Pleurisy is one of the common diseases of the human respiratory system. According to medical statistics, it occurs in 10% of patients in therapeutic hospitals. This disease very often accompanies pneumonia (up to 95% of cases), tuberculosis, connective tissue diseases, as well as malignant neoplasms - the incidence of pleurisy in cancer of the lungs, breast, ovaries, and hematopoietic system reaches 50%. The large number of causes that cause this disease, as well as the difficulties encountered in diagnosing the disease, often complicate the treatment of a patient with pleurisy.
Causes
The causes of pleurisy can be divided into infectious and aseptic or inflammatory (non-infectious).
Non-infectious pleurisy usually occurs
- for rheumatoid arthritis,
- with vasculitis (vascular damage),
- for rheumatism,
- with systemic lupus erythematosus,
- with scleroderma,
- as a result of pulmonary embolism and pulmonary edema,
- with pulmonary infarction,
- when metastasis of lung cancer into the pleural cavity,
- with a primary malignant tumor of the pleura – mesothelioma,
- lymphoma,
- during hemorrhagic diathesis (clotting disorders),
- during leukemia,
- with a tumor process of the ovaries, breast cancer as a result of cancer cachexia (terminal stage of cancer),
- with myocardial infarction due to congestion in the pulmonary circulation.
- for acute pancreatitis.
Infectious diseases include:
- syphilitic or tuberculous pleurisy,
- parasitic (echinococcal or amoebic),
- pleurisy in particularly dangerous infections (tularemia, brucellosis, caused by the typhoid microbe or occurring with typhus),
- microbial pleurisy (infection of the pleural cavity with staphylococci, Escherichia coli and Pseudomonas aeruginosa, pneumococci, etc.)
- viral pleurisy (occurring when affected by the influenza virus, herpes),
- fungal pleurisy (damage to the pleura by candidiasis, coccidiosis, blastomycosis),
- pleurisy, which occurs during wounds or operations on the chest, due to microbes entering the pleural cavity.
Causes of pleurisy
Pulmonologists distinguish the causes of pleurisy depending on the form of the disease itself. Pathological inflammation of the pleural lobes has non-infectious and infectious etiologies.
Reasons for the development of non-infectious forms of pleurisy:
- myocardial infarction and pulmonary infarction (therapy by a cardiologist);
- diseases that destroy the connective tissue of the lungs;
- cancer metastases affecting the pleural layers (oncologist consults);
- renal failure.
Non-infectious pleurisy has pronounced symptoms, which allows specialists to make accurate diagnoses, using additional examinations to clarify the degree and type of the disease.
Infectious pleurisy develops for completely different reasons:
- lung tissue is affected by nonspecific bacterial strains, for example, pathogens of syphilis, typhoid, Protea or mycoplasma; and specific microorganisms - pneumococci, tuberculosis bacillus, Haemophilus influenzae and Klebsiella pneumoniae;
- the lungs are attacked by viruses, fungi, blastomycetes, actinomycetes, coccidia, amoebas, echinococci, etc. that are dangerous to the respiratory system.
Any of the pathogenic microorganisms can enter the pleural tissue in several ways:
- through the bloodstream;
- through the lymph circulation system;
- with chest trauma;
- due to contact between the lung and pleura.
The infectious form of pleurisy can be contagious (with tuberculous or fungal pleurisy), in which case the patient is isolated from others. This disease is characterized by paroxysmal pain in the chest on the affected side, often in the lower parts, aggravated by breathing movements and coughing, which can only be relieved with anesthetic drugs.
In both acute and chronic pleurisy, the causes of development are almost identical. But fluid accumulates in the pleural cavity only with the exudative type of inflammation.
Classification
In clinical practice, it is customary to distinguish several types of pleurisy, which differ in the nature of the effusion formed in the pleural cavity and, accordingly, in the main clinical manifestations.
- Dry (fibrinous) pleurisy . Develops at the initial stage of inflammatory damage to the pleura. Often, at this stage of pathology, there are still no infectious agents in the lung cavity, and the changes that occur are due to the reactive involvement of blood and lymphatic vessels, as well as an allergic component. Due to an increase in vascular permeability under the influence of pro-inflammatory substances, the liquid component of plasma and some proteins begin to leak into the pleural cavity, among which fibrin is of greatest importance. Under the influence of the environment in the inflammatory focus, fibrin molecules begin to unite and form strong and adhesive threads that are deposited on the surface of the serous membrane.
- Purulent pleurisy . Purulent exudate accumulates between the layers of the serous membrane of the lung. This pathology is extremely severe and is associated with intoxication of the body. Without proper treatment, it poses a threat to the patient's life. Purulent pleurisy can form either due to direct damage to the pleura by infectious agents, or due to the spontaneous opening of an abscess (or other accumulation of pus) of the lung into the pleural cavity. Empyema usually develops in debilitated patients who have serious damage to other organs or systems, as well as in people with reduced immunity.
- Exudative (effusion) pleurisy . It represents the next phase of the development of the disease after dry pleurisy. At this stage, the inflammatory reaction progresses, and the area of the affected serous membrane increases. The activity of enzymes that break down fibrin threads decreases, and pleural pockets begin to form, in which pus can subsequently accumulate. The outflow of lymph is disrupted, which, against the background of increased fluid secretion (filtration from dilated blood vessels at the site of inflammation), leads to an increase in the volume of intrapleural effusion. This effusion compresses the lower segments of the lung on the affected side, which leads to a decrease in its vital volume. As a result, with massive exudative pleurisy, respiratory failure may develop - a condition that poses an immediate threat to the patient’s life. Since the fluid accumulated in the pleural cavity reduces to some extent the friction between the layers of the pleura, at this stage the irritation of the serous membranes and, accordingly, the intensity of the pain is somewhat reduced.
- Tuberculous pleurisy . It is often placed in a separate category due to the fact that this disease is quite common in medical practice. Tuberculous pleurisy is characterized by a slow, chronic course with the development of a syndrome of general intoxication and signs of damage to the lungs (in rare cases, other organs). The effusion from tuberculous pleurisy contains a large number of lymphocytes. In some cases, this disease is accompanied by the formation of fibrinous pleurisy. When the bronchi melt by an infectious focus in the lungs, specific curdled pus, characteristic of this pathology, can enter the pleural cavity.
This division in most cases is rather arbitrary, since one type of pleurisy can often transform into another. Moreover, dry and exudative (effusion) pleurisy are considered by most pulmonologists as different stages of one pathological process. It is believed that dry pleurisy initially forms, and effusion develops only with further progression of the inflammatory reaction.
Complications
Fluid accumulated in the pleural cavity, especially in large quantities, can lead to many complications. This may be acute pulmonary failure, inflammation and infection of pulmonary origin, problems with the function of the liver, heart and other internal organs.
Since fluid and pus have a high probability of spreading into the abdominal cavity, complications from the gastrointestinal tract should be expected. This type of effusion, accumulated in the pleural area, is a factor that often leads to death or disability. This concerns the need to resect part of the pancreas or spleen.
Such complications can occur in both men and women of any age, so treatment should begin as early as possible and preventive measures should be used.
Symptoms
The clinical picture of pleurisy is divided into dry and exudative.
Symptoms of exudative pleurisy:
- general malaise, lethargy, low-grade fever;
- chest pain, shortness of breath intensify, a gradual increase in fever - this happens due to the collapse of the lung, the mediastinal organs are compressed.
Acute serous pleurisy usually has a tuberculous origin and is characterized by three stages:
- In the initial period (exudative), smoothing or even bulging of the intercostal space is noted. The mediastinal organs are shifted to the healthy side under the influence of a large amount of fluid in the pleural fissure.
- The stabilization period is characterized by a decrease in acute symptoms: the temperature drops, chest pain and shortness of breath disappear. At this stage, pleural friction may appear. In the acute phase, a blood test shows a large accumulation of leukocytes, which gradually returns to normal.
- It often happens that fluid accumulates above the diaphragm, so it is not visible with a vertical x-ray. In this case, it is necessary to conduct the study in a lateral position. Free fluid moves easily in accordance with the position of the patient's torso. Often its accumulations are concentrated in the cracks between the lobes, as well as in the area of the diaphragm dome.
Symptoms of dry pleurisy:
- chest pain;
- general unhealthy condition;
- dry cough;
- low-grade body temperature;
- local pain (depending on the location of the lesion);
- When palpating the ribs, deep breathing, and coughing, the pain intensifies.
In the acute course of the disease, the doctor diagnoses pleural noise by auscultation, which does not stop after pressing with a stethoscope or coughing. Dry pleurisy, as a rule, goes away without any negative consequences - of course, with an adequate treatment algorithm.
Acute symptoms, in addition to the described serous pleurisy, include purulent forms - pneumothorax and pleural empyema. They can be caused by tuberculosis and other infections.
Purulent pleurisy is caused by pus entering the pleural cavity, where it tends to accumulate. It should be taken into account that non-tuberculous empyema can be treated relatively well, but with an inadequate algorithm of action it can develop into a more complex form. Tuberculous empyema is severe and can be chronic. The patient loses significant weight, suffocates, experiences constant chills, and suffers from coughing attacks. In addition, the chronic form of this type of pleurisy causes amyloidosis of internal organs.
If optimal care is not provided, complications arise:
- respiratory arrest;
- spread of infection throughout the body through the bloodstream;
- development of purulent mediastinitis.
Diagnosis of pulmonary pleurisy
The therapist will be able to establish the correct medical history by listening to breathing for the presence of wheezing, as well as examining the area of the sternum and determining its enlargement.
To identify the inflammatory process, it is necessary to take a urine and blood test.
The accuracy of the diagnosis will also depend on radiography and fluorography.
After diagnosing pleurisy, fluid is collected from the pleural area to determine the type of disease.
More often, effusion or purulent discharge is found in the fluid, more rarely bloody.
- Childhood pleurisy is basically purulent.
Much less often, an oncological disease or lung cancer can be diagnosed, but this is a rather rare and extreme case in which a sample of lung tissue is removed.
Important! Pleurisy is a contagious form of the disease, regardless of the fact that it is secondary and is usually a consequence of some infectious disease.
If pleurisy is detected, you need to minimize contact with others, and if you are in public places, you must wear a gauze bandage, which will reduce the risk of infecting others.
The disease is spread by airborne droplets.
The tuberculous type of pleurisy is the most dangerous of all forms, because the course of the disease is practically asymptomatic.
Diagnostics
The primary task in diagnosing pleurisy is to determine the location and cause of the inflammation or tumor. To make a diagnosis, the doctor studies the medical history in detail and conducts an initial examination of the patient.
Basic methods for diagnosing pulmonary pleurisy:
- Blood tests can help determine whether you have an infection, which may be the cause of pleurisy. In addition, blood tests will show the state of the immune system.
- A chest x-ray will determine if there is any inflammation of the lungs. A chest x-ray may also be taken with the patient lying down, which will allow the free fluid in the lungs to form a layer. A supine chest x-ray should confirm whether there is any fluid buildup.
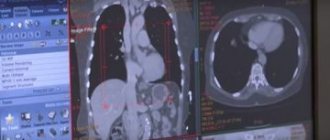
- A computed tomography scan is performed if any abnormalities are found on a chest x-ray. This analysis presents a series of detailed, cross-sectional images of the chest. The images produced by a CT scan create a detailed picture of the inside of the breast, allowing your doctor to get a more detailed analysis of the irritated tissue.
- During a thoracentesis, the doctor will insert a needle into the chest area to test for fluid. The fluid is then removed and analyzed for infections. Due to its invasive nature and associated risks, this test is rarely done for a typical case of pleurisy.
- During a thoracoscopy, a small incision is made in the chest wall and a tiny camera attached to a tube is then inserted into the chest cavity. The camera locates the irritated area so a tissue sample can be taken for analysis.
- A biopsy is useful in the development of pleurisy in oncology. In this case, sterile procedures are used and small incisions are made in the skin of the chest wall. An X-ray or CT scan can confirm the exact location of the biopsy. A doctor may use these procedures to insert a lung biopsy needle between the ribs and into the lung. A small sample of lung tissue is then taken and the needle is removed. The tissue is sent to a laboratory where it will be analyzed for infections and abnormal cells consistent with cancer.
- Using ultrasound, high-frequency sound waves create an image of the inside of the chest cavity, which will allow you to see if there is any inflammation or fluid build-up.
As soon as the symptoms of pleurisy are identified, treatment is prescribed immediately. The first place in treatment is antibiotics against infection. In addition to this, anti-inflammatory drugs or other painkillers are prescribed. Sometimes cough medicine is prescribed.
The structure of the pleural fissures
The pleura is the serous membrane of the lung. There are 2 types of pleura:
- Visceral - the membrane that covers the lung.
- Parietal is a membrane that covers the chest cavity.
Pleural cavity
The gap that is located between the visceral and parietal membranes, filled with fluid, is the pleural region.
The visceral membrane envelops the lung and penetrates into every gap between the pulmonary segments. At the root of the lung, the visceral membrane passes into the parietal membrane. And under the root, where the sheets of the pleura are connected, the pulmonary ligament is formed.
The parietal membrane covers the inner surface of the chest, and in the lower part it connects with the pulmonary pleura.
There are 3 types of parietal pleura:
Costal pleura is a membrane that lines the ribs and intercostal spaces.
- Mediastinal (mediastinal) - the pleura that covers the organs of the mediastinum.
- Diaphragm - a film that lines the top of the diaphragm, except for its central sections.
The dome of the pleura is the upper section, located where the costal pleura passes into the mediastinal pleura. The dome is located over the first rib and collarbone.
The pleural cavity is a narrow gap between the parietal and pulmonary pleura, which has negative pressure. The slit-like space is filled with 2 ml of serum fluid, which lubricates the pulmonary and parietal membranes and minimizes friction between them. With the help of this liquid, 2 surfaces adhere.
When the respiratory muscles contract, the chest expands. The parietal membrane moves away from the pulmonary membrane and pulls it along with it, as a result, the lung stretches.
With a penetrating chest injury, intrapleural and atmospheric pressure is equalized. The pleural cavity fills with air, which penetrates through the hole, as a result the lung tissue collapses and the organ ceases to function.
Pleura
Pleural sinuses are depressions in the pleural space, which are located at the point of transition of parts of the parietal membrane into each other.
There are 3 sines:
- Costophrenic formed in the area where the costal membrane passes into the diaphragmatic membrane.
- The phrenic-mediastinal sinus is the least pronounced sinus, which is located where the mediastinal pleura passes into the phrenic pleura.
- Costomediastinal - located in the area where the costal membrane passes into the mediastinal membrane on the left side.
Thus, the pleural sinuses are areas that are located between the two parietal sheets of the pleura. When the membrane becomes inflamed, pus may form in the pleural pockets.
The anterior border of the pleural membrane (on the right side) begins from its upper part, passes the sternoclavicular joint, the middle of the half-joint of the manubrium of the sternum. It then crosses the posterior part of the body of the sternum, the cartilage of the 6th rib and descends to the lower limit of the pleura. This boundary of the shell corresponds to the limits of the lung.
Sinuses
The lower border of the pleural membrane is located below the limit of the lung. This line coincides with the area where the costal membrane passes into the diaphragmatic membrane. Since the lower limit of the left lung is located 2 cm lower than that of the right, the limit of the pleura on the left side is slightly lower than on the right.
The posterior limit of the pleura on the right side is located opposite the head of the 12th rib, the posterior border of the membrane and the lungs coincide.
Treatment of pleurisy
Effective treatment of pleurisy depends entirely on the cause of its occurrence and consists mainly in eliminating the unpleasant symptoms of the disease and improving the patient’s well-being. In case of a combination of pneumonia and pleurisy, treatment with antibiotics is indicated. Pleurisy, which accompanies systemic vasculitis, rheumatism, scleroderma, is treated with glucocorticoid drugs.
Pleurisy that occurs against the background of tuberculosis is treated with isoniazid, rifampicin, and streptomycin. Typically, such treatment lasts for several months. In all cases of the disease, diuretic, painkillers and cardiovascular drugs are prescribed. For patients who do not have any special contraindications, physical therapy and physiotherapy are indicated. Often, in the treatment of pleurisy, in order to prevent relapses of the disease, obliteration of the pleural cavity or pleurodesis is performed - the introduction of special “gluing” preparations into the pleural cavity.
The patient is prescribed analgesics, anti-inflammatory drugs, antibiotics, and drugs to combat cough and allergic manifestations. For tuberculous pleurisy, specific therapy with anti-tuberculosis drugs is carried out. For pleurisy resulting from a tumor of the lung or intrathoracic lymph nodes, chemotherapy is prescribed. Glucocorticosteroids are used for collagen diseases. If there is a large amount of fluid in the pleural cavity, a puncture is indicated to suction out the contents and administer medications directly into the cavity.
During the rehabilitation period, breathing exercises, physiotherapeutic treatment, and restorative therapy are prescribed.
Types of pleurisy and causes of the disease
In medicine, pleural effusion is divided into two types - transudate and exudate. This helps determine the cause of the increased effusion. If excess fluid accumulates as a result of changes in capillary blood pressure, then they speak of a transudate; in case of blockage of lymphatic vessels or increased vascular permeability - about exudate.
The causes of transudate may be:
- Heart failure and inflammation of the serous membrane of the heart (pericarditis).
- Cirrhosis of the liver.
- Kidney diseases accompanied by edema.
- Blockage of the urinary tract.
- Diseases of the thyroid gland leading to edema.
- Medical manipulations in the abdominal and thoracic cavity: purification of blood from toxins (peritoneal dialysis through a catheter), heart surgery; bone marrow transplant operations.
- Low level of albumin in the blood.
- Blood clots in the pulmonary artery, blockage of the superior vena cava.
Reasons for the accumulation of exudate in the pleural cavity:
- Related to internal diseases:
- cancerous tumors;
- infectious infections (tuberculosis, viral, fungal, parasitic and bacterial infections);
- gastrointestinal diseases : hernias, esophageal perforation, pancreatitis; as well as surgical interventions for the treatment of these diseases;
- connective tissue diseases : rheumatism, rheumatoid arthritis, systemic lupus erythematosus, scleroderma, leading to impaired blood supply to the organs of the human body.
- Arising from external influences:
- taking provoking drugs (amiodarone, nitrofurantoin, phenytoin, methotrexate, carbamazepine, procainamide, propylthiouracil, penicillamine, cyclosporine, bromocriptine);
- radiation therapy;
- injuries of various types : as a result of mechanical damage to the chest, burns, chemical exposure, electric shock.
According to the degree of localization of the lesion, diffuse (general) and encysted pleurisy are distinguished. In the latter case, fluid accumulation occurs in local areas, between the pleural adhesions. Adhesive isolated cavities arise as a result of a long-term inflammatory process in the pleural area.
Prevention
Of course, it is impossible to predict how the body will react to the action of a particular factor. However, anyone can follow simple recommendations for the prevention of pleurisy:
- First of all, complications should not be allowed during the development of acute respiratory infections. To prevent pathogenic microflora from penetrating the mucous membrane of the respiratory tract, and then into the pleural cavity, colds cannot be left to chance!
- For frequent respiratory tract infections, it is good to change the climate for a while. Sea air is an excellent means of preventing respiratory tract infections, including pleurisy.
- If pneumonia is suspected, it is better to take a chest x-ray in a timely manner and begin adequate therapy. Improper treatment of the disease increases the risk of complications in the form of inflammation of the pleura.
- Try to strengthen your immune system. In the warm season, do hardening, spend more time in the fresh air.
- Stop smoking. Nicotine becomes the first cause of the development of pulmonary tuberculosis, which in turn can provoke inflammation of the pleura.
- Do breathing exercises. A couple of deep breaths after waking up will serve as an excellent prevention of the development of inflammatory diseases of the respiratory system.
Types of pulmonary pleurisy
There are two types of this disease:
- exudative pleurisy - the human body cannot independently remove accumulated fluid from the lungs;
- fibrous pleurisy - when fluid is removed from the body, plaque remains on both layers of the pleura.
Both types of pleurisy are extremely dangerous; treating this disease at home is not recommended.
If this disease is detected in a timely manner, it can be cured quite quickly and without consequences, but only under the supervision of a specialist!
Forecast
The prognosis for pleurisy is favorable, although it directly depends on the underlying disease. Inflammatory, infectious, post-traumatic pleurisy can be successfully cured and does not affect the quality of future life. Unless, during the rest of your life, pleural adhesions will be noted on radiographs.
The exception is dry tuberculous pleurisy, as a result of which fibrous deposits can calcify over time, forming the so-called armored pleurisy. The lung becomes encased in a “stone shell,” which interferes with its full functioning and leads to chronic respiratory failure.
To prevent the formation of adhesions that form after removal of fluid from the pleural cavity, after treatment, when the acute period subsides, the patient should undergo rehabilitation procedures - this is physiotherapy, manual and vibration massage, daily breathing exercises are required (according to Strelnikova, using a Frolov breathing simulator) .
Causes of hydrothorax
Fluid in the pleural cavity is always a sign and complication of any disease. Hydrothorax does not occur on its own.
Reasons for the development of hydrothorax:
- Cardiovascular failure. In chronic cardiovascular failure due to pericarditis or heart disease, pleural fluid fills the lung cavity gradually. In case of acute development of pathology, urgent pumping is necessary due to the risk of suffocation.
- Severe pathology of the kidneys. Hydrothorax in this case appears in renal failure due to impaired renal function due to a serious illness. Most often this is glomerulonephritis with nephrotic syndrome. In this case, fluid fills both lungs.
- Cirrhosis of the liver. With cirrhosis of the liver, fluid does not always fill the lungs, but only in 1 case out of 10. Hydrothorax with cirrhosis is right-sided. It develops when fluid from the abdominal cavity enters the pleural cavity through an opening in the diaphragm. Fluid can also enter the lungs during dialysis.
- The appearance of a tumor in the mediastinum. The mediastinum refers to the space between the lungs. The appearance of malignant neoplasms in this place is rare, but one of their symptoms may be the formation of fluid in the lungs. The tumor gradually leads to the disruption of normal blood flow and the outflow of lymph, which provokes the accumulation of fluid in the lungs.
- Pneumonia. Most diseases of the respiratory system do not provoke an imbalance of pressure between the blood plasma and hydrostatic pressure in the capillaries. Fluid in the lungs with pneumonia appears only when the disease is complicated or in case of long-term absence of treatment.
- Anemia and lack of vitamins B and C.
Treatment
Treatment of pleurisy in elderly people is carried out in a hospital setting. It is aimed at eliminating the cause of the disease, stabilizing the patient and normalizing respiratory functions.
Complex therapy for pleurisy is carried out:
- drug treatment;
- physiotherapy;
- physiotherapy;
- diet.
If there is profuse effusion, it is evacuated using drainage or pleural puncture. A specialist will talk about the thoracentesis procedure in the video in this article.
Medication
Drug therapy for pleurisy in old age is carried out with the same drugs as for other people. However, when prescribing them, the characteristics of an elderly organism and the course of the disease should be taken into account.
Table. Medicines for the treatment of pleurisy.
| Group of drugs | Indications | Instructions for use |
| Antibiotics - Ceftriaxone, Levofloxacin | If pleurisy is caused by microbial flora | Intramuscularly, the course of treatment is determined by the severity of the condition |
| NSAIDs - Ibuprofen, Diclofenac | Severe pain syndrome | Take a tablet orally for pain |
| Antiarrhythmic drugs | Development of heart rhythm disturbances against the background of pleurisy | As prescribed by a doctor |
| Vitamins | Stimulation of the body's defenses | One tablet a day |
The dosage of some drugs (antibiotics, NSAIDs) must be reduced by one third from the standard. This is due to a decrease in metabolism in an elderly person and a slower elimination of the drug from the body.
Diseases in the elderly are characterized by a long, protracted course, so the course of treatment must be extended by 2-3 days more than the standard one.
Folk remedies
Older people are accustomed to trusting a variety of traditional medicine. And not without reason. In combination with traditional therapy, folk recipes proven over the years bring good results.
- Onion juice. Squeeze the juice from a small onion. Add a spoonful of liquid honey and mix. Take 20 ml before meals.
- Infusion of horsetail. Pour 20 grams of dry herb into 500 ml of boiling water, leave for 4 hours and strain. Drink 50 ml before meals.
- A mixture of horseradish root and lemon juice. Wash and peel a small horseradish root thoroughly. Grate and mix with the juice of half a lemon. Take the mixture one teaspoon 2 times a day.
- Badger fat rub. Mix 300 grams of badger fat with the same amount of crushed aloe leaves and a glass of honey. Place in a low-heat oven for half an hour. Cool and rub the chest and back area before going to bed.
Home remedies effectively complement traditional pleurisy therapy
Treatment of pleural adhesions in the lungs
The high prevalence of pulmonary diseases is explained by the fact that they usually accompany seasonal viral diseases. It’s rare that someone manages to avoid getting sick with acute respiratory infections or the flu at least once a year. As a result, pleural adhesions can form in the lungs, which negatively affect the functioning of the entire body.
In order not to start the disease, you need to consult a doctor in time, who will make a diagnosis and prescribe treatment.
Causes of the disease
Adhesions form in the pleural cavity, which is located between the membranes that cover the inside of the chest and the outside of the lungs. This shell is a smooth surface with a large number of nerve endings. It is filled with fluid that is secreted on the surface of the pleura covering the chest, after which it is absorbed through the membrane adjacent to the lungs.
The causes leading to pleural disease are very diverse. Inflammatory processes occurring in the body can lead to an increase in the amount of fluid produced. In this case, a protein is released that settles on the surface of the pleura, making it rough. When breathing deeply, the surfaces rub, irritating the nerve endings, which leads to coughing and pain in the sides of the chest. Such symptoms are characteristic of a disease such as pleurisy.
Sometimes the excess fluid in the pleural cavity reaches one and a half liters. This increase occurs when the lining of the lung is damaged and fluid is not absorbed.
This can cause the lung to compress, causing the person to feel short of breath, making it difficult to breathe and causing heaviness in the sides. Such symptoms most often accompany kidney disease or heart failure; this picture is also possible with the development of tuberculosis or a tumor.
There are cases when adhesions form in large numbers, and the free space decreases. This also leads to decreased mobility of the membranes, which contributes to severe shortness of breath and difficulty breathing. In such cases, urgent treatment is necessary.
Adhesions in the lungs
They are formed anywhere due to the presence of connective tissue. Many organs of the human body are susceptible to the formation of adhesions.
In the pleura, adhesions are connective tissue growing between the linings of the lung and chest.
They can have a single structure, or they can grow so much that they ultimately occupy the entire pleural cavity. In this case, emergency medical care is needed.
Symptoms that occur when there are adhesions in the pleural cavity:
As a rule, the formation of adhesions is preceded by previous pulmonary diseases, which serve as an impetus for their development. There are main diseases that are the root cause of the formation of adhesions:
- pneumonia,
- bronchitis,
- tuberculosis,
- lungs' cancer,
- pleurisy,
- pneumonia,
- lung infection
In small quantities, adhesions are not dangerous, but viral diseases that provoke their development and increase in number must be avoided. Which can ultimately lead to pulmonary failure.
As they grow, adhesions can reduce blood circulation in the lungs, blocking blood vessels and bronchi. Blockage of the bronchi leads to a decrease in oxygen levels in the blood. In adhesions with prolonged development, the formation of their own vessels and nerves is possible.
Pleurocostal adhesions mainly form after fibrinous or purulent pleurisy, and they develop very quickly. The resulting thickenings of the pleura mainly occur in the lateral sections, on the walls, towards the surface of the ribs of the lung.
Diagnostics and treatment measures
Fluorography is primarily used to detect pulmonary diseases. This procedure must be carried out annually; it is mainly aimed at identifying the early stage of tuberculosis. However, an experienced radiologist can identify formed pleural adhesions in the image, which appear as shadows. Moreover, their shape does not change depending on inhalation and exhalation.
If necessary, an additional x-ray is prescribed. As a rule, adhesions are located in the lower part of the lung. In this case, there will be a darker picture, and there may also be partial deformation of the chest and diaphragm.
When diagnosing pleural adhesions, further treatment depends on their number and stage of development. As a rule, therapeutic effects accompanied by physiotherapy are sufficient.
In case of exacerbation of inflammatory processes in the lungs, which lead to the formation of adhesions, it is necessary, first of all, to localize them. For this purpose, antibiotics are used, which are administered intravenously or intramuscularly. As a rule, such processes are accompanied by a cough, so medications that improve sputum discharge are needed.
After the inflammation has been stopped, inhalations and electrophoresis can begin. Also, when pleural adhesions form, breathing exercises and chest massage have worked well.
It is important to note that proper nutrition plays an important role in pulmonary diseases.
If the body is predisposed to pulmonary diseases, it is recommended to periodically undergo spa treatment. This will help improve the health of the body. You should also avoid exposing your body to hypothermia, play sports and give up bad habits.
In addition to medications, it is good to use folk remedies when fighting adhesions. They are inexpensive, do not burden the body like medications, and are also very effective. Here are some recipes that will help get rid of adhesions:
Rose hips, nettles and lingonberries are used to make tea.
Course of the disease
In each case, the course of pleurisy occurs differently, depending on the processes occurring in the lungs under the influence of the underlying disease. Most often, it is a complication of pneumonia that affects the respiratory system. However, there are common characteristic features inherent in all forms of pleurisy.
The onset of the inflammatory process is marked by the appearance in the cavity of exudative fluid containing a large amount of fibrin. It is this substance that creates deposits on the surface of the pleura. With a slight accumulation of exudate, such pleurisy is considered dry or fibrinous. If the effusion continues to accumulate, in addition to plaque on the surface, more intense fibrin deposition occurs, leading to thickening of the pleura. Gradually they become connective tissue with varying degrees of density, merging with the pleura located in different parts of the affected organ.
Treatment methods for purulent pleurisy
Successful treatment of purulent pleurisy of the lungs is possible only if measures are taken simultaneously against the primary disease. The main goal of the treatment course is to reduce intoxication, increase the body's immunity, eliminate hypoxemia, and improve the functioning of vital organs.
Conservative treatment consists primarily of antibacterial therapy through punctures. After removing the pus, broad-spectrum antibiotics are introduced into the cavity. The sensitivity of the microflora to these drugs is preliminarily determined.
This treatment gives positive results in approximately 75% of cases. At the same time, detoxification measures and general strengthening therapy are carried out - taking vitamins, glucose, blood and plasma transfusions, high-calorie nutrition, etc. If necessary, cardiac and sedative medications are prescribed.
Surgical treatment of purulent pleurisy is carried out using closed and open methods. The ultimate goal in each case is to remove pus and create a favorable environment for tissue repair. The closed method involves introducing drainage inside and removing pus using a water jet pump and other means. The soft tissue around the drainage is sutured, and the outer end is connected to the equipment.
With the open method, a wide opening of the pleura is performed through the resected rib. After this, a wide drainage device is inserted into the cavity, without connecting to aspiration equipment. In modern conditions, general surgery uses this method very rarely. Each of these methods has its own advantages and disadvantages associated with the effectiveness of evacuation of purulent masses in each specific case.
Treatment in the postoperative period plays an important role. The main measure is to ensure a constant outflow of purulent masses and neutralize possible infections. Measures are being taken to increase the body's resistance and speed up the expansion of the lungs. For this purpose, it is necessary to constantly monitor the drainage and regularly monitor the amount of fluid using x-rays. Evacuation of pus should be as complete as possible. Removal is carried out as slowly as possible, in order to avoid a sharp displacement of the mediastinum and severe disturbances in the basic functions of the heart and breathing.
Features of the treatment of pulmonary pleurisy in the elderly
With pulmonary pleurisy, symptoms and treatment in older people are slightly different from the standard approach to therapy. In addition to drug treatment, older people are advised to stay in bed. Because with age it is much more difficult for the body to recover. Doctors advise not to strain the heart muscles, to avoid stress and anxiety. It is also necessary to adhere to a gentle diet with plenty of useful microelements and vitamins. The basis of nutrition should be vegetables, fruits and cereals.
What is pleurisy
Around the lungs there is a special serous membrane, consisting of 2 lobes: visceral, i.e. internal, and parietal, i.e. outdoor Normally, between these membranes there is a small space filled with liquid, the volume of which does not exceed 25 mm. It acts as a lubricant.
When pulmonary pleurisy develops, this balance is disrupted. Inflammatory damage to the pleural sheets leads to the fact that the fluid ceases to be absorbed into the blood and lymphatic vessels, accumulating between the serous membranes.
Less common is the dry version of the disease, in which the vessels in the pleura affected by the inflammatory process retain functionality and fluid accumulation does not occur. In addition, as a result of inflammation, the pleura swells and becomes rough. When performing breathing movements, friction appears.
What are the symptoms of exudative pleurisy and hydrothorax?
Symptoms increase gradually as more fluid accumulates in the pleural cavity. Shortness of breath occurs, at first only during intense physical activity, but over time it begins to bother you when doing everyday activities, walking, or at rest. The patient begins to get tired faster and often wakes up at night. Often, shortness of breath intensifies when lying down, and when a person stands or sits, he feels better.
The left and right parts of the pleural cavity are separated from each other, most often fluid accumulates on only one side. Such patients often feel better when they lie on the painful side, since this allows the healthy lung to expand better. During the examination, you can notice how the affected half of the chest “lags behind” during breathing. Less commonly, exudative pleurisy is bilateral.
Gradually, a feeling of heaviness and pain in the chest begins to bother me. A persistent cough occurs. It is usually dry, sometimes there is a little phlegm. The patient becomes pale and constantly feels weak. It constantly seems that there is “not enough air”, that the lungs do not fully expand during inhalations. Many patients experience fear and are afraid of suffocating.
Why do pleural deposits appear in the lungs and treatment?
Under what conditions do pleural deposits occur?
These textures are combined and are represented by the action of the pleura during inflammation. They act as insulators for each other's tissues. Usually the layers are stored for a long time even after the patient has been treated. Sometimes they have the potential to produce symptoms such as a mild cough with transient shortness of breath and slight chest pain. Under certain circumstances they become calcified, making them easier to detect.
How is the disease diagnosed?
Pleural layers can be detected by fluorography or x-ray. If they are tiny, fluorography shows a slight darkening of the field on the left of the lungs, and sometimes no darkening of both sides is visible at all. The pleural wall becomes larger and in the image, uneven scattered shadows are noticeable, most intensified in the lateral sections. However, a similar picture can also be observed with scoliosis of the thoracic spine. In this case, checking the pleural layers becomes somewhat more complicated.
When to do treatment
Prevention of deposits
To prevent the formation of these structures in the lower parts, everything initially comes down to early diagnosis of the disease and appropriate treatment, otherwise they may worsen with the formation of an inflammatory course. If necessary, it is necessary to remove blood, air and exudate. Subsequently, after lung surgery, special treatment methods are required to facilitate the rapid restoration of pulmonary matter in the postoperative stage.
You can often notice a pathology when viewing an x-ray/fluorography, namely a deviation of the diaphragm. There are many factors for the occurrence of deviation. These include the following:
- excessive weight,
- genetic predisposition,
- pleurisy,
- a process in which pleurodiaphragmatic adhesions are deformed,
- diseases of the digestive tract and stomach,
- diseases of the intestinal tract, liver and other abdominal organs.
Analysis of such an indicator is carried out only when combined with other fluorography transformations. It is impossible to determine a conclusion based solely on changes in the aperture in a fluorography image.
The effectiveness of diagnosing tuberculosis and pulmonary diseases cannot be ignored. And no matter how annoying the sometimes incomprehensible conditions for performing fluorography in an institution, at work or somewhere under other circumstances may be, you should under no circumstances refuse. Often it is only through X-rays or fluorography that it is possible to establish the formation of tuberculosis, especially since this honey. the service is provided for free.
Heavy roots
If in the fluorography image there is nothing more than the severity of the roots of the chest, then we can say that the doctor has accurately and without doubt made the diagnosis. However, it cannot be ruled out that another chronic process exists. For example, a constructive illness of simple or protracted illnesses. This indicator, together with the expansion and thickening of the roots, is also typical for bronchitis of smokers.
In the current epidemiological negative circumstances, humanity is at risk, but first of all these are people with chronic lung diseases, immunodeficiency, smokers, and children. Tobacco smoking undoubtedly makes a harmful contribution to the formation and maintenance of the tuberculosis epidemic, primarily by weakening the lungs.
Summing up the results, it is necessary to note once again that annual x-rays/fluorography will be able to protect you from extremely dangerous diseases. Because timely detected lung cancer or tuberculosis in certain cases provides the only opportunity to survive these diseases.
Therapy
Schematic representation of pleural cavity drainage
Regardless of the origin, treatment of purulent pleurisy follows general principles.
Its first and main goal is to remove purulent exudate from the pleural area, which can be done in several ways:
- drainage;
- pleural or bronchoalveolar lavage;
- removal of pus using a vacuum;
- administration of medications (antibiotics, enzymes, etc.) directly into the affected area (therapeutic bronchoscopy).
Important. Removal of pathological effusion dramatically improves the patient's condition, reduces signs of intoxication, slows down or stops adhesions, helps to straighten the lung and reduce the pleural cavity.
Treatment is always comprehensive. Simultaneously with the evacuation of purulent fluid, the patient is prescribed antibacterial drugs (fluoroquinolones, cephalosporins, carbapenems, aminoglycosides). Medicines may be given by injection or orally, depending on the severity of the disease.
In addition, the following types of medications are recommended for the patient:
- immunostimulants and correctors;
- drugs to reduce intoxication of the body;
- vitamin and mineral complexes;
- infusion of glucose solution, electrolytes, protein agents (including blood plasma).
To quickly normalize the patient’s condition (strengthening protective mechanisms, leveling intoxication, returning homeostasis to a normal state, and so on) or in case of a strong pathological process, the following manipulations with blood are indicated:
- hemosorption;
- Ural Federal District;
- plasma- or plasmacytopheresis.
After the high fever, pain and cough have subsided, physiotherapeutic procedures are prescribed to speed up recovery, enhance natural drainage and prevent the formation of adhesions (or reduce this process):
- therapeutic and breathing exercises;
- various types of massage, for example, vibration, percussion, etc.;
- ultrasound therapy;
- electrophoresis.
Surgery can be performed if a chronic form develops. Depending on the indications, surgical procedures and the scope of surgical intervention may vary - from open drainage (thoracostomy) and closure of fistulas, to various options for removing the pleura and sections of the lungs.
Intrapleural thoracoplasty is often required; for example, this is more common with tuberculosis complications.
APICAL AND BOSTAL LAYERS AT THE APIPS OF THE LUNGS
PETRUSHA LEONID YURIEVICH
Chief physician of the COMPLEX CLINIC of Vladykino
Pulmonology is a branch of medicine dealing with the diagnosis, treatment and prevention of respiratory diseases (COPD, bronchitis, pneumonia, bronchial asthma, emphysema, etc.).
You should contact a pulmonologist if you have complaints about:
- cough, shortness of breath or shortness of breath, shortness of breath during exercise or at rest, sputum production
- snoring, sleep apnea
- chest pain when breathing
Pulmonary diseases (respiratory diseases):
- acute and chronic bronchitis bronchopulmonary aspergillosis tracheobronchitis
- bronchial asthma chronic obstructive pulmonary disease (COPD)
- emphysema
- pneumosclerosis
- lung cancer - diagnosis
- pneumoconiosis
- pneumonia
- pneumothorax
- psittacosis
- pulmonary embolism
- pulmonary fibrosis
- pulmonary hypertension
- pulmonary infarction
- hyperventilation syndrome
- sarcoidosis
- silicosis
- idiopathic fibrosing alveolitis
- pulmonary alveolar proteinosis
- alveolar microlithiasis
- sleep apnea (stopping breathing during sleep), snoring
- exogenous allergic alveolitis
Causes and pathogenesis of the disease
There are many reasons for the occurrence of pleural empyema, which explains the sufficient prevalence of this problem. These include:
- chest injuries (including gunshot wounds);
- infectious lung diseases - pneumonia, gangrene, abscesses, tuberculosis;
- operations performed on the esophagus, lungs and heart;
- lung cancer;
lesions of soft tissues, bones of the sternum and ribs (phlegmon, osteomyelitis);
- metastases from extrapulmonary malignant tumors;
- heart disease (pericarditis and infective endocarditis);
- acute inflammation of the abdominal organs and retroperitoneal space: peritonitis, pancreatitis, cholecystitis, liver abscesses;
- sepsis (generalized infection);
- pulmonary congenital and acquired (parasitic) cysts;
- medical errors (inadequate surgical treatment of wounds for chest injuries, frequent pleural punctures, incorrectly selected instruments for drainage, late treatment of external ulcers).
The main trigger factors for the occurrence of purulent pleurisy are:
- decreased immunity;
- penetration of pathogenic bacteria into the pleural cavity.
The result of this current situation is an inflammatory response from the pleura, which is a serous membrane covering the lungs and chest from the inside.
Purulent pleurisy
When bacteria get on it, they produce various toxins. Their effect is reduced to damage to pleural cells. The body responds to such irritation by producing an inflammatory fluid - exudate, which is absorbed by the serous membrane in large quantities.
If diagnosis and treatment are not timely at this stage, bacterial toxins continue to damage the pleura. The result is the impossibility of reabsorption of exudate. It accumulates in the pleural cavity and gradually becomes purulent.
The inflammation continues to increase. Above the fluid, the layers of the pleura of the lungs and chest are connected to each other. They begin to grow together, forming adhesions. Thus, the accumulation of pus is demarcated. It is possible to form pleurisy with several chambers, or encysted.
The consequence of the progression of this process can be fistulas, when pus “makes” its way out through the chest wall under the skin or into the bronchi. With the latter option, the appearance of a purulent cough with copious sputum is characteristic. This situation often leads to chronicity of the disease.
Occurrence and development of the disease
The reaction of the pleura to infection may differ, since the reactivity of a particular organism and the virulence of the microflora are always different. For example, an infection with weak virulence leads to the formation of a small amount of fibrinous effusion, which glues the pleural layers. As a result, adhesions and adhesions form around the infectious focus, causing the appearance of dry pleurisy. Microorganisms with higher activity provoke the accumulation of large amounts of fluid, leading to exudative pleurisy. Subsequently, it begins to progress and turns into a purulent form.
In some cases, the clinical picture of the inflammatory process immediately takes on a purulent form. As a rule, this occurs with abscesses, when the abscess breaks directly into the pleural cavity. If the pleura is not freed from pus in a timely manner, the infected fluid finds its way out through the muscle tissue and subcutaneous tissue of the chest walls, thereby forming phlegmon.
Serious attention is paid to purulent intoxication as one of the main causes of the pathology under consideration. The pleura itself has a pronounced sorption capacity and the ability to capture a large number of different toxins. Together with the breakdown products of tissues and leukocytes, they cause the development of severe forms of intoxication. Such a negative effect disrupts the protein and water-electrolyte balance, the basic functions of the circulatory system, up to the appearance of anemia.
A particular danger for the patient occurs when pyopneumothorax occurs. This special form of empyema is a rupture of an acute pulmonary abscess into the pleural cavity. The same thing happens when lung gangrene opens into the cavity with simultaneous necrosis of the lung tissue. In some cases, the cause of a breakthrough is a burst chronic abscess or a festering cyst. The impetus for the development of pyopneumothorax is most often a gangrenous abscess, gangrene of the lung and acute lung abscess. Other diseases provoke this pathology much less frequently.
A severe form of pneumothorax can be caused by a valvular mechanism of development. In this case, air is forced into the cavity without getting a free exit from there. In addition to purulent intoxication, the severity of the patient’s condition is determined by compression of the lungs with air, with a displacement of the mediastinal organs to the healthy side.
The onset of the inflammatory process is characterized by a vascular reaction, which is pleural hyperemia. Next comes a pronounced phase of fluid accumulation, during which the exudate permeates tissues and structures that do not contain blood vessels. The permeability of capillary walls in places of venous stagnation for blood proteins, fibrinogens and other blood elements increases.
Over time, the amount of purulent structure accumulates and increases in the pleural cavity, after which pleural empyema is directly formed. To stop the process, the cavity undergoes comprehensive sanitation. This procedure slows down and stops inflammation at almost any stage, but only timely treatment gives stable positive results.
How to treat pleurisy with folk remedies
It is important to understand that it is impossible to treat pleurisy with folk remedies alone, since the disease can quickly progress and lead to respiratory failure and suppuration of the effusion.
Treatment of pulmonary pleurisy with folk remedies involves the use of compresses and the use of infusions, decoctions, and tinctures.
- Beetroot juice helps with pleurisy. It is squeezed from fresh root vegetables and mixed with honey. For 100 g of juice, 2 tablespoons of honey are required. Take the product 2 times a day after meals. Each time you need to prepare a fresh portion, the composition does not need to be stored.
- Try to treat pleurisy with an infusion of herbs such as: mint, cudweed, coltsfoot, take a glass three times a day.
- Boil the roots (0.5 tsp) and rhizomes (0.5 tsp) of the Caucasian hellebore in 0.5 liters of water so that after evaporation you get a glass of liquid. Take 0.5 tsp. three times a day. The decoction is useful for the treatment of pleurisy, pneumonia, tuberculosis, and heart failure.
- Mix honey and onion juice in equal portions (you can take black radish juice instead of onions) - one tablespoon twice a day to treat pleurisy.
- Infusion of plantain leaf or common plantain. For half a liter of boiling water add 2 tbsp. l. dried plant. The liquid is filtered and drunk warm, 100-120 ml 4 times a day. The drink is harmless, has a healing and antibacterial character.
Symptoms of the development of hydrothorax
The symptoms of hydrothorax directly depend on the amount of fluid that is in the pleural cavity.
If the volume of pleural fluid is insignificant, its amount does not exceed 150 ml (such hydrothorax is called small), then this condition has practically no effect on the course of the underlying disease. With total hydrothorax, when fluid fills almost the entire lung cavity in a person, clear clinical signs of pathology appear.
Most often, water accumulates either only in the right lung, or in both at the same time. Left-sided hydrothorax is considered a rare form. It appears in cardiovascular failure, when fluid can accumulate not only in the pleural cavity or lungs, but also in the abdominal region.
Typically, pulmonary hydrothorax develops gradually, and its clinical signs increase as the pleural cavity of the lungs fills with fluid.
Signs of hydrothorax development:
- Gradually increasing shortness of breath, which especially torments people during physical activity.
- In the lower parts of the pleural cavity of the lungs, which are primarily filled with fluid, heaviness and discomfort are felt.
- With hydrothorax there is no pain and no fever. There is no inflammation in the protein contained in the liquid, so the person does not feel any signs of intoxication.
Hydrothorax can be determined not only by analyzing the patient’s complaints, but also by visual examination. Due to constant shortness of breath and chest discomfort, a patient with hydrothorax constantly strives to take a certain position. Shortness of breath is slightly relieved when the patient lies on the side of the affected lung or squats a little.
If you suspect the development of hydrothorax, you need to pay attention to the patient's abdomen. Due to the large amount of fluid not only in the lungs, but also in the abdominal cavity, the abdomen may become enlarged. In cardiovascular diseases, fluid enters the fat layer, which is manifested by swelling of the soft tissues.
In liver cirrhosis, hydrothorax has its own specific symptoms. With a similar reason for the development of pathology, the patient begins to experience severe shortness of breath, even with a small accumulation of fluid in the lungs. With cirrhosis of the liver, infection of the hymen may occur due to the entry of bacterial flora into its area.