of cardiac ventricular hypertrophy, are diagnosed.
The third degree (average systolic pressure from 76 to 110 mm Hg) is an irreversible stage with formed vascular atherosclerosis and complete hypertrophy of the heart ventricle. Previously identified manifestations include hemoptysis and an obsessive, prolonged cough. Small loads cause severe shortness of breath, and significant swelling appears in the legs and in the area of the lymph nodes.
The fourth degree (average systolic pressure above 110 Hg) is high pulmonary hypertension, in which a person becomes incapacitated and cannot partially or fully care for himself without outside help. There is significant swelling of the lower extremities, a number of concomitant diseases appear, for example, the liver increases in size, diffuse cyanosis. Pain in the chest area and severe shortness of breath are present at rest.
According to the course, pulmonary hypertension is divided into acute and chronic. Provocateurs of the acute type are hypertensive crisis, myocardial infarction, pulmonary embolism, etc. Increased blood pressure in the left atrium, obstructive respiratory diseases, and other causes of narrowing of the pulmonary arteries are provocateurs for the development of the chronic type.
Clinical picture
Symptoms of pulmonary hypertension appear if the pressure in the pulmonary artery is increased by 2 times or more. Patients with hypertension in the pulmonary circle notice:
- shortness of breath, which worsens with physical activity (can develop in paroxysms);
- general weakness;
- rarely loss of consciousness (as opposed to neurological causes without convulsions and involuntary urination);
- paroxysmal chest pains, similar to angina pectoris, but accompanied by an increase in shortness of breath (scientists explain them by a reflex connection between the pulmonary and coronary vessels);
- the admixture of blood in the sputum when coughing is characteristic of significantly increased pressure (associated with the release of red blood cells into the interstitial space);
- hoarseness is detected in 8% of patients (caused by mechanical compression of the recurrent nerve on the left by the dilated pulmonary artery).
The development of decompensation as a result of pulmonary heart failure is accompanied by pain in the right hypochondrium (liver stretching), swelling in the feet and legs.
The patient feels unable to take a breath
When examining a patient, the doctor pays attention to the following:
- a blue tint to the lips, fingers, ears, which intensifies as shortness of breath becomes more severe;
- the symptom of “drum” fingers is detected only in long-term inflammatory diseases and defects;
- the pulse is weak, arrhythmias are rare;
- blood pressure is normal, with a tendency to decrease;
- palpation in the epigastric zone makes it possible to determine increased impulses of the hypertrophied right ventricle;
- On auscultation, an accentuating second sound on the pulmonary artery is heard, and a diastolic murmur is possible.
The relationship of pulmonary hypertension with persistent causes and certain diseases allows us to distinguish variants in the clinical course.
Classification and prognosis
The classification is based on the principle of functional disorders in PH, the version is modified and is associated with manifestations of heart failure (WHO, 1998):
Class I: PH with normal physis. activity. Standard loads are well tolerated, mild PH, grade 1 failure. Class II: LH plus decreased activity. Comfort in a quiet position, but dizziness, shortness of breath and chest pain begin even with normal exertion. Moderate pulmonary hypertension, increasing symptoms. Class III: PH with decreased initiative. Problems even at low loads. High degree of blood flow disturbances, worsening prognosis. Class IV: PH with minimal activity intolerance. Shortness of breath and fatigue are felt even at complete rest. Signs of high circulatory failure are congestive manifestations in the form of ascites, hypertensive crises, pulmonary edema.
The prognosis will be more favorable if:
The rate of development of PH symptoms is low; The treatment improves the patient's condition; The pressure in the pulmonary artery system decreases.
Poor prognosis:
Symptoms of PH develop dynamically; Signs of decompensation of the circulatory system (pulmonary edema, ascites) are increasing; Pressure level: in the pulmonary artery more than 50 mmHg; With primary idiopathic PH.
The overall prognosis for pulmonary arterial hypertension is related to the form of PH and the phase of the prevailing disease. Mortality per year, with current treatment methods, is 15%. Idiopathic PH: patient survival after a year is 68%, after 3 years - 48%, after 5 years - only 35%.
Portopulmonary hypertension
Pulmonary hypertension leads to a simultaneous increase in portal vein pressure. In this case, the patient may or may not have cirrhosis of the liver. It accompanies chronic liver diseases in 3–12% of cases. The symptoms are no different from those listed. Swelling and heaviness in the hypochondrium on the right are more pronounced.
Treatment of this form depends on the possibility of restoration of liver tissue. During liver transplantation, the condition is taken into account as a relative contraindication, since the risk of complications and death increases.
Development mechanism
The development of pulmonary hypertension is provoked by a gradual narrowing of the lumen of the vessels of the pulmonary artery bed - capillaries and arterioles. Such changes are caused by thickening of the inner layer of blood vessels - the endothelium. In a complicated course, this process may be accompanied by inflammation and destruction of the muscular layer of the pulmonary artery.
The narrowing of the lumen of blood vessels causes constant sedimentation of blood clots in it and leads to its obliteration. Subsequently, the patient's pressure in the pulmonary artery system increases and pulmonary hypertension develops. This process increases the load on the right ventricle of the heart. Initially, its walls hypertrophy, trying to compensate for hemodynamic disturbances. Subsequently, due to constant loads, their contractility decreases and a stage of decompensation develops, expressed in right ventricular failure.
Factors causing hypertension in the pulmonary circulation
The main factors of pathology, according to V. Parin’s classification, are divided into 2 subtypes. Functional factors include:
- constriction of arterioles in response to low oxygen levels and high concentrations of carbon dioxide in the inhaled air;
- increase in minute volume of passing blood;
- increased intrabronchial pressure;
- increased blood viscosity;
- left ventricular failure.
Anatomical factors include:
- complete obliteration (blocking of the lumen) of blood vessels by a thrombus or embolus;
- impaired outflow from the zonal veins due to their compression due to aneurysm, tumor, mitral stenosis;
- changes in blood circulation after surgical removal of a lung.
What is pulmonary hypertension (increased pressure in the pulmonary artery)
Pulmonary hypertension is a complex of various pathologies that are united by a single symptom - high pressure in the arteries of the lungs, which provokes an increased load in the right ventricle. The vascular system gradually becomes clogged, and the clearance between the walls decreases. All this provokes disruption of the correct functioning of the heart.
The disease is accompanied by a whole range of symptoms:
- increased fatigue;
- shortness of breath, feeling of lack of air;
- dizziness;
- pain, compression in the chest area.
Pulmonary hypertension is considered a serious, life-threatening disease
In addition to noticeable discomfort, this disease can cause serious disruptions in the functioning of the body, when surgical intervention is necessary.