Often, a child’s lack of bowel movements for several days does not cause any concern. Especially if such an incident happens to an adult. Sometimes this symptom really does not pose any threat. But there are cases when persistent constipation leads to harmful changes in the intestines, its expansion and retention of feces. This condition, known as megacolon, can be caused by congenital abnormalities or a number of associated factors. In any case, this condition requires immediate treatment, otherwise it threatens with dangerous complications.
- 2 Types of disease
2.1 Photo gallery: manifestations of megacolon in adults and children
- 2.2 Video about Hirschsprung's disease
- 4.1 Differences in the manifestations of congenital and acquired forms of the disease - table
4.1.1 Symptoms of pathology in the photo
- 5.1 Diet
5.1.1 Photo gallery: basic nutrition during illness
- 5.2.1 Agents used for the symptomatic treatment of megacolon - table
What is megacolon?
This is a concept that combines a complex of similar symptoms from the large intestine, resulting from various congenital and acquired causes. Megacolon is characterized by an increase in length or proliferation (hypertrophy) of the intestinal wall in one area of the colon or throughout the entire colon.
The condition occurs among adults and among children of various age groups. Megacolon in an adult is a disease that occurs as a result of the action of damaging factors on the intestines from the outside (infection, toxins, etc.); megacolon in children is, as a rule, a congenital pathology.
Megacolon is a congenital or acquired disease that manifests itself as an enlargement of the colon
Interestingly, megacolon was identified in 1886 by pediatrician G. Hirschsprung, who noticed an “unusual disease” of the colon in some children, manifested by persistent constipation. This pathology was unlike any other intestinal disease previously known. Since the development of the disease was based on the “large colon,” the pathology was called megacolon (mega (Greek) - large, colon (Latin) - colon). Subsequently, to this day, it is the congenital form of megacolon that is called Hirschsprung's disease.
Classification
Stages: compensation, subcompensation, decompensation.
There are congenital megacolon and acquired
. The pathological process is also classified as follows: Congenital underdevelopment of the intramural nervous system in areas of the large intestine - Hirschsprung's disease.
Obstacles of a mechanical nature, which are expressed by stenosis, atresia, scars, postoperative deformities - obstructive or functional type
. Stagnation of food gruel initially provokes hypertrophy of the muscle layer due to increased peristaltic movements, then the tone weakens and the intestine undergoes expansion. Functional tissue is replaced by sclerotic tissue. Obstructive type of megacolon is diagnosed in 10% of patients. Mental disorders and associated incorrect eating habits, suppression of the urge to defecate lead to the fact that the colon is in an overstretched position for a long time due to the accumulation of a large volume of feces - the psychogenic type, occurs in 2-5%.
Endocrinological diseases, most often isolated mexidema and cretinism, lead to the development of endocrine megacolon
in 1% of cases.
Toxic megacolon
- one of the manifestations of pathology, occurs against the background of abundant damage by pathogenic microflora, taking laxatives.
Organic damage to the central nervous system (for example, meningoencephalitis) disrupts the motor-evacuation function of the colon due to pathological innervation due to disease - neurogenic megacolon
.
If the cause of colon gigantism cannot be determined, idiopathic megacolon
.
Classification of megacolon in accordance with the anatomical structure:
• rectal option; • rectosigmoidal; • segmental; • subtotal; • total.
ICD-10 code – K53.3
Types of disease
- Hirschsprungs disease. Or congenital megacolon, aganglionic megacolon, congenital intestinal aganglionosis - this form of the disease is the most common cause of intestinal obstruction in newborns. This pathology can be found in one in 5,000 newborns. It is 4 times more common in boys than in girls. It is more often found in premature babies and in children with other hereditary diseases (Down's disease, congenital pulmonary hypoventilation syndrome and others).
- Obstructive megacolon. It occurs in 8–10% of cases and occurs as a result of the appearance of a mechanical obstacle to the passage of feces in the form of stenosis (congenital or acquired narrowing) of the intestine, occlusion of the anus, postoperative adhesions. As a result of this, the sections of the intestine overlying the obstruction begin to increase peristalsis in order to increase the likelihood of feces passing through the intestines; the muscle wall of these sections hypertrophies. Over time, exhaustion sets in, as the effort expended does not lead to the desired result. The muscles, on the contrary, become thinner, the intestine stretches and increases in size.
- Psychogenic megacolon. A form that develops against the background of the patient’s mental illness or the formation of an improper bowel movement. For example, when he postpones defecation for a long time, feces continue to accumulate and the intestine becomes overstretched.
- Endocrine form of megacolon. It can develop against the background of certain diseases of the glands of the internal system (for example, hypothyroidism, diabetes mellitus, pheochromocytoma, etc.). Due to human hormonal imbalances, many regulatory mechanisms, including bowel movements, are disrupted. This leads to constipation and the development of megacolon. That is why in the treatment of endocrine diseases it is necessary to pay attention not only to the main pathology, but also to the accompanying symptoms, in particular constipation.
- Toxic megacolon. This is a type of disease that appears as a result of exposure to various toxins (viral, bacterial) on the intestines and the development of an inflammatory process. This type occurs with ulcerative colitis, Crohn's disease, infectious colitis, as well as with frequent use of laxatives.
- Neurogenic megacolon. This type of disease develops after or against the background of diseases of the central nervous system (meningitis, encephalitis), as a result of which the regulation of many body functions is disrupted, including bowel movements. In this regard, the patient develops persistent constipation, and over time, megacolon.
- Idiopathic megacolon. This disease with an unclear cause unites all cases when it is not clear why the pathology occurred. In some cases, a digital examination of the rectum may reveal a functional muscle spasm or stenosis at the level of the internal anal sphincter in the patient. Sometimes no obstacles to the passage of stool are identified, and the reason for the expansion of the large intestine is unclear. But we should not forget about the possibility of congenital immaturity of the nerve plexuses of the intestine, which during the patient’s life is subject to unfavorable factors in the form of exposure to toxins, vitamin deficiencies, injuries, as a result of which megacolon can develop.
Photo gallery: manifestations of megacolon in adults and children
Hirschsprung's disease is a congenital form of megacolon that occurs due to a lack of nerve cells in the wall of the colon.
In the presence of a mechanical obstruction in the lower parts of the large intestine, a structural type of megacolon develops
A characteristic manifestation of congenital megacolon is an enlarged abdomen
Video about Hirschsprung's disease
DOLICHOMEGACOLON
Dolihomegacolon is an excessive enlargement of the colon, manifested by its elongation and expansion, often with wall hypertrophy and elongation of the mesentery. These changes may be in the nature of a total lesion of the colon, reaching a significant size (colon gigantism), or they may be limited to any part, most often affecting the sigmoid. This pathological condition in some cases is congenital, representing a developmental anomaly, in other cases it is acquired.
There are megacolon and dolichocolon, that is, elongation of the large intestine or its parts, not accompanied by a significant expansion of its lumen; in the latter cases the term macrocolon is sometimes used; megacolon is also referred to as Hirschsprung's disease or Favalli-Hirschsprung's disease. It should be borne in mind, however, that the differentiation of the concepts megacolon and dolichocolon is to a certain extent relative and conditional, since in most cases with megacolon there is an elongation of the colon, and with dolichocolon its expansion with hypertrophy of the walls.
There are no exact data on the frequency of dolichomegacolon. In pathological practice, it is rare: 1: 5000-10,000 autopsies (Ya. L. Rappoport and I. A. Abrikosov); in the clinic, during systematic examination of the gastrointestinal tract, it is observed more often; According to various authors, the percentage of detection of dolichomegacolon ranges from 4-8 to 14. This difference between clinical and anatomical data can be explained, on the one hand, by a broader clinical diagnosis of dolichomegacolon, and on the other hand, by insufficient registration of changes in the colon during autopsies. , characteristic of megacolon, but not clearly expressed (I. E. Sandukovsky).
Dolihomegacolon. Megacolon mainly affects children, but this disease also occurs in adults.
Among the 137 patients observed by V.L. Bogolyubov, 91 were under the age of fifteen years. In males, it is observed 2-3 times more often than in women.
Etiology and pathogenesis. Literature data on the etiology and pathogenesis of dolichomegacolon are characterized by uncertainty and inconsistency. This is explained by the insufficiently clear delineation of the nosological boundaries of this disease, as well as by the fact that practically there are various clinical and anatomical variants of dolichomegacolon, and therefore its origin does not always have the same mechanism. The variety of etiological factors and the complexity of the pathogenesis of this disease should be taken into account.
Among the various theories of the development of dolichomegacolon, the following are most recognized and widespread.
The earliest is the theory that considers dolichomegacolon as a congenital deformity. A similar view was held by Hirschsprung. From this point of view, the disease is a congenital anomaly of the intestine; pathological elongation, expansion and hypertrophy of the colon is a consequence of an embryonic developmental defect, similar to the primary expansion of the esophagus, stomach and other organs.
The evidence is that the disease usually develops in early childhood and is often combined with other developmental anomalies: enlargement and dystopia of the urinary bladder, dystopia of the uterus, vaginal atresia, intestinal diverticula, intestinal dystopia in the form of its right-sided location, malformations of the spinal cord at the level of the lower lumbar vertebrae and others.
Dolihomegacolon. It should be borne in mind that the large intestine can have different shapes and positions and is characterized by various anomalies, which is associated with the complexity of the process of morphological development of the intestine, accompanied by changes in its positions during intrauterine life.
Disruption of the flow of the basic elements of the embryonic process - the growth of the intestinal tube, rotation of the intestinal loop, fusion of the mesentery - causes the occurrence of various variations and anomalies of the large intestine. According to embryology, if the growth of the intestinal tube was normal, but the fusion was delayed, mobility of one or another part of the intestine is observed; in the absence of fusion, mobility of the entire colon with the mesentery occurs; if fusion precedes growth, undescended bowel occurs; in cases where increased growth of the primary loop occurs, the intestine turns out to be excessively long. There is reason to believe that megacolon may be associated not only with this disruption of the process of embryonic development of the intestine, but also with pathological processes during the intrauterine life of the child.
A number of authors, without denying the possibility of the congenital nature of this disease, believe that such cases are extremely rare and can occur only in newborns, appearing immediately after birth and soon leading to death.
Some authors point to the constitutionally congenital nature of the origin of dolichomegacolon in connection with its development as a family disease.
Numerous observations have shown that in some cases megacolon occurs due to disturbances in the normal evacuation function of the intestine, caused by anatomical changes in it, creating a mechanical obstacle to the movement of feces.
Dolihomegacolon. This circumstance was emphasized at the end of the 19th century, when the theory of “intestinal blockage” was proposed to explain the origin of dolichomegacolon.
According to this theory, the disease is based on congenital blockage of the intestine, caused by numerous bends of the sigmoid colon; The resulting stagnation of feces consistently causes a number of phenomena characteristic of dolichomegacolon. The expansion of the intestine in such cases is due to chronic distension by gases and stagnant feces, and hypertrophy of the walls occurs partly as a result of concomitant colitis, but mainly due to increased activity of the intestine during peristaltic movements. Excessive length and mobility of the sigmoid colon is congenital; the formation of megacolon is secondary in such cases.
Various changes of both congenital and acquired nature have been described as mechanical obstacles that contribute to the occurrence of megacolon: bends, narrowings and constrictions of the intestine, the formation of loops and kinks due to significant elongation of the mesentery, descent of the sigmoid flexure and the formation of an intestinal spur, the formation of a valve in the lumen intestines due to excessive development of folds of the transverse colon to the semilunar valve and others.
Local anatomical changes in the intestinal wall, described by various authors, can be of great importance in disrupting the movement of intestinal contents through the large intestine with pronounced stagnation of feces in it and its subsequent expansion.
Dolihomegacolon. First of all, a decrease in elastic tissue in the intestinal wall, vessels and mesentery with the development of connective tissue is indicated, which leads to a weakening of peristaltic ability and subsequent expansion of the intestine.
Concetti attached importance to congenital aplasia of the muscles of the lower segment of the colon, which causes, due to stagnation of feces in the distal segment, expansion and hypertrophy of the overlying sections. The author divides the changes that develop in the colon into three types: macrocolon, megacolon and ectacolon.
Finally, dysfunction of the sympathetic and parasympathetic innervation of the colon, which leads to impaired evacuation of the contents of the colon, is indicated as the cause of the development of gigantism of the colon. This point of view forms the basis of the neurogenic theory of the origin of dolichomegacolon.
Innervation disorders are based, first of all, on morphological disorders, the essence of which is a change in the structure of the nodes of the Auerbach parasympathetic nerve plexus. With megacolon, there is an increase in the deficiency of the nodes of this plexus in the distal direction of the colon, most pronounced in the zone located below the area of its expansion - in the distal sigmoid and in the rectum (the so-called rectosigmoid zone).
Due to the deficiency or absence of parasympathetic plexus nodes, dominance of the tone of the sympathetic (Meissnerian) nerve plexus occurs and spastic contraction of the sigmoid and rectum develops, promoting expansion of the overlying sections, which should be considered as a secondary phenomenon arising as a result of decompensation occurring due to constant overcoming of resistance , provided to the feces by the contracted distal intestine.
Dolihomegacolon. A known role, apparently, also belongs to the disappearance of the reflex that relaxes the sphincter (achalasia), which leads to a delay in bowel movement and, thus, contributes to the stagnation of its contents.
According to A.I. Abrikosov, one should take into account not only a violation of tone, but also a direct violation of intestinal trophism (neurotrophic disorder), accompanied by its increased growth. Changes in the ganglion cells of the Auerbach plexus can apparently be both congenital and acquired. Experimental data (McCarisson, Schimazono) indicate that when animals are fed food devoid of vitamin B1, death of the Auerbach plexus, dilation of the colon, and chronic stasis are observed. A. Netto and S. Netto noted varying degrees of changes in the Auerbach plexus with megacolon that developed in people with low nutrition (vitaminosis B1).
There is evidence indicating that functional disorders of innervation are important in the origin of dolichomegacolon. For example, long-term reflex spasm of sections of the colon, functional disorders in the area of the anal sphincter, in the form of a spasm of the latter due to cracks, viscero-visceral reflexes in the presence of various pathological foci in the abdominal cavity, etc. Of particular importance is the disruption of the activity of the so-called physiological sphincters colon: Payer's sphincter, in the area of the splenic flexure of the transverse colon, as well as the Bally and Mutier-Rossi sphincters, located in the sigma.
Dolihomegacolon. It is necessary to keep in mind dyskinesia of the colon due to a violation of the central regulation of intestinal activity.
The above data explain the development of this disease as secondary to various severe chronic diseases of the abdominal organs, in particular in persons suffering from peptic ulcer disease (G. I. Burchinsky). It is worthy of attention to compare the above data on the role of vitamin B1 deficiency in the origin of changes in the Auerbach nerve plexus and the development of megacolon and the importance that some authors attach to hypovitaminosis B1 in the pathogenesis of gastric and duodenal ulcers.
Consequently, various factors play a role in the origin of dolichomegacolon, and therefore the pathogenesis of this suffering is not only complex, but also varied; this excludes the possibility of creating a unified theory of the origin of dolichomegacolon. Both congenital and acquired factors are involved in the development of this disease.
Congenital ones include: excessive growth of the intestine during the embryonic period, the presence of a congenital mechanical obstruction (kinks and narrowing of the intestine), rectovaginal fistula, excessive development of the transverse fold, insufficient development of the intestinal muscles and elastic elements of the intestinal wall, as well as deficiency of the parasympathetic nerve plexus nodes.
Acquired ones may include: inflammatory peritoneal adhesions and adhesions, cicatricial narrowing, cords and kinks after the inflammatory process and injury, spastic state of the intestinal muscles, sphincter spasms due to cracks in the anus, intestinal atony with prolapse of the sigmoid flexure and the formation of spurs, and others factors, in particular nutritional.
Dolihomegacolon. Some authors tend to attach a certain importance to this latter, if not as an etiological factor, then as a factor that causes and aggravates the disease in persons predisposed to it.
Based on the fact that short intestines are found in carnivores and long intestines in herbivores, in an experiment, when feeding dogs, rabbits and rats with plant foods rich in waste, it was possible to cause an elongation of the large intestine, and when feeding meat, a shortening.
Most often, there is a combination of congenital and acquired factors, while the latter in some cases contribute to the manifestation of the disease and its progression, which explains the occurrence of symptoms of suffering at different periods of the life of patients and their development sometimes in connection with any disease (dysentery, cholelithiasis, peptic ulcer illness and others).
It should be borne in mind that in the pathogenesis of the disease in all cases, additional factors that can be characterized as conditional play a significant role; Among them, disturbances in intestinal motility and tone, the addition of colitis and especially pericolitis are of particular importance.
Depending on the predominance of one or another of the listed factors in a given patient, various variants of dolichomegacolon arise, which served as the basis for the creation of various classifications of the disease in connection with the characteristics of its origin. Accordingly, primary and secondary dolichomegacolon can be distinguished. In the first case, the disease may be caused by congenital underdevelopment of the nodes of the parasympathetic plexus or is a congenital anomaly, which manifests itself either in the form of gigantism of the intestine with predominant expansion and hypertrophy of its walls (Favalli-Hirschsprung disease), or in the form of dolichomegacolon with predominant elongation of the intestine.
Dolihomegacolon. Secondary dolichomegacolon develops either due to congenital or acquired mechanical obstructions, or due to a violation of the innervation of the colon, manifested mainly by elongation of the colon.
Pathological anatomy. The main changes in dolichomegacolon boil down to expansion of the colon, reaching enormous sizes (16-20 cm in circumference in small children and up to 50-76 cm in adults) and accompanied by an inconsistent change in the ratios of the thickness of its individual layers due to hypertrophy of the intestinal layer. There are also cases when not only there is no hypertrophy and the usual ratio of the thickness of the layers of the intestine is observed, but there is thinning of the muscular layer of the bloated intestine.
There is an assumption that such atrophy develops secondarily as the disease progresses (Ya. L. Rappoport and A. I. Abrikosov). The sigmoid colon is most often affected; in approximately half of the cases - in isolation, and in the rest of the cases - in combination with changes in other parts of the colon or the entire colon as a whole (V.L. Bogolyubov, I.E. Sandukovsky). Along with the expansion, lengthening of the colon is also noted. The usual ratio between the length of the small and large intestines, defined as 7:1, with this disease changes to 3:1, accompanied by the formation of kinks.
In pronounced cases of gigantic size, the colon occupies almost the entire abdominal cavity, causing significant displacement of other organs and distorting the usual topography. Enlargement of the intestine most often has a uniform, diffuse, and less often ampulla-like character. The intestine often takes on the appearance of a dense, leathery tube that does not collapse upon cross-section; it contains a huge amount of feces and dense fecal masses, sometimes fecal stones.
Dolihomegacolon. Histological examination also reveals more or less significant changes.
Hypertrophy of the muscle layer is observed both due to an increase in the size of muscle fibers and their number. There is thickening of the mucous membrane due to edema, inflammatory cell infiltration and proliferation of submucosal tissue. Due to the sharp stretching of the intestine, the folds of the mucous membrane are smoothed out; there are often multiple ulcerations such as bedsores, leading to perforation and peritonitis. Significant changes in blood vessels are observed in the form of endo- and periarteritis with their obliteration, as well as the nervous apparatus of the large intestine.
In some cases, hypertrophy of the intramural nerve ganglia is noted, in others there is an absence of ganglion cells of the Auerbach plexus or a significant decrease in their number. Sometimes in the nerve cells of the Auerbach plexus various changes are found in the form of swelling of protoplasm, diffuse chromatolysis, hyperchromic nuclei and proliferation of satellites, as well as a significant increase in nerve trunks, sometimes unchanged, sometimes fragmented, sometimes thickened, sometimes weakly impregnated with silver (A.V. Gabay, 1955). These changes are important from the point of view of the theory of impaired innervation during the development of megacolon.
Clinic. The symptomatology and clinical course of dolichomegacolon vary depending on the pathogenesis: along with severe manifestations, there are cases when dolichomegacolon does not manifest itself during life and is discovered by chance during an X-ray examination or is diagnosed on a section.
Three main clinical forms of dolichomegacolon can be distinguished: 1) latent, or asymptomatic, when the patient does not experience any sensations and dolichomegacolon is discovered by chance; 2) masked, in which, along with pathological changes in the colon, there are other diseases (cholecystitis, appendicitis, peptic ulcer) and, finally, 3) a typical form with pronounced clinical phenomena (E.M. Maergoiz).
Dolihomegacolon. The symptoms and course of the disease vary in accordance with these forms.
The main clinical manifestations of dolichomegacolon are symptoms associated with dysfunction of the colon. The most consistent symptom is constipation (retention of bowel movements for many days or even weeks); Even in cases where bowel function is less affected, periods of sudden release of huge amounts of feces are observed. There are cases when the amount of feces reached 10 kg. This phenomenon is explained by the fact that with dolichomegacolon, the large intestine does not empty completely. In this regard, over time, large amounts of feces accumulate and are periodically released. The smell of feces is often foul and rotten. Cases are described when feces were not excreted at all, but a dark, greenish, foul-smelling liquid came out.
Associated symptoms of constipation: bloating and a feeling of fullness, caused not only by stagnation of feces, but also by gases, as well as pain of a constant or variable nature and varying intensity, in some cases having the character of mild colic, in others pronounced. Dyspeptic symptoms are observed in the form of nausea, heartburn, belching, and sometimes bad breath.
In a number of patients, especially children, their general condition worsens: pallor, exhaustion, and, in severe cases, swelling of the lower extremities. Due to the high position of the diaphragm, there is shortness of breath, tachycardia, and cyanosis. The general appearance of sick children with severe forms of megacolon is very characteristic: thin legs, a small head and a large, swollen, elongated abdomen, since fecal retention leads to significant distension of the colon and the abdomen reaches enormous sizes; if these phenomena are constant, the abdominal wall stretches, becomes thinner, when examining the patient, separate loops of intestines are visible, often especially in children, peristalsis of dilated intestinal loops is determined, sometimes dilated veins and a protruded navel are visible.
Dolihomegacolon. On palpation of the abdominal cavity, individual intestinal loops appear dilated, thickened, and in some cases, with a soft abdominal wall, it is possible to trace the course of the intestinal loop.
In some cases, due to the accumulation of feces, a picture of a “fecal tumor” appears; sometimes general or partial splanchnoptosis is noted. When digitally examining the anus, increased tone of the rectal sphincter is noted.
In case of prolonged stool retention, the patient's condition may worsen, intoxication, weakness, and vomiting may increase.
During the period of exacerbation of the disease, the intensity of the symptoms increases, the symptoms become more diverse. Exacerbations can manifest themselves in the form of colitis: pain increases, takes on the character of cutting, rumbling appears, constipation is replaced by increased frequency of stools with the discharge of large quantities of feces, mucus and gases, and sometimes blood. Colitis can take on an ulcerative nature; in rare cases, perforated peritonitis develops. When the disease worsens, symptoms of intestinal obstruction sometimes appear, which is accompanied by flatulence, vomiting, and severe intoxication.
In cases where the elongation of the intestine is predominantly expressed, in the absence of significant expansion, the symptoms of the disease are manifested by pain. They are sometimes paroxysmal in nature and are accompanied by flatulence and rumbling, sometimes there are signs of partial obstruction. There is also an alternation of diarrhea and constipation. There is usually no chronic intoxication in such cases, and the disease progresses slowly.
Dolihomegacolon. Laboratory tests, especially with severe stasis, reveal an increase in indican in the urine and a slight increase in calcium in the blood.
When examining stool, an increase in organic acids and ammonia is sometimes detected. When examining gastric secretion, a decrease in secretion, signs of hypochilia and even achylia are often revealed.
Significant changes are determined by x-ray examination. It is advisable to carry it out by introducing a contrast mass both through the mouth and through the rectum. This is necessary due to the fact that research by introducing barium through the mouth does not always provide the opportunity for topical diagnosis of changes in the colon.
When preparing barium suspension, it is not recommended to use ordinary water. When studying patients, mainly children, complications are possible. They are manifested by a significant deterioration in the general condition after a contrast enema: convulsions, loss of consciousness, cyanosis, dilated pupils. It has been proven that the serious condition of the children studied is the result of the absorption of a significant amount of hypotonic fluid into the blood. Moreover, swelling of the parenchymal organs and brain occurs (K. Hiatt, 1951).
To avoid these complications, isotonic saline and iso-oncotic protein solutions (7% gelatin solution) should be used for enemas and irrigoscopy. Usually, a 1% solution of table salt is used to obtain a barium suspension (S. Ya. Doletsky). It is also not recommended to tightly fill the large intestine if it is large, since its capacity with megacolon reaches 3-5 liters or more.
Dolihomegacolon. X-ray examination often reveals displacement or compression of the stomach by the dilated intestine.
In most cases, a slowdown in the passage of contrast through the colon is detected. Changes in the latter are manifested by a significant expansion of the entire colon or, most often, the sigmoid. Dilatation of the sigmoid and rectum may be observed. Elongation of the sigmoid and other parts with a more or less pronounced expansion of the lumen is often detected. In such cases, additional intestinal loops are formed, the elongated section forms two parallel segments (double-barrel), which most often occurs when the ascending or descending intestine is lengthened; There is also a garland-like sagging of the transverse intestine. In some cases, the elongation of the intestine is accompanied by its fixation in the area of physiological bends, which leads to the formation of intestinal kinks.
Flow. The symptoms of the disease and the dynamics of its course are very diverse. In congenital forms of megacolon with pronounced gigantism of the colon, symptoms usually appear no later than the first or second year of a child’s life. Dominant symptoms: persistent constipation, foul-smelling stools, bloated abdomen, high diaphragm, severe intoxication. Periodic intensification and weakening of the symptoms of the disease is very typical. In some patients, a fairly rapid progression of the disease is observed, and children die from intoxication, accompanied by drowsiness, cachexia, cerebral phenomena, due to acute obstruction or perforation of ulcerated areas of the intestine. In other cases, the disease develops slowly and is treatable.
Dolihomegacolon. Often, symptoms of dolichomegacolon appear in adulthood.
In such cases, there is sometimes only a significant increase in mild dyspeptic symptoms that were observed in childhood. Sometimes the symptoms of the disease develop after an acute gastrointestinal disease, most often colitis or dysentery, which can be a conditioning factor that reveals a previously hidden pathological condition of the colon.
In some cases, symptoms of dolichomegacolon gradually develop in people suffering from chronic diseases (calculous cholecystitis, peptic ulcer); in severe cases of concomitant diseases, dolichomegacolon progresses. In some cases, when a peptic ulcer or chronic cholecystitis is combined with dolichomegacolon, the clinical picture becomes especially severe; symptoms of colon damage may be dominant.
The prognosis for dolichomegacolon depends on the severity of the clinical picture of the disease and is unfavorable with the rapid development of the disease in early childhood. A more favorable outcome is observed in children with a slow development of symptoms, as well as when the disease occurs at a more mature age. An important role is played by frequent exacerbations and especially severe complications—obstruction and perforation.
The diagnosis is relatively easy in severe clinical forms of the disease and is based on identifying typical signs - persistent constipation, bloating and enlargement of the abdomen.
Dolihomegacolon. X-ray examination is essential, especially in patients with mild symptoms and with the predominant development of dolichocolon.
Treatment depends on the characteristics of pathogenesis, clinical manifestations, severity of the disease, the presence of complications and the age of the patient. Both conservative and surgical treatment are used.
Conservative therapy in some cases gives favorable results and consists of regulating intestinal function, eliminating complications and using restoratives; nutritional therapy is important.
The main focus should be on normal bowel movements. Measures aimed at stimulating peristalsis and pursuing the goal of mechanical movement of feces are shown. This is successfully accomplished, especially in children, through gentle abdominal massage, as well as through therapeutic exercises, especially exercises that help improve the tone of the abdominal muscles and enhance peristalsis. Enemas, both cleansing and siphon, are widely used.
Various formulations of enemas are recommended: 1% solution of table salt, soap, hypertonic, vaseline, chamomile infusion, depending on which of them gives the most favorable effect for a given patient. Sometimes you have to resort to removing hard feces that tightly fill the ampulla of the rectum with your fingers. It is not advisable to prescribe strong laxatives; it is better to use mild laxatives (vaseline, olive, peach oils), which give especially favorable results in children.
Dolihomegacolon. For intestinal sluggishness, food is prescribed that enhances intestinal motility (vegetables, fruits, coarse cereals, honey, prunes, etc.).
In case of complications in the form of colitis, as well as in the predominant processes of irritation of intestinal motor function, the presence of adhesions and other mechanical obstacles, it is advisable to prescribe antispasmodics (papaverine, no-spa, platifillin), light heat (in the form of not very hot heating pads) and predominantly a diet poor in waste and not stimulating peristalsis. In case of increased gas formation, adsorbents (animal charcoal) are prescribed; sometimes lumbar novocaine blockade is effective. The most favorable results are obtained by conservative treatment for dolichocolon with preferential lengthening of the intestine.
In some cases, stretching of the anus is used (L. Ladd, E. Gross) with fingers or using bougies of various diameters. This measure is advisable for isolated high sphincter tone 2-3 times a week for 5-10 minutes.
Surgical treatment is indicated for: progressive development of the disease, lack of effect from conservative treatment, as well as the development of severe complications, especially with obstruction. It should be taken into account that children under 3 years of age do not tolerate intestinal resection well.
Causes
The development of the congenital form of the disease is based on the absence of special ganglion cells in the intestinal wall, which are responsible for conducting nerve impulses through the intestine. As a result of aganglionosis, the muscles of the affected area of the large intestine are unable to contract, that is, there is no peristalsis in these places. Feces reach the affected intestine and cannot pass further. Aganglionosis can be observed only in the area of the anus and sigmoid intestine (in 75% of cases) or spread throughout the entire colon, right up to the colon (about 10% of cases).
The very beginning of the disease lies in the prenatal period of fetal development, when the formation of the nervous system of the large intestine occurs between 5 and 12 weeks. Normally, nerve cells from the head end of the neural tube begin to migrate to the tail. In Hirschsprung's disease this migration does not occur.
There is also a version of a hereditary factor in the development of this pathology, when the disease occurs as a result of gene defects.
Causes of acquired megacolon:
- mechanical obstacle to the path of feces (stenosis, tumor, intestinal kinks, intestinal obstruction, postoperative scars or cicatricial changes that have developed against the background of long-term inflammatory processes in the intestines);
- disruption of the nervous regulation of intestinal function due to diseases of the central nervous system (meningitis, encephalitis) or diseases of the endocrine system (diabetes mellitus, hypothyroidism);
- chronic intestinal infections (amoebiasis, shigellosis, campylobacteriosis);
- severe hypovitaminosis B1;
- abdominal injuries;
- anal canal fistulas.
The idiopathic type of megacolon can be placed in a separate group, when the cause of fecal retention and expansion of the colon is unknown. With this form of the disease, the version of aganglionosis is excluded, since morphological examination of the intestine reveals ganglion cells. There is a version of the development of idiopathic megacolon as a result of a lack of the so-called vasoactive intestinal peptide (VIP), which is responsible for relaxing the internal anal sphincter. Accordingly, with its deficiency, the sphincter does not relax, resulting in fecal retention and expansion of the colon (megacolon).
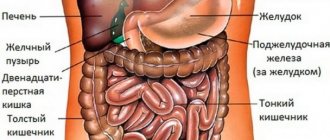
Anatomical and physiological basis of pathology
The large intestine is the final section of the human gastrointestinal tract (GIT), which is almost two meters long and consists of three main parts:
- cecum;
- colon, which is divided into ascending, transverse, descending, sigmoid;
- rectum ending in the anus (back passage).
About 2 liters of mushy contents enter the large intestine from previous sections. Here the process of absorption of water molecules and electrolyte ions occurs, the formation of the final stool from the remains of undigested food and its removal out.
Feces accumulate and are held in the rectum by the sphincter. Receptors from the intestinal walls send signals to the brain; at a certain level of stretching, the sphincter relaxes and feces exit through the anus. Normally, a person has bowel movements every 24-48 hours. Constipation is considered to be more infrequent and difficult bowel movements.
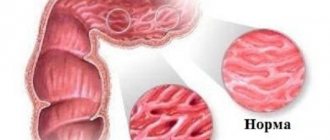
The diameter of this section of the intestine in a healthy person is no more than 8 cm in the ascending colon and 6 cm in the transverse colon. With megacolon, there is a chronic expansion (dilatation) of the lumen and an increase in thickness (hypertrophy) of the intestinal mucosa and all other layers of the wall (muscle, connective tissue). This situation leads to impaired motor function, the development of constant flatulence, abdominal pain and stool retention.
Congenital and acquired megacolon are characterized by persistent constipation. Defecation occurs after 10-14 or more days with the release of solid feces, the volume of which significantly exceeds their amount in a healthy person.
Symptoms and signs
In adults, an asymptomatic course of the pathology may be observed. For example, when a patient has mild congenital aganglionosis, it may not lead to megacolon and may not manifest itself in any way during life. But if the existing aganglionosis is layered with provoking factors in the form of alcohol, smoking, abuse of spicy or fried foods, constipation, then megacolon is more likely to develop and the symptoms described below will appear.
Differences in the manifestations of congenital and acquired forms of the disease - table
| Symptoms of the disease | In children (using the example of Hirschsprung's disease) | In adults (using the example of the acquired form of megacolon) |
| Constipation | Observed from the first days of life, the child cannot empty himself without using a gas tube or an enema. After bowel movements, the stool has a putrid odor and may contain mucus or blood. | Constipation is intermittent. May alternate with periods of spontaneous bowel movement. |
| Flatulence | Occurs in children older than one year. Accompanied by pain and an increase in the size of the abdomen. The symptoms do not improve even after a bowel movement. | Flatulence and abdominal pain intensify only against the background of constipation. After a bowel movement, bloating and pain decrease or disappear completely until the next episode of constipation. |
| Fecal intoxication (nausea, loss of appetite, weight loss) | Vividly expressed from the first days of life. The newborn is not gaining weight well and refuses to eat. With age, such children experience a lag in physical development (thin limbs, but a large protruding belly). The abdominal wall stretches so much that it becomes thinner, and intestinal peristalsis can be visible through it. | These symptoms appear to a significant extent only with persistent constipation. With periodic constipation, these symptoms are practically absent. A decrease in body weight is observed in patients with severe disease. |
| Manifestations from the bronchopulmonary and cardiovascular systems (cyanosis, shortness of breath, frequent bronchitis and pneumonia, tachycardia, heart pain) | These symptoms develop as a result of the displacement of the chest by an enlarged abdomen. Occurs in children older than one year with a progressive course of the disease. The chest takes on the shape of a barrel. | These symptoms more often occur with obstructive megacolon, when constipation is pronounced and the abdomen is enlarged. Symptoms from the heart are more pronounced - pressing pain, shortness of breath after exercise, increased heart rate, sometimes even changes in the electrocardiogram. |
| Intestinal obstruction | Intestinal obstruction can develop from the first months of life. It manifests itself in the form of a sharp deterioration in the child’s condition. He becomes restless, constantly cries, and finds no place for himself. Older children may complain of sharp, unbearable abdominal pain. After prolonged retention of stool, vomiting of feces mixed with blood may occur. The condition requires immediate surgical treatment. | Intestinal obstruction can develop with obstructive, toxic or psychogenic megacolon. The latter type involves the entry of a foreign body into the patient’s intestines. Intestinal obstruction in adults begins acutely - with the appearance of sharp abdominal pain, weakness, increased heart rate, and a drop in blood pressure. The abdomen increases in size and takes on an irregular shape. |
Symptoms of pathology in the photo
In children, if untreated, megacolon may increase in size in the abdomen, sometimes peristalsis can be seen through the anterior abdominal wall
Intestinal obstruction due to megacolon is a life-threatening symptom that requires immediate surgical treatment
Enlargement of the colon can affect one of its parts or the entire organ
Operations for megacolon: colectomy
Some types of colectomy
Colectomy - removal of the colon (complete or partial) - is a surgical procedure that in some cases is vital. Surgery for megacolon often ends with a colostomy or ileostomy.
Indications for urgent surgical intervention:
• progression of expansion; • perforation; • bleeding; • increase in symptoms of intoxication.
Most experts recommend colectomy if there is no positive dynamics within 24-72 hours during treatment. The extent of the operation depends on the extent of the pathological process and its location.
Diagnosis of the disease
Diagnosis of megacolon begins with the collection of complaints, anamnesis (history of the occurrence of the disease) and examination of the patient. Accurate determination of the causes of the disease is necessary for successful treatment; for this, the following research methods are used:
- General blood analysis. Allows you to determine the presence of an inflammatory process in the body. The analysis does not show the localization of the inflammatory focus and does not prove its presence in the intestines, but it may lead to a version of the toxic or infectious cause of megacolon. Leukocytosis (increased number of white blood cells) and increased ESR may speak in favor of the latter.
- Analysis of stool for dysbacteriosis and occult blood. The positive results of these studies also indicate the toxic nature of the disease.
- Digital examination of the rectum. With congenital megacolon, an empty ampulla of the organ will appear; the acquired form, on the contrary, is characterized by an ampulla distended by feces.
- X-ray. Examination of the abdomen with megacolon allows one to identify areas of dilated intestine; chest x-ray reveals an upward displacement of the heart and a high diaphragmatic dome.
X-ray examination reveals areas of expansion of the colon
- Irrigographic research. This is a type of x-ray using a contrast agent injected into the intestines. Areas of narrowed intestine with expansion of its overlying sections will speak in favor of megacolon. The contour of the dilated intestine will be smoothed out, and there will be no natural folds in it.
- Colonoscopic examination. Visual inspection of the inner surface of the intestine using a special apparatus. With megacolon, areas of expansion or pockets of inflammation will be observed (in the case of toxic megacolon). During a colonoscopy, a biopsy (removal of part of the intestinal tissue) can be performed. A biopsy reveals the presence of ganglion cells; in their absence, a diagnosis of congenital megacolon - Hirschsprung's disease - is made.
- Anorectal manometry. Determining the presence or absence of a rectal reflex. In the congenital form of the disease it will be absent.
Diagnostic measures are carried out selectively, according to indications. If Hirschsprung's disease is detected by colonoscopy and biopsy, other studies may not be performed to confirm the diagnosis. Treatment of megacolon
Treatment of congenital megacolon (Hirschsprung's disease) with conservative methods is ineffective; only complete removal of the affected intestine provides a therapeutic effect. Therapeutic measures for secondary (acquired) megacolon are aimed at eliminating the cause that led to the disease. In addition, the patient is recommended to change his lifestyle and diet, whether he wants it or not.
Diet
Therapeutic nutrition for megacolon is aimed at preventing constipation, so the patient is recommended meals containing large amounts of plant fiber, as well as fermented milk products. Foods that cause fermentation and rotting in the intestines should be excluded from the diet. The patient should drink liquid at the rate of 30 ml per kg of body weight per day.
Products and dishes recommended for megacolon:
- first courses daily - soups with vegetable and mushroom broths. Meat and fish broths are prepared from lean meat;
- meat dishes from lean varieties (veal, skinless chicken, beef, rabbit, turkey). It is recommended to consume the meat boiled, steamed or baked. Fried meat is possible, but without crust;
- fresh vegetables and herbs (zucchini, beets, carrots, tomatoes, potatoes, pumpkin, parsley, celery, lettuce). Legumes and cabbage can be consumed if these foods do not cause severe flatulence;
- fresh and dried fruits (apricot or dried apricots, peach, plum or prune, raisins, apples, kiwi, dates);
- milk and fermented milk products (ryazhenka, yoghurts with added fruit, kefir);
- natural juices from fruits or vegetables (apricot, plum, peach, beetroot, pumpkin, carrot);
- cereals and porridges made from them (oatmeal daily, buckwheat and rice 1-2 times a week);
- wholemeal bread;
- butter and vegetable oils (olive, sunflower).
Foods and dishes prohibited for megacolon:
- soups and borscht in broths made from fatty meats and fish (lamb, duck, goose, salmon, salmon);
- smoked meat and fish;
- legumes (beans, peas, lentils). Vegetables: radish, radish;
- rice, corn and millet porridge;
- hard-boiled eggs;
- canned fish and meat;
- baked goods and pastries, fresh white bread;
- hard cheese;
- strong tea, coffee, chocolate;
- spices and seasonings.
Photo gallery: basic nutrition during illness
Natural juices are an excellent source of vitamins and nutrients, and for megacolon they also prevent constipation.
Treatment and prevention of constipation with megacolon will be the addition of vegetables and fruits to the diet.
To avoid constipation, eat oatmeal with yogurt or fruit for breakfast.
A properly composed menu will relieve constipation and prevent complications of megacolon
Medicines
Depending on the type of megacolon and the symptoms experienced by the patient, drug treatment is prescribed. Medicines have only a symptomatic effect, but do not remove the cause of the disease.
Drugs used for symptomatic treatment of megacolon - table
| Group of drugs | Medicine | Release form of the drug | For what purpose are drugs prescribed? |
| Antibacterial agents | Flemoxin solutab (penicillin group) | Water soluble tablets | Prescribed for the toxic form of megacolon, when an infectious cause is confirmed. The choice of drug is made after conducting a diagnostic culture of stool, determining the type of bacteria and their sensitivity to the antibiotic. If treatment requires immediate medication and there is no time to wait for test results, then broad-spectrum antibiotics are prescribed. |
| Sumamed (group of macrolides) | Oral suspension, tablets | ||
| Amikacin (aminoglycoside group) | Solution for parenteral (intramuscular) administration | ||
| Nifuroxazide (nitrofuran group) | Oral suspension, tablets | ||
| Probiotics | Linex | Capsules | Prescribed when dysbacteriosis is detected against the background of toxic megacolon. |
| Enterogermina | Suspension for oral administration | ||
| Carminatives | Espumisan | Oral drops, tablets | Prescribed for severe flatulence to reduce the amount of gas in the intestines |
| Meteospasmil | Capsules | ||
| Enzyme preparations | Panzinorm | Pills | Prescribed for enzymatic insufficiency of the pancreas, when food is not completely broken down and is excreted in the feces in the form of undigested pieces. |
| Pangrol | Capsules | ||
| Mezim | Pills |
It is important to remember that the use of laxatives during megacolon is contraindicated; they can lead to complications such as intestinal atony and intestinal obstruction.
Therapeutic exercise for intestinal diseases
An important aspect for normal bowel function is strengthening the muscles of the anterior abdominal wall. To do this, use a set of the following exercises:
- Breathing exercises. Lying on your back, placing one hand on your stomach, exhale forcefully, pushing out the air with your hand. Then relax and take a passive breath without straining. Repeat the exercise in 2 sets of 4-5 times, daily. This exercise also helps to relax the diaphragm and increase the volume of the chest.
- Fixing the position. Lying on your back, place your hands on the back of your head. Raising your head and legs above the floor, maintain the position for as long as possible.
- Exercise "Bicycle". Lying on your back, make movements with your legs, as if riding a bicycle.
- Exercise "Birch". Lying on your back, raise your legs at right angles to the floor, then lower them to your head and touch the floor. Repeat 4-5 times.
- Exercise "Twisting". Sitting on the floor, raise your arms parallel to the floor. Make turns to the sides 4-5 times, while pulling your legs in the opposite direction.
Therapeutic exercise strengthens the muscles of the abdominal wall and improves intestinal motility
Additional conservative methods
- Carrying out cleansing enemas (hypertonic, vaseline). This type of treatment is prescribed according to strict indications only by a doctor; you cannot do cleansing enemas for megacolon on your own!
- Abdominal massage is performed to stimulate intestinal motility and enhance peristalsis. This promotes spontaneous emptying of the organ. It is recommended to massage the abdomen daily 10–15 minutes before meals. The patient is placed on his back, stroking movements are made in a clockwise direction, that is, in the same way as feces move in the intestines. After stroking, you can begin rubbing and kneading manipulations. Vibration massage on the stomach is not used.
- Electrical stimulation is a method of physiotherapeutic treatment based on the impact of low-frequency waves on the affected area of the intestine, which leads to increased peristalsis in this area.
Operation
With secondary megacolon, surgical treatment is resorted to only if there is no effect from conservative methods. In the case of obstructive megacolon, the cause of the obstruction is removed—scarring changes in the intestine, adhesions, and stenoses. With toxic or neurogenic megacolon, it is sometimes necessary to resort to removing a large section of the intestine (rectum, sigmoid and colon), it all depends on how extensive the pathological process is.
Currently, surgeons are making every effort to perform organ-saving surgery with minimal removal of the intestine and preservation of all intestinal functions. But there are cases when the process is too advanced or too extensive, most of the large intestine has to be removed. And then the patient is given a colostomy on the anterior abdominal wall - an opening through which feces are released from the intestines to the outside.
Treatment
Elimination of megacolon is carried out surgically, but in the initial stages and after surgery, a conservative technique is used to maintain the body.
Are radical methods used to eliminate megacolon in children? Indications for surgery depend on the severity of the pathology - surgical intervention is recommended at the age of 2-3 years, but in severe cases of the disease, surgery is prescribed earlier.
Lack of treatment or re-occurrence of colon pathology can cause intestinal perforation, sepsis and severely reversible digestive disorders.
Conservative treatment
Conservative tactics are aimed at maintaining the patient’s normal well-being in the early stages of megacolon. The following methods are used:
- dietary nutrition;
- medications;
- physiotherapy;
- massage;
- electrical stimulation;
- enemas.
For many digestive and bowel problems, diet is the main treatment method. Proper nutrition during megacolon softens stool, which makes defecation easier. Children and adults include the following foods in their diet:
- cereals and dishes made from them: casseroles, porridges;
- dried fruits: prunes, raisins, dried apricots;
- dairy products;
- green tea;
- fruit drinks and compotes;
- Fiber-rich foods: fruits and vegetables.
Excluded from the menu:
- fried and fatty foods;
- legumes: peas, beans;
- sweets;
- canned food;
- spicy and smoked dishes.
Prohibited products in the photo
Canned foods pose a risk to people with megacolon
Sweets have a negative effect on intestinal motility
Fatty and fried foods are a blow to the digestive organs
Legumes increase the inherent flatulence of megacolon
Drug treatment is also aimed at maintaining the patient’s body. The following groups of funds are used:
- enzyme preparations: Pangrol, Festal-P, Creon, Pancreatin, Mezim, Panzinorm;
- medications to improve motor skills: Motilak, Domperidone, Hexal, Motilium;
- antibiotics - if there is a threat of sepsis (blood poisoning) and the presence of infection;
- bacterial preparations - to maintain the balance of intestinal flora, the following are used: Bifidumbacterin, Bifikol Colibacterin.
Under no circumstances should laxatives be used for treatment, as long-term use can lead to the development of intestinal obstruction.
Photo gallery of medicines
Pancreatin improves protein breakdown and normalizes digestion
Bifidumbacterin is necessary to normalize the balance of intestinal microflora
Motilak accelerates bowel movements and eliminates vomiting if it occurs
Mezim replenishes intestinal enzyme deficiency
To strengthen the muscle tissue of the abdominal cavity, physical therapy complexes are used. The classes are prepared together with the doctor, and the patient strictly follows the instructions. The following elements are used:
- abduction of legs to the sides;
- walking with alternately raising the hips;
- walking with body turns;
- flexion and extension of the legs in the knee-elbow position.
Massage is extremely beneficial for megacolon. Massage the abdominal area, starting from the top point and gradually moving down. Perform circular movements clockwise. It is recommended to massage 20 minutes before meals.
Electrical stimulation is associated with the effect of low-frequency current on the affected area. This improves motility and speeds up the excretion of feces.
To facilitate bowel movements, enemas are also used. However, the technique should not be abused. In addition, only a doctor will select the correct way to perform an enema. The following types of enemas are used:
- hypertensive;
- cleansing;
- siphon;
- Vaseline
In addition to the means and methods presented, the doctor may prescribe the use of vegetable oil. This measure speeds up bowel cleansing. Adult patients take 30–40 ml of oil 3 times a day. For children, 1 tbsp is enough. l. vegetable oil once a day.
Operation
Surgical treatment is prescribed in the absence of a positive result from conservative treatment or in the development of severe forms of pathology. They also resort to a surgical method to solve the problem in the congenital form of the disease in children. The earlier the operation is performed, the better, but the optimal period for intervention is the age of 2–3 years. You should not wait until the child turns 10 years old - the pathology is dangerous.
Before the operation, patients undergo preparation. The exception is when emergency intervention is required. The training is aimed at strengthening the abdominal muscles. In addition, enemas and other means of conservative therapy are used. After the enema, a tube is installed to remove gases.
Surgical intervention involves excision of the diseased area of the intestine. Healthy areas are connected to each other. If the patient has an obstructive form, then obstacles to the passage of feces are removed: scars, fistulas, adhesions.
After treatment, restorative therapy is prescribed: medications are used, therapeutic exercises are prescribed, and the diet is adjusted. The patient is registered for 18 months after the operation; monitoring of his condition is required.
In some cases, it is impossible to completely excise the megacolon in one operation. In such situations, a colostomy is installed - an artificial anus, and feces are collected using a stool bag. If the second stage of the operation cannot be performed, the patient lives with the intestine protruded into the side of the peritoneum all his life.
Colostomy is a necessary measure necessary to remove feces
Possible complications
- Intestinal obstruction is the most terrible complication that can lead to the death of the patient. Intestinal obstruction is dangerous because the intestine can burst at any moment, and feces will enter the abdominal cavity, causing severe intoxication and fecal peritonitis. In this case, it is almost impossible to save the patient.
- Dysbacteriosis is a complication of the toxic type of megacolon. It is dangerous because an imbalance in the intestinal microflora and the growth of pathogenic microflora can lead to blood poisoning and death of the patient.
- Enterocolitis is a consequence of toxic megacolon, when a focus of inflammation develops in the intestines.
- Chronic constipation is the absence of independent bowel movements, which can later lead to hemorrhoids.
Intussusception is a complication of megacolon that threatens the patient's life; if left untreated, the intestine can burst and cause peritonitis.
How is the pathology treated?
Treatment of intestinal megacolon is carried out using conservative and surgical methods. The former are contraindicated in cases of Hirschsprung aganglionosis and obstructive coprostasis; only surgery is needed here.
Resection of part of the affected intestine, removal of mechanical obstacles and other types of interventions are performed. With idiopathic and other types of megacolon, conservative methods can lead to a decrease in intestinal diameter. Clinical recommendations are as follows:
- diet - increasing coarse dietary fiber in the diet due to bran, vegetables and fruits;
- development of a reflex to empty the bowel after 2-3 days;
- toxic megacolon requires discontinuation of medications or replacement with others;
- courses of biological products for intestinal microflora;
- rational use of saline laxatives;
- prokinetic agents – cisapride, trimebutine;
- proserin subcutaneously;
- methods of physiotherapy, massage, physical therapy.
All prescriptions are made by a doctor depending on the type, stage of the disease and the characteristics of the patient’s body.
Patient complaints of persistent constipation should always raise red flags regarding megacolon. Prolonged retention of feces can lead to the formation of stones, which can lead to the development of bedsores, ulcers, perforation of the intestinal wall and peritonitis. Therefore, if home methods for treating constipation are not effective, you should consult a doctor to find out the cause and eliminate it.