- Reasons for development
- Types and types of disease
- The first signs of uterine cancer at an early stage
- Metastasis
- Stages of tumor development
- Diagnostics
- Modern principles of treatment
- Prognosis for different forms of the disease
- Is it possible to prevent uterine cancer pathologies?
- Clinics
Uterine cancer is a term used in modern oncology to designate any malignant tumor in the body of the uterus.
Invasive neoplasms of the female pelvic organs account for about 15% of all cancers in women. The most common of these malignancies is uterine cancer.
It is the fourth most common cancer, accounting for 7% of women's cancers, after breast, lung and colorectal cancer.
At the same time, endometrial cancer itself (endometrioid adenocarcinoma) is the most common gynecological malignancy in developed countries. In Russia, statistics on the prevalence of this pathology show an incidence rate of 5% of the total number of all cancer cases in women.
However, with this pathology the prognosis is usually favorable. This is due to the fact that most patients see an oncologist at an early stage. As a result, only 4% of cancer deaths in women are associated with endometrial cancer. More aggressive forms of malignancies, such as uterine sarcomas, account for less than 9% of uterine cancers but are associated with a more aggressive course and worse prognosis.
Uterine cancer: causes and risk factors for development
Certain factors can increase a woman's risk of developing endometrial cancer, but they do not always cause the disease. Having one or more risk factors for cancer does not necessarily mean you will develop the disease. But the absence of common risk factors does not mean that it will not develop.
General risk factors
Age over 50 years and postmenopause.
Increased number of menstrual cycles . Women who have had more menstrual cycles over their lifetime have an increased risk of endometrial cancer.
No previous pregnancies . During pregnancy, a woman's hormonal balance is disrupted and her body produces more progesterone and less estrogen.
Obesity . Excess fat increases estrogen levels, especially after menopause, which increases your risk.
Chronic diseases. Diabetes, endometrial hyperplasia and ovarian tumors can be considered risk factors and causes of uterine cancer.
Often, endometriosis is also considered a risk factor for uterine cancer. However, it has been proven that there is no connection between endometriosis and an increased risk of endometrial cancer.
Estrogen replacement therapy . Replacing estrogen without increasing progesterone levels after menopause may increase the risk.
Long-term use of Tamoxifen. Women who are treated with the drug tamoxifen for breast cancer have an increased risk of developing the disease.
Causes of the disease
There are several etiological factors that contribute to the formation of a tumor of the uterine body; oncogynecologists distinguish between estrogen-dependent, against the background of endocrine-metabolic disorders, and genetic.
The hormonal theory is characterized by hyperestrogenism. This type of cancer has a favorable prognosis; the cells are highly differentiated and treatable. With an increased level of the hormone estrogen, an anovulatory cycle, inability to conceive, late onset of menopause, and benign formations are observed.
Patients suffering from obesity, hypertension, and diabetes mellitus are prone to hormone-dependent cancer. Provoking factors are:
- frequent abortions;
- feminizing ovarian tumors;
- estrogen therapy;
- hyperplasia of the internal mucous layer;
- polypous formations;
- precancerous diseases;
- burdened hereditary history of malignant neoplasms of the internal genital organs and lower parts of the colon (colorectal cancer).
Endocrine metabolic disorders provoke the degeneration of healthy cells into cancer cells against the background of immunosuppression and atrophy of the internal mucous layer lining the organ cavity.
Provoking etiofactors can be early and promiscuous sexual life, radiation (both an occupational disease and for the purpose of treatment), diseases of the liver, adrenal glands, scar postoperative changes.
Types, classification
Uterine cancer is represented by two main types of tumors that develop from different tissues:
- Endometrial cancer develops in the lining of the uterus, called the endometrium. This is the most common type of pathology, accounting for more than 90 percent of cases.
- Uterine sarcoma is a rarer type of pathology; it forms in the muscles or other tissues of the uterus.
Endometrial cancer
Endometrial cancer is the most common form of the disease.
More than 80 percent of all cases of this disease are endometrioid adenocarcinomas .
The other 20% of endometrial malignancies are:
- serous adenocarcinoma - tumors that more often metastasize to lymph nodes and other parts of the body
- adenosquamous carcinoma , a rare type of cancer similar to endometrial adenocarcinoma and squamous cell carcinoma that lines the outer layer of the uterus
- carcinosarcoma , in which the cancer cells look like both endometrial cancer and sarcoma and have a high risk of spreading to lymph nodes and other parts of the body
Sarcoma of the uterus
Uterine sarcomas, which form in the muscular wall of the uterus, are rare, accounting for less than 4% of all cases.
Three main types of uterine sarcoma.
- Leiomyosarcoma is the most common type; this disease forms in the muscle wall (myometrium) and accounts for about 2% of cases.
- Endometrial stromal sarcoma . These tumors develop in the connective tissue that supports the endometrium, account for less than 1% of all cases and usually grow slowly.
- Undifferentiated sarcoma . The rarest subtype. This tumor is similar to stromal sarcoma, but is more aggressive. This type of cancer accounts for less than 1% of all cases.
Classification of uterine cancer
Classification for cancer of the uterine body is carried out depending on the size of the tumor, the degree of deepening of tumor cells into the muscle structure, the intensity of spread to nearby tissue and neighboring organs, the affected areas of the lymph nodes and the presence of distant metastases. The classified list is used to determine the stage of the disease according to the TNM standard and according to the International Federation of Obstetricians and Gynecologists (FIGO) system. Preinvasive cancer is characterized by the development of a lesion within the endometrium. The tumor name according to the standard is carcinoma in situ, Tis and stage 0. There are 4 stages of uterine cancer.
Education affects exclusively the body of the uterus:
- endometrium (T1a or IA);
- half-depth of the myometrium (T1b or IB);
- over half the depth of the myometrium (T1c or IC).
Stage 2 malignant process progresses to the cervix:
- into glandular tissue (T2a or IIA);
- deepens along the cervical layers (T2b or IIB).
Stage 3 cancer spreads to the vagina, appendages or lymph nodes:
- the outer layer of the uterus and appendages is affected (T3a or IIIA);
- the affected cells have spread throughout the vagina (T3b or IIIB);
- the presence of metastases in the pelvic or peri-aortic lymph nodes (N1 or IIIC).
Uterine growth 4 degrees with metastasis:
- on the bladder or in the layers of the rectum (T4 or IVA);
- in lung tissue, liver, bones, distant lymph nodes (M1 or IVB).
There are also different degrees of differentiation of cancer cells - from G1 (increased level of tissue maturity) to 3 (poorly differentiated growth). With highly expressed differentiation, formation develops at a reduced rate, and the likelihood of the lesion spreading with metastases decreases. When diagnosing a poorly differentiated neoplasm, the survival prognosis worsens. Depending on the structure at the microscopic level, the morphological type of oncology is distinguished:
- adenocarcinoma;
- clear cell carcinoma;
- squamous;
- glandular-squamous;
- serous;
- mucinous;
- undifferentiated.
The morphological variety in particular indicates the degree of malignancy. The course of undifferentiated pathology is negative and unreliable, and squamous growth has a high chance of recovery. Pathology forms and develops in exophytic (through the uterine fissure) and endophytic (through layers of the muscular structure) form or has a mixed combination of course. The tumor is located on the territory of the fundus and body of the uterus. In the lower part, the neoplasm is localized in rare cases.
Uterine cancer: symptoms and signs
Common symptoms of early stage uterine cancer include:
- bleeding not associated with menstruation;
- postmenopausal bleeding;
- unusual vaginal discharge without visible blood;
- difficult or painful urination;
- pain during intercourse;
- pain and/or pressure in the pelvic area;
- unintentional weight loss.
The most common first sign of early stage uterine cancer (symptoms occurring in 90% of women) is abnormal bleeding. Especially common is postmenopausal (PMP) bleeding.
Bleeding becomes a justified reason for visiting a doctor, as a result of which in 70-75% of women the pathology is diagnosed already at stage I.
Screening tests for uterine cancer are not currently recommended in Europe for women without symptoms. There is no evidence that screening in asymptomatic women plays a role in early detection. Even in women who take tamoxifen after breast cancer or have a cancer syndrome.
There are also no specific tumor markers to identify this disease.
Uterine sarcoma may present similarly to endometrial carcinomas, with vaginal bleeding and often pelvic pressure. Imaging shows swelling and an increase in the size of the uterus.
Leiomyosarcoma may present in women in the early sixth decade of life with irregular menstruation or postmenopausal bleeding. Its early signs include pain, pelvic pressure and rapidly increasing pelvic mass. Unfortunately, the diagnosis is rarely made before abdominal surgery.
Endometrial stromal sarcoma (ESS) is commonly associated with postmenopausal bleeding, pelvic pain, and uterine enlargement. Like mixed Müllerian tumors (MMT), ESS is usually present in the seventh decade of life. Weight loss, anorexia and changes in bowel or bladder habits are the main symptoms of this rapidly progressive disease.
Causes of endometrial cancer
The main significance in the occurrence of hormone-dependent endometrial cancer of the uterus is hyperestrogenism occurring over a long period of time.
In this case, endometrial cancer becomes a kind of target for steroid sex hormones, which normally provide phase changes in the uterine mucosa. Disturbed hormonal homeostasis, which is the result of anatomical and functional changes occurring in the hypothalamic-pituitary-ovarian system, contributes to the development of proliferative and then hyperplastic processes in the endometrium. But the exact cause of the appearance of a precancerous condition and cancer against this background has not yet been precisely established.
Risk factors for hormone-dependent endometrial cancer are:
- No history of childbirth;
- Infertility;
- Late menopause;
- Diabetes;
- Arterial hypertension;
- Hereditary burden of ovarian, colon, breast, endometrial cancer;
- Hormone replacement therapy during postmenopause;
- Obesity;
- Use of the drug Tamoxifen in the treatment of breast cancer.
Autonomous endometrial cancer develops in women who do not have metabolic-endocrine disorders and in the absence of hyperestrogenism. The occurrence of this type of cancer is based on changes in immunity associated with a significant decrease in the number of T-lymphocytes and inhibition of all their subpopulations.
Autonomous endometrial cancer usually appears in elderly, thin women, who may have a history of bleeding in the postmenopausal period against the background of endometrial atrophy.
Metastases
The rate and extent of metastasis depends on the type of tumor, general hormonal levels and many other factors.
Metastases to regional lymph nodes can begin to appear when the tumor reaches the advanced second stage.
The first separated metastases most often affect the greater omentum. Metastasis to the spine and liver is also common.
Treatment
Treatment of endometrial cancer, similar to diagnosis, is carried out in several ways. It directly depends on the stage of the disease. Carry out:
- surgical removal of a malignant tumor. Several methods are used. Complete elimination of the endometrium can be carried out only in the initial stages, when no metastases are detected. Direct removal of the uterus through the vagina can be carried out at the first or second stage of the lesion. Sometimes the body, cervix, uterine tubes and ovaries are cut out. The prognosis from surgery is most often positive, but there is a fairly high probability of cancer reappearance;
- radiation exposure to a cancer tumor using ionizing or X-ray radiation;
- chemotherapy;
- taking hormonal medications – is carried out to restore the normal level of female hormones in the body.
Stages
Stage 0
This stage is also known as carcinoma in situ. Cancer cells are found only in the surface layer of endometrial cells, without growing into the layers of cells below. This is a precancerous lesion.
Stage 1 uterine cancer
The tumor is just beginning to grow in the body of the uterus. It can grow into the glands of the cervix, but not into the supporting connective tissue. The tumor has not spread to lymph nodes or distant sites. This stage has two subcategories:
- Stage IA: In this earliest form, the tumor is in the endometrium and may develop from the endometrium less than halfway through the underlying muscle layer of the uterus (myometrium). It did not metastasize to lymph nodes or distant sites.
- Stage IB: The tumor has grown from the endometrium into the myometrium, more than halfway, but has not spread beyond the body of the uterus.
Stage 2
The tumor has spread from the uterine body and is growing into the supporting connective tissue of the cervix (cervical stroma). The tumor has not spread to neighboring organs and tissues, lymph nodes, or distant areas of the body.
Stage 3
The tumor has spread outside the uterus or into nearby tissue in the pelvic area. This stage has four subcategories:
- Stage IIIA. Spread to the outer surface of the uterus and/or to the fallopian tubes or ovaries (epididymis). The tumor did not metastasize to lymph nodes or distant sites.
- Stage IIIB. The tumor has spread to the vagina or tissue around the uterus (parameter). Lymph nodes are not affected, there are no distant metastases.
- Stage IIIC. The tumor may spread to some nearby tissues, but does not invade the bladder or rectum. The tumor had invaded the lymph nodes of the pelvis, but not the lymph nodes around the aorta or distant sites.
- Stage IIIC2: The tumor may have spread to some nearby tissue but has not invaded the bladder or rectum. The tumor has spread to the lymph nodes around the aorta (periaortic lymph nodes), but not to distant sites.
Stage 4 uterine cancer
The tumor has spread to the inside of the bladder or rectum (lower part of the colon), to the lymph nodes in the groin, and/or to distant organs such as the bones, omentum, or lungs.
Stage IV uterine cancer has two subcategories:
- Stage IVA: The tumor has spread to the lining of the rectum or bladder. It may or may not have spread to nearby lymph nodes, but not to distant sites.
- Stage IVB. The tumor has spread to distant lymph nodes, the upper abdomen, the omentum, or to organs distant from the uterus, such as the bones, omentum, or lungs. The tumor can be any size, and it may or may not have spread to the lymph nodes.
Diagnosis of cancer of the uterus (endometrium)
Diagnosis of cancer of the body of the uterus is always associated with penetration into the organ, which is deeply against nature, which has placed the fetal reservoir in practical inaccessibility. No “soft” examination methods - ultrasound or palpation - can solve the diagnostic problem.
Diagnosis of uterine cancer is completed under a microscope, and tissue for examination is taken from the tumor, wherever it is located. The uterine cavity, in which the malignant degeneration of the mucous membrane began, is clearly visible during ultrasound examination; you can even outline the area where the tumor tissue is growing; it can only be taken from there for microscopy using surgical diagnostics.
Modern ultrasound machines detect endometrial polyps smaller than half a centimeter, and all diagnostics that clarify the cellular structure have remained virtually unchanged over the past few decades.
The first stage of diagnosis is aspiration biopsy
Aspiration is the pulling of cellular material from the uterine cavity into a syringe, a simple manipulation. However, it involves penetration into a sterile internal space. With a fairly extensive lesion, the cells are absorbed already in the cervical canal, but with minimal neoplasm, preliminary irrigation of the uterine cavity with a solution may be required, with the collection of this washout for microscopic examination. The manipulation is called aspiration biopsy, but in fact it is not a biopsy - taking a piece of tissue, but a collection of scattered cells, that is, cytological diagnosis.
If microscopy of the material obtained during aspiration reveals a sufficient number of cancer cells, which allows the cytologist to express an unambiguous opinion, then the invasive diagnosis may be completed and all that remains is to look for metastases and determine treatment tactics. If there is no certainty, the next stage is diagnostic curettage of the uterine cavity.
The second stage of cancer diagnosis is separate curettage
Diagnostic curettage of the uterus provides greater certainty, since entire layers of cells obtained during “cleaning” are examined under a microscope. Based on the cell layers, it is already possible to determine the degree of aggressiveness of the tumor and its type.
Curettage is performed separately: first, the mucous membrane of the cervical canal is removed, then the entire endometrium is scraped off. Formally, the same abortion, but with different – noble diagnostic purposes. This examination is performed in a small operating room and under general anesthesia.
Diagnostics
In Belgium, the algorithm for diagnosing uterine cancer pathology is based on the principle of reasonable sufficiency. The patient will not be prescribed those types of studies that are not necessary.
Specific symptoms in combination with gynecological examination data often provide sufficient grounds for the suspected presence of a tumor.
In order to clarify the location of such a tumor, an ultrasound examination can be performed.
The final diagnosis is made based on the results of a biopsy performed during the hysteroscopy procedure.
This set of diagnostic procedures provides the oncologist with comprehensive data to make the correct diagnosis.
Medical imaging methods such as CT, MRI, PET, SPECT, etc. are used only when there is reasonable suspicion of damage to other organs and systems of the body by a sprouted tumor or metastases.
This approach makes the diagnostic process fast, accurate and at the same time reasonable in price.
International classification
To assess the extent of cancer spread, the FIGO system is used: Stage I (T1):
- IA – the tumor is located only in the endometrium;
- IB – malignant formation affects half of the muscle tissue of the uterus;
- IC – cancer affects more than half of the myometrium.
Stage II (T2):
- IIA – endocervix affected;
- IIB – the tumor grows into the stroma of the cervix.
Stage III (T3):
- IIIA – invasion of the serosa, fallopian tubes or ovaries;
- IIIB – cancer spreads to the vagina;
- IIIC – metastases are detected in the pelvic lymph nodes.
Stage IV (T4):
- IVA – metastases grow into the walls of the bladder, the lumen of the large intestine;
- IVB – the tumor is found in distant organs and lymph nodes.
Treatment of uterine cancer in Europe
The main treatment method for uterine cancer abroad is surgery. Other methods either complement surgery or are used when surgery is not possible or must be postponed.
Surgery
The type of surgery performed depends on the stage of the disease, as well as individual fertility problems.
Simple hysterectomy is the most common type of surgery. During a simple hysterectomy, the uterus and cervix are removed.
Radical hysterectomy - This type of surgery involves removing the uterus, cervix and ovaries, as well as all surrounding tissue (parametria) and the upper part of the vagina.
Lymphadenectomy - removal of lymph nodes in the pelvis.
Chemotherapy
Modern chemotherapy for this pathology is carried out using various combinations of chemotherapy drugs. The most commonly used combination is cisplatin and paclitaxel.
Hormone therapy
Uterine cancer is a hormone-dependent tumor. Therefore, by changing the hormonal balance towards an excess of gestagens, it is possible to achieve good results in the treatment of relapses and metastases of uterine cancer. This type of hormone therapy can be used alone or in combination with surgery, chemotherapy, or radiation therapy.
Typically, the treatment regimen may include high doses of progestins and gonadotropin-releasing hormone.
Immunotherapy in the treatment of uterine cancer abroad
Immunotherapy for uterine cancer is based on the use of checkpoint inhibitors.
Checkpoint inhibitors are effective only for treating patients with unresectable metastatic endometrial cancer with certain genetic characteristics. This is microsatellite instability (MSI-H) or deficiency of mismatch repair (dMMR).
Radiation therapy
This type of treatment is used both as an adjunct to surgery and as an independent treatment for inoperable forms. Currently, several methods of radiation therapy for uterine cancer are used.
External beam radiation therapy (EBRT) directs a beam of radiation from outside the body to cancerous tissue inside the body. This is a cancer treatment option that uses low doses of radiation to destroy cancer cells and shrink tumors. EBRT helps reduce the risk of gastrointestinal and sexual side effects commonly associated with radiation treatment for uterine cancer. It is a quick, painless, outpatient procedure and does not carry the usual risks of surgery, such as bleeding, post-operative pain, or the risk of stroke or thrombosis.
High dose rate (HDR) brachytherapy for uterine cancer is a type of internal radiation therapy that places implants near or inside the tumor that emit radiation that is quickly absorbed by body tissue. This method delivers the maximum radiation dose to cancerous tissue while minimizing exposure to surrounding healthy tissue.
Intensity modulated radiation therapy (IMRT) uses advanced software to plan precise radiation doses based on tumor size, shape and location.
Varieties
Based on localization and spread to neighboring organs, endometrial cancer or uterine precancer is divided into the following degrees:
- damage only to the mucous layer of the uterus;
- with distribution to all layers of the organ;
- precancerous lesions of the cervix;
- oncology moves beyond the uterus;
- damage to nearby internal organs by this disorder;
- spread of cancer metastases to distant organs and lymph nodes.
Absolutely all stages of the disease can be diagnosed using ultrasound.
Benefits of treatment in Belgium
Oncology clinics in Belgium use a differentiated approach to the selection of methods and tactics for treating uterine cancer. The choice of treatment is made based on the principles of evidence-based medicine, taking into account the individual characteristics of the patient and the course of her disease.
Treatment in Belgium will give you a number of advantages.
- Possibility of cancer treatment with temporary fertility preservation. Treatment can be conservative (hormone therapy) and carried out, including during pregnancy. Removal of the uterus is performed after childbirth.
- Treatment of complex inoperable forms of oncology using immunotherapy methods (if there are immunological indications) using checkpoint inhibitors and angiogenesis inhibitors (bevacizumab).
- Comprehensive rehabilitation programs, including not only the prevention of relapses and metastases, but also psychological assistance.
- Possibility of optimizing the cost of treatment for uterine cancer. In Belgium, the price of the operation will be 20-40% lower than in Germany or Israel.
Complications
If treated incorrectly and symptoms are ignored, there is a high probability of developing complications such as:
- spread of cancer to nearby organs;
- cancer metastases from the uterus to distant areas of the body, which are transferred with the bloodstream;
- secondary occurrence of oncology even after complete recovery;
- death of a woman.
To prevent such terrible consequences, women and girls need to regularly undergo ultrasound of the abdominal organs.
The most positive prognosis is for patients in whom signs of this disorder were detected in the early stages. For patients with stage 3 or 4 endometrial cancer, the prognosis worsens, but with the right combination of treatment and surgery, there is the possibility of a complete cure (but in this case, do not forget about the recurrence of the disease).
Forecast
Due to the fairly typical early clinical picture, most cases of endometrioid cancer are treated at the first stage of the disease.
Overall 5-year survival rates for all grades and histologic subtypes are approximately 85–95%, 75%, 50%, and 20% for surgical grades 1, 2, 3, and 4 disease, respectively.
For grade I surgical disease, the 5-year survival rates for grades 1, 2, and 3 endometrial cancer are 92%, 87%, and 74%, respectively.
Clear and papillary serous carcinomas have the lowest overall 5-year survival rates. When considering all stages together, the 5-year survival rates for clear and papillary serous carcinomas are 51% and 46%, respectively.
Endometrioid adenocarcinoma has an overall 5-year survival rate of approximately 76%. Adenosquamous carcinoma has an overall 5-year survival rate of approximately 68%.
Deeper myometrial invasion is associated with metastases to the pelvic and para-aortic lymph nodes. All these are unfavorable prognostic factors. Recurrence rates of up to 46% are observed with deep myometrial invasion (more than half) compared with 8-13% with superficial or no invasion.
Most recurrent endometrial cancers are diagnosed within 2 years. Recurrences in patients treated with surgery alone tend to be more localized to the pelvis (40%), especially the vaginal cuff.
The prognosis for these patients is better if the initial diagnosis was more than 2 years before relapse.
Uterine sarcomas have a high recurrence rate
The overall 5-year survival rate for leiomyosarcoma (LMS) is 15-25%.
Stage 1 LMS has a 58% and 70% 5-year survival rate after surgery without and with radiation therapy, respectively. Recurrences are rarely localized and most often appear in the lungs.
Early-stage mixed Mullerian tumor (MMT) has a 5-year survival rate of approximately 50%, whereas stages II-IV have a 5-year survival rate of 5-15%.
These statistics reflect the prognosis with tactically correct treatment carried out in accordance with the principles of the European Society of Medical Oncology (ESMO). In developing countries, the survival rate is still, unfortunately, significantly lower.
Etiology
The main causes of uterine precancer include:
- female gynecological diseases;
- disorder or complete cessation of menstruation;
- taking large quantities of medications that contain too much estrogen;
- genetic predisposition. If one of your close relatives suffered from such an illness, then there is a high probability of recurrence of endometrial cancer in other relatives;
- prolonged abstinence from sexual intercourse;
- frequent change of sexual partners;
- absence of children, and, accordingly, pregnancy and childbirth in a woman, as well as in the case of bearing her first baby at the age of more than thirty years;
- artificial termination of pregnancy, more than once;
- the appearance of the first menstruation in a girl under the age of twelve;
- critical increase in body weight;
- a history of diabetes mellitus;
- mental disorders;
- unhealthy lifestyle, abuse of alcoholic beverages and smoking;
- prolonged exposure to stressful situations;
- a sharp decrease in immunity;
- untimely ultrasound examination of the genital organs;
- the onset of menopause over the age of fifty-five.
Prevention
Most measures to prevent uterine cancer involve reducing exposure to risk factors.
- taking combined oral contraceptives (COCs) may reduce the risk by reducing the amount of endometrial growth;
- use of progestin-secreting intrauterine devices (IUDs) also helps reduce risk.
- When prescribing estrogen hormone replacement therapy, it is also recommended to add a progestin component to the course to reduce the level of risk.
Causes of cancer development
There are 2 hypotheses for the appearance of carcinoma: hormonal and non-hormonal. In the first case, the cause is an increase in the level of estrogen in a woman’s body and dysfunction of the endocrine system. This form of cancer is found in patients suffering from obesity, arterial hypertension, diabetes mellitus, infertility, and polycystic ovary syndrome. Autonomous carcinoma develops against the background of endometrial atrophy and a decrease in general immunity, which is observed with the onset of menopause.
Main risk factors:
- hereditary predisposition;
- a large number of medical abortions;
- hyperplasia, endometrial adenomatosis;
- late menopause;
- taking oral contraceptives (estrogens);
- uterine polyps;
- early onset of menstruation;
- treatment with Tamoxifen;
- radiation therapy of the pelvic organs;
- infertility, lack of childbearing;
- polycystic ovary syndrome.
Precancerous diseases include polyposis and adenomatosis of the endometrium, which lines the inner layer of the uterus. In 70% of cases, oncology is diagnosed in women during menopause, in 20% symptoms of the pathology arise during perimenopause, and in 7–10% of patients the disease progresses until menopause.
Uterine cancer treatment stages 1, 2, 3. Symptoms, signs, metastases, prognosis.
What is uterine cancer?
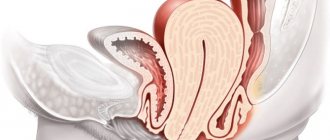
Cancer of the uterine body (endometrial cancer) is a malignant tumor of the mucous membrane (endometrium) from the inside lining the body of the uterus (from the side of the uterine cavity).
Most often, uterine cancer occurs in postmenopausal (post-menopausal) women, but recently there has been a tendency towards its “rejuvenation”. Increasingly, uterine cancer occurs in women of fertile age before menopause.
In most patients, uterine cancer is diagnosed in stage I of the disease (72%), stage II accounts for 12%, stage III – 13%, stage IV – 3%.
What causes uterine cancer?
The causes of uterine cancer (etiology) are not fully understood. In most cases, it develops against the background of estrogenization of the woman’s body, i.e. against the background of an excess of female sex hormones - estrogens. This is the 1st pathogenetic type of uterine cancer. It accounts for 75% of all endometrial cancer cases.
Excess estrogen is, on the one hand, the result of hormonal disorders, on the other hand, it itself leads to the aggravation of these hormonal disorders. The uterine mucosa reacts in a certain way to excess estrogen, and endometrial hyperplasia develops.
The following types of endometrial hyperplasia are distinguished:
- simple endometrial hyperplasia without atypia;
- complex (adenomatous) endometrial hyperplasia without atypia;
- simple atypical endometrial hyperplasia;
- complex (adenomatous) atypical endometrial hyperplasia.
The first two options are classified as background diseases of the uterine body (endometrium), 3 and 4 – as precancerous. Moreover, complex atypical endometrial hyperplasia deserves special attention, since the probability of its degeneration into cancer is more than 80%.
These variants of endometrial hyperplasia and endometrial cancer represent different phases of the process of changes in the endometrium under the influence of excess estrogen.
Thus, the following chain of changes is possible:
- complex (adenomatous) endometrial hyperplasia without atypia;
- complex (adenomatous) atypical endometrial hyperplasia;
- cancer of the uterine body (endometrium).
In addition to changes in the lining of the uterus, pathogenetic type 1 endometrial cancer is characterized by metabolic disorders (metabolic syndrome). It is characterized by:
- obesity;
- diabetes;
- arterial hypertension.
Estrogen is formed in a woman’s adipose tissue; excess adipose tissue leads to excess estrogen. The pathological circle closes.
Uterine cancer of the 1st pathogenetic type
Cancer of the uterine body, developing according to the 1st pathogenetic type, is usually detected in the early stages and is characterized by a favorable prognosis.
Uterine cancer of the 2nd pathogenetic type
The second pathogenetic type of uterine cancer develops against the background of normal endometrium without any metabolic or hormonal disorders. It accounts for 25% of all cases of uterine cancer. Tumors of this type have a high malignant potential. This type of cancer has a less favorable prognosis.
Uterine cancer of the 3rd pathogenetic type
Currently, a third pathogenetic type of endometrial cancer is being described, which is a genetically inherited form. This cancer is inherited and is combined with non-polyposis colon cancer.
Consequences
Of course, the consequences of cancer are extremely serious. Without treatment, metastases may form in vital organs. As a result, this will lead to death. At the same time, it is important to remember that the development of the condition can be quite rapid, even if initially it developed slowly, then its intensity may change. Therefore, you cannot delay treatment.
Moreover, the younger the patient, the faster the pathological process occurs. That is, postmenopausal cancer is often less dangerous than premenopausal cancer.
Forms and stages
According to the generally accepted classification system, several types of uterine cancer are distinguished. All of them relate to the degeneration of endometrial cells into malignant forms with a location within the reproductive organ or with germination beyond its limits.
- Hormone-dependent adenocarcinoma is diagnosed in almost 70% and is the most common. It is often called glandular cancer. Dangerous due to a long latent period that is asymptomatic. Formed in the tissues of the ovaries, uterine fundus, and cervical canal. The age of increased risk is considered to be the period from 40 to 65 years; during menopause, the likelihood of developing the disease increases significantly under the influence of an imbalance of sex hormones. It occurs in several varieties and has 4 stages. The prognosis for treatment and the likely life expectancy depend on the general condition of the body, the rate of tumor growth and the stage at which treatment measures were started. It is curable in the early stages. The most commonly used method is surgical removal of the uterus and appendages, followed by chemotherapy in combination with HRT.
- Clear cell adenocarcinoma of the endometrium develops quickly, is aggressive in nature, and is successfully diagnosed in the early stages. It is rare; the vast majority of patients are postmenopausal. Requires surgical intervention in combination with complex therapy.
- Squamous cell carcinoma is formed from mucous and epithelial cells. The form is aggressive, mainly affecting the cervix. It has several types and 4 stages, differing in clinical picture, degree of damage to the organ and surrounding space. Symptoms are similar to other types of cancer of the uterine body. Gives complications to the kidneys, urinary and lymphatic systems, and liver. Surgical intervention with removal of the organ, in some cases with part of the vagina and ureter, is recommended.
- Mucinous adenocarcinoma is a hormone-dependent neoplasm. It is rare and the prognosis for the patient is favorable. A special feature is the poor response to radiation therapy, so this type of treatment is almost never used. Particular attention is paid to follow-up, since relapses are common. Appears in older women with a history of repeated inflammatory processes. Also, risk factors include hormonal imbalance, diabetes, endometriosis, and genetic predisposition. The disease is characterized by a long asymptomatic period. Treatment is carried out by surgical intervention.
- Glandular squamous cell carcinoma is a poorly studied form, is very rare, affects the cervix and fundus of the uterus, and occurs against the background of age-related hormonal changes. Postmenopausal women are at risk; the first signs of uterine cancer most often appear already at stages 2-3. They grow quickly and are aggressive. Treatment is facilitated by clear localization of the tumor, which gives a favorable prognosis with timely surgery to remove the uterus.
- Undifferentiated is considered one of the most dangerous; the prognosis is determined by the degree of organ damage. At stage 1, treatment gives very good results up to complete healing. The species is dangerous due to the occurrence of repeated outbreaks.
Read
How to relieve the symptoms of menopause in women?
All types of the disease are characterized by progressive development. According to the severity of the condition and the level of organ damage, 4 stages are distinguished:
- the tumor grows only in the endometrium, gradually affecting muscle tissue;
- growth into the stroma of the cervix is observed;
- changes affect the fallopian tubes, ovaries, vagina, pelvic lymph nodes;
- tumor and metastases are found in distant organs.
Metastasis
The spread of cancer cells is possible through the lymphatic tract, blood vessels and peritoneum.
Lymphogenic metastasis occurs in the nearest (regional) pelvic lymph nodes. At an early stage and high differentiation (G1-G2), the probability of lymph node involvement does not exceed 1%. If cancer cells invade the myometrium, the risk of metastasis increases to 6%. If the tumor affects a large area, penetrates deep into the uterine wall or spreads to the cervix, metastases in the lymph nodes are found in 25% of patients.
Hematogenous metastasis occurs later. Tumor cells travel through blood vessels to the lungs, bones and liver.
Implantation metastases occur on the peritoneum and omentum when the outer layer of the uterus grows and the fallopian tubes are damaged.
The danger of cancer is not only functional disorders in the functioning of organs and systems caused by the replacement of normal cells with atypical ones. The neoplasm spreads throughout the body, and this becomes too dangerous, as the disease becomes inoperable.
First, the tumor grows into nearby tissues (the organ itself or neighboring ones), i.e. it metastasizes. The mechanism of spread is as follows: modified cancer cells begin to separate from the primary tumor. These are the first metastases of uterine cancer, which is characterized by the onset of a pathological process in nearby organs (stage 3).
The transition from the third stage to the fourth means that the lymphatic system, the main “carrier” of atypical cells to distant organs, undergoes metastasis. Damage to the lymph nodes close to the primary tumor indicates a real danger of spread throughout the body. If distant ones are affected, then uterine cancer metastases can affect almost any organ (lungs, brain, etc.) or musculoskeletal system.
The initial stages of uterine cancer are relatively easy to treat surgically, since the tumor has a relatively clear localization. In the future, removal of the pathological focus is often difficult or even impossible, since in addition to the primary tumor, multiple metastases appear in the body, penetrating entire layers of tissues of different types.
In case of cancer in the body of the uterus, the main routes of metastasis are the lymphatic vessels and nodes, and at the terminal stage the circulatory system also participates in the spread.
First, the lesion spreads to the lymph node structures in the iliac region and hypogastric zone. Much less often, the lesion affects other groups of pelvic lymph nodes.
Metastasis extends to the cervical canal and beyond the uterine body. In a hematogenous manner, metastases penetrate from the upper uterine region into the appendages; in addition, the vagina, and sometimes even the kidney or liver or bone tissues are affected.
Manifestations at different localizations
When the oncological process spreads to the cervical area, the clinical picture of the disease is supplemented by such a pathological condition as pyometra - accumulation of purulent contents in the uterine cavity. In this case, signs of intoxication of the body resulting from the development of an inflammatory reaction are observed: an increase in general weakness, a feverish state, and high body temperature.
If a tumor develops on the anterior wall of the uterine body, as it grows, compression of the urinary tract occurs and the oncological process spreads into the bladder. In this case, signs such as blood in the urine, changes or disturbances in urination processes, and pain when trying to empty the bladder appear.
When the tumor is localized on the back wall of the uterus, the intestines are affected as the oncological process worsens. In this case, patients note a violation of the act of defecation and its accompanying pain, and the presence of impurities of fresh blood in the stool.
When the oncological process generalizes into the pelvic cavity, ascites develops—an accumulation of fluid in the abdominal cavity. If metastasis of endometrial cancer of the uterus occurs, the symptoms are complemented by the appearance of intense pain in the bones, weakening of the musculoskeletal system (frequent fractures), the development of jaundice (with the formation of metastases in the liver), deterioration of appetite and a sharp decrease in body weight.
In most cases, the prognosis for specific treatment of this cancer is quite favorable. The sooner pathological changes in the structure of the endometrium of the uterus are identified, the easier it is to eliminate them. Regular preventive examinations by a gynecologist, timely contact with a specialist in the event of the slightest disturbance in the menstrual cycle, the nature of menstruation, or the appearance of suspicious vaginal discharge helps to reduce the time of specific therapy and avoid the development of extremely severe complications.
Features of oncology detection: diagnostics
If symptoms and complaints occur, a woman should immediately visit an antenatal clinic. Diagnosis of endometrial cancer includes the following procedures:
- Examination of the uterine cavity by a gynecologist using special mirrors.
- Carrying out a biopsy procedure, as well as curettage of the uterine cavity and cervical canal. Conducting an ultrasound of the pelvic organs.
- Patients are also prescribed a chest x-ray.
- Hysteroscopy, as well as CT or MRI.
- Laboratory research: blood test, urine test, coagulogram.
Carrying out such diagnostic procedures makes it possible to determine the degree of histopathological tumor. These techniques make it possible to determine the size of the tumor, the presence of signs of enlargement, as well as the location and nature of damage to neighboring organs. Each of the methods proposed above has its own characteristics and allows you to determine the corresponding deviations.
- Examination of the vagina using special mirrors reveals the absence of lesions of the vagina and cervix.
- A biopsy or curettage makes it possible to collect fragments of tumor tissue for subsequent laboratory testing.
- Ultrasound allows you to identify the location of the tumor, size, contours and other useful information.
One of the most popular methods for diagnosing cancer is the fluorescence test technique. The procedure is accompanied by the introduction of special substances that accumulate in the tumor with their subsequent registration. The procedure has a significant advantage - the ability to detect even microscopic foci of tumors.
Signs characterizing endometrial cancer
The disease at stages 1 and 2 is usually asymptomatic. In some cases, there are single mild symptoms that the woman practically does not notice. A pronounced symptom that determines the presence of cancer in the body appears at stage 3 together with metastases in neighboring tissues.
Characteristic signs of endometrial cancer:
- pathological disorders are observed in the menstrual cycle - the nature of the discharge can be abundant or scanty;
- uterine bleeding during the menstrual cycle;
- painful sensations in the uterine area with varying intensity - depending on the size of the tumor;
- purulent vaginal discharge with an unpleasant odor appears, which indicates the addition of a secondary infection or inflammatory process;
- blood impurities are observed during urination;
- there is blood in the stool;
- in the lumbar back there is pain that occurs in separate attacks;
- in some cases, there is a violation during bowel movements - constipation or diarrhea;
- in the area of the small intestine there is increased gas formation, which indicates a significant size of the tumor filled with liquid - this can be determined by ultrasound;
- problems with appetite appear – there is a decrease or complete absence;
- a woman suddenly loses weight;
- there is pronounced weakness in the muscles against the background of rapid fatigue;
- physical activity decreases, which leads to a complete loss of the ability to perform physical activity.
When the first suspicious symptoms appear, you should immediately consult a doctor - this will allow you to start treatment in the early stages of the disease. Detection of pathology at stages 3 or 4 reduces a woman’s chance of a full recovery.
Endometrial cancer - risk factors
Endometrial malignancy usually produces clear symptoms at an early stage, allowing the disease to be quickly diagnosed and effectively treated. You should pay attention to intermenstrual bleeding or bleeding from the genital tract in the postmenopausal period, as well as copious, unpleasant-smelling, bloody or purulent-bloody vaginal discharge. There may also be pain in the abdomen or lumbosacral spine.
How is endometrial cancer diagnosed?
Uterine cancer can be detected using transvaginal ultrasound. If cancer is suspected, invasive tests requiring anesthesia are also necessary: curettage of the uterine cavity or hysteroscopy with biopsy.
To identify possible metastases, a chest x-ray and computed tomography of the abdomen and pelvis are performed. In some cases, magnetic resonance imaging of the reproductive organ is indicated, which allows one to assess the locoregional condition.
The following are factors that predispose to the development of endometrial cancer:
- early first menstruation and late last menstruation in a woman’s life;
- childlessness (the period of pregnancy and breastfeeding helps to reduce estrogen levels with a balanced production of another hormone - progesterone, which is important for women);
- use of hormone replacement therapy with estrogen alone;
- obesity (adipose tissue is the site of hormonal transformation);
- diabetes;
- menstrual irregularities that lead to increased hormone levels, such as polycystic ovary syndrome .
Genetic characteristics also predispose to the development of endometrial cancer.
Main symptoms of the disease
If menopause has not yet occurred, cancer may manifest itself as prolonged, heavy bleeding during menstruation. Bleeding may also occur in the middle of the cycle. Since endometrial cancer most often occurs in older women, it is characterized by uterine bleeding: both spotting and heavy. Bloody discharge during menopause is observed in 90% of cases of uterine cancer. In other cases, there may be no symptoms.
In addition to bleeding, purulent discharge may appear. When the tumor compresses the cervix and ureter, pain appears in the lower abdomen and lumbar region. In later stages, ascites or large tumors in the ovaries and greater omentum may develop.
A uterine tumor is often detected by ultrasound, which is recommended for older women to do at least once a year. If the cycle is disrupted and there are signs of endometrial hyperplasia, diagnostic curettage of the uterine cavity is indicated. The information content of such a study for uterine cancer during the postmenopausal period gives almost 100% results. Histological analysis of the material allows a final diagnosis to be made.
After determining the nature of the tumor, the patient is sent for a general examination to identify metastases in the body and determine the stage of the cancer. For this purpose, colonoscopy, chest x-ray, and computed tomography are performed.
Glandular squamous cell carcinoma of the uterus
This is a special type of formation that tends to develop in organs with a branched system of glands. Most often, this type of cancer occurs in the uterine cavity and combines signs of squamous cell carcinoma and adenocarcinoma. Women over 55 years of age are at risk.
Tumors of the glandular squamous cell type are formed in the form of a node, which is characterized by an exophytic type of development and over time can affect the myometrium, which happens very rarely. Most diagnostic cases are clearly localized tumors that practically do not affect the entire endometrium and do not invade the parametrium and myometrium.
Glandular squamous tumors are characterized by rapid growth and a high degree of aggressiveness, which is explained by the presence of a glandular component in the formation. With an advanced form of the tumor, the risk of damage to such a distant organ as the lungs increases significantly. If this happens, a personal treatment program for the secondary tumor is developed for the patient. Israeli clinics in this case are the best choice, as they provide effective treatment of all forms of cancer at different stages at reasonable prices.
Features of endometrial cancer treatment
Treatment for endometrial cancer is based on surgical removal of the carcinoma. In addition to removing the tumor, the oncologist may decide to carry out therapy in the following ways:
- Radiation therapy;
- Chemotherapy;
- Hormone therapy.
However, to effectively combat tumors, surgical intervention is predominantly used. The scope of such assistance and methods of performing the operation are determined depending on the stage of the cancer. The surgical procedure involves complete excision of the uterus and ovaries. The principle of this operation is to remove the uterus, ovaries and fallopian tubes. This option is possible for women over 40-50 years old. If there are age restrictions for the operation, then hysteroresectoscopic ablation is performed. This method of treatment requires high precision, so it is carried out mainly in exceptional cases and in the initial stages of cancer development.
Radiation therapy is the basis of complex treatment. The principle of treatment is based on ionizing radiation or radiography. If the tumor has a low degree of differentiation, double-acting radiation therapy is used: external and intracavitary. Radiation therapy is usually given after surgery.
Chemotherapy treatment of pathology is also not used as a monotherapeutic method. After all, endometrial cancer cells are not highly sensitive to all cytostatic drugs. Often, the chemotherapy treatment regimen includes the use of cyclophosphamide, doxorubicin and cisplatin.
Hormone therapy is possible as an independent treatment method. However, it is carried out mainly in the early stages of the development of the disease. Hormone therapy includes 2 stages of treatment. At the first stage, gestagen and antiestrogen preparations are used, under the control of hysteroscopy and biopsy. One of these procedures is carried out once every 2 months. The second stage involves the use of estrogen-gestagen drugs of 1-2 generations. The duration of the first stage is 1 year, and the second is about 6 months.
It is important to know! Any treatment method is highly effective if it is used at an early stage of the development of the disease. Self-medication of endometrial cancer is strictly contraindicated and can lead to active tumor growth.
Features of surgical treatment
Cancer must be treated through surgery, which can have a high level of success.
Many patients must undergo removal of not only the uterus, but also its appendages. In some cases, lymph nodes located in the pelvis are also removed. In some cases, combined treatment is required, including surgery with radiation performed remotely and intracavitary gamma therapy. Radiation irradiation of the affected organs can be carried out before surgery, which is recommended in the third stage. Radiation therapy can be an independent technique, which is used only in cases of local spread of the oncological process and contraindications to surgery. Therapeutic agents intended to effectively fight a tumor are usually prescribed for the third and fourth stages of the disease, as well as for neoplasms that differ in differentiation. Most often, two types of treatment are successful: combined radiation therapy and extirpation of the uterus and appendages. Treatment is determined by the stage of the disease:
- At stage 1-A, which involves microinvasive oncology, it is necessary to extirpate the uterus, as well as its appendages.
- At stage 1 (the process involves only the cervix), irradiation is necessary, either remote or intracavitary. Then it is necessary to remove the uterus and its appendages. The intervention promises to be expanded. In this case, surgical intervention may be performed first, and then gamma therapy.
- At the second stage, when the disease develops in the upper part of the vagina and there is a risk of spreading to the body of the uterus, the main technique is radiation therapy. Surgery is performed extremely rarely.
- At the third stage, radiation therapy is performed.
- At the fourth stage, irradiation is necessary, but its purpose is palliative maintenance of the body.
Symptomatic treatment allows you to successfully treat the disease.
Treatment in later stages
In the later stages, removal of the uterus alone may not be enough. Since metastases are located in many organs. That is, not only the reproductive system, but also other systems are involved in the oncological process. Removal of the uterus is carried out in any case. But the further task is to get rid of metastases to other parts of the body. This is done through chemotherapy, radiation, or a combination of both.
Chemotherapy
It is not effective as a standalone treatment method. Used as part of combination therapy. Its meaning is to introduce active chemicals into the body. These drugs are toxic, causing severe symptoms.
Irradiation
It is usually prescribed for the third or fourth stage of the disease. We are talking about external beam radiation therapy on the pelvic organs. It can be used either independently or as part of complex therapy. It can be external or intracavitary. Both of these methods can be used in combination, or only one of them.
Concomitant diseases during menopause. Uterine and ovarian cancer
Natalya June 14 at 0:00 1535
During menopause and postmenopause, the risk of developing any cancer increases, so we should also mention such a disease as cervical cancer. Fear of him is one of the problems that worries women during this period. It must be said that there is no point in worrying in vain. All that is required is a regular (once a year) test that can detect the presence of atic cells, that is, cells with signs of malignant degeneration. This way, cervical cancer can be detected early. If for some reason this was not possible, this disease is curable, but only if the malignant cells have not spread beyond the surface layer.
Cervical cancer is always preceded by a painful condition caused by the papilloma virus (condyloma), which is sexually transmitted.
An advanced viral disease can cause the development of cancer.
The fewer casual partners and unprotected sexual intercourse, the greater the chance of avoiding sexually transmitted infections: papillomas (condylomas), chlamydia, mycoplasmosis, ureaplasmosis, trichomoniasis, the long-term existence of which provokes the development of cervical cancer. Despite the life experience that women at this age have, I would like to remind you once again that sex should be safe - protect yourself, and you will not be at risk of infection. Smoking also has a powerful stimulating effect on the development of atypical cervical cells and the development of cancer. Experts have proven that nicotine stimulates the occurrence of this type of cancer, as well as many others, so quitting smoking in such cases is a necessary, vital condition. The ovaries, along with the fallopian tubes and ligaments, belong to the uterine appendages. The fallopian tubes depart from the bottom of the uterus in the area of its corners and go towards the side walls of the pelvis. The fallopian tubes are oviducts, that is, the paths through which the egg enters the uterine cavity. The fallopian tube has an average length of 10-12 cm, its lumen is not the same along its entire length and reaches a maximum at the end, in the so-called funnel. From the funnel of the tube there are numerous fimbriae, thanks to the flickering movements of which, along with the contraction of the fallopian tube, the egg moves into the uterine cavity. The ovaries are a pair of granular, tonsil-shaped glands, approximately the size of a walnut, located at the ends of the fallopian tubes on either side of the uterus. They produce female sex hormones - estrogens and progesterone. In the main layer of the ovary - the cortex - there are follicles (vesicles) in which eggs mature. During the ovarian (ovarian) cycle, one of the follicles begins to grow and reaches its maximum size of 2-2.5 cm by the 13-14th day of the cycle. Such a follicle is called dominant. In the middle of the ovarian cycle, this follicle bursts, the egg that has matured in it is released into the abdominal cavity and then moves through the fallopian tube into the uterine cavity.
The growth of the follicle and the development of the egg in it occurs under the influence of estrogens, which are produced in the ovary in the first half of the ovarian cycle. After the release of an egg from a ruptured follicle (ovulation), a corpus luteum is formed in place of the latter, producing progesterone, the hormone that maintains pregnancy. It should be noted that on those days when an egg is released from a ruptured follicle, that is, ovulation, conception is most likely.
The ovaries produce eggs and female sex hormones (estrogens and progesterone), and their functioning is vital for any woman. However, by the time a woman reaches menopause, she worries about the possibility of cystic tumors and ovarian cancer. In general, cysts form in the ovaries constantly - as long as the menstrual cycle continues. The dominant follicle in which the egg matures is a benign cyst. During ovulation, the follicle ruptures and the mature egg is released into the abdominal cavity. If ovulation does not occur, the follicle may continue to grow, and thus the cyst will increase in size. Such a cyst is called functional because it is formed during the normal functioning of the female genital organs from normal tissues. It is not dangerous and usually disappears before the next menstrual cycle. But if this does not happen, problems may begin. In this case, it is better to undergo an examination to make sure that there is no danger. A cyst can also develop in the corpus luteum after the egg leaves the ovary. After the egg is expelled, the follicle does not remain empty: it is filled with blood vessels and new cells, from which the corpus luteum is then formed. As mentioned above, it is in the corpus luteum that progesterone is produced - the hormone for maintaining pregnancy.
If pregnancy does not occur, the corpus luteum shrinks, forming a tiny scar. Therefore, normally, corpus luteum does not exist for long - no more than two weeks. It’s another matter if blood gets into the corpus luteum, and this can happen if the surface of the ovary bleeds. In this case, a swollen, blood-filled cyst can exist much longer - a month, two, and sometimes even longer. Such a cyst can also disappear on its own, or it can “linger” in the body, causing trouble for the woman.
Another common type of ovarian cyst is a small tumor filled with fluid and sometimes even fat and hair (dermoid cyst). Some fill with mucus and can grow to the size of a full term pregnancy; they are called mucinous. Other cysts are caused by elements of the uterine lining and menstrual blood entering the ovary and are called endometriotic. These types of ovarian cysts are considered true, not functional, and require mandatory surgical treatment, as they can degenerate into malignant ones. Seven out of ten ovarian cysts are functional varieties and go away on their own with the start of the next menstrual cycle. If the cyst persists longer, causing pain or bleeding, or becomes too large, it should definitely be examined. Using an ultrasound examination, you can find out its type, size and features. Most ovarian cysts do not cause any symptoms, and you may not even know you have one until your doctor discovers it during a routine checkup or with an ultrasound. But if ovarian cysts become too large, they can put too much pressure on the bladder, intestines, or abdominal wall. Sometimes this causes sudden severe pain, possibly accompanied by nausea, as it erupts or twists around itself. This pain usually goes away quite quickly, but sometimes persists for a long time. In any case, you need to immediately understand the reasons for this phenomenon by contacting a gynecologist. A woman, regardless of age, should regularly check the condition of her reproductive organs. Without an examination, you may not know you have an ovarian cyst until it grows too large and causes problems. Each cyst that has not disappeared within a month (or so) after its occurrence and has grown more than 5 cm (in a woman with a preserved menstrual cycle) or more than 2 cm (in a woman of menopausal age) requires careful examination. In most cases, it is removed no later than 3-4 months after discovery, even if it turns out to be completely benign. This is done in order to avoid the possibility of its rupture or torsion and to finally make sure that it is benign. A blood test can also provide valuable information in this regard, especially in women whose menstrual cycle has already stopped. In menopausal women with positive ultrasound results and normal CA-125 test results (a so-called tumor marker for ovarian cancer), the likelihood that the cyst will be malignant is very low.
The cyst can be removed using laparoscopy (through small incisions in the umbilical area), unless it is too large or the ultrasound results are questionable. Then abdominal surgery with dissection of the abdominal wall (laparotomy) will be more likely to be chosen - so that the doctor can better examine the ovaries and adjacent organs.
Ovarian cancer is rare in women under 40, but with each passing year after this milestone, its cases become more and more frequent. This type of cancer is dangerous because in very rare cases it can be diagnosed at an early stage because it does not give any symptoms: no bleeding, no pain, no visible swelling, or other warning signs. Ovarian cancer is often discovered by chance. At an early stage, it is most often discovered during abdominal surgery, performed for completely different reasons. Later stages cause symptoms such as strange digestive disorders, bloating, and fatigue. Removal of the ovaries means the immediate onset of menopause with all its consequences - from hot flashes to osteoporosis. Moreover, these phenomena will be expressed much more clearly than during natural menopause. In case of removal of the ovaries, doctors strongly advise the use of hormone replacement therapy - this is the only way to prevent premature aging and the occurrence of problems associated with menopause. Currently, no specific causes have been identified that cause ovarian cancer. It is known that the risk of developing it is higher in women who have never been pregnant, especially if they have not used protection during sex for many years. There is also some evidence that a high-fat diet may increase this risk to some extent. A full pregnancy and the birth of a child has its own positive impact, as does breastfeeding. Pregnancy, breastfeeding, and oral contraceptives reduce the risk of ovarian cancer. A diet containing little animal fat and plenty of fibrous vegetables may also help prevent the disease. To prevent the development of ovarian cancer, it is recommended to undergo an annual examination by a gynecologist. Moreover, you should definitely bring to the attention of the doctor whether there have been cases of malignant ovarian tumors in the family history. In this case, observation will be more careful, and examinations will need to be carried out more often. S. Trofimov
medbe.ru
Stages of oncology
In total, there are 4 degrees of development of uterine cancer:
It is difficult to identify malignant manifestations at the initial stage due to the lack of pronounced symptoms.
- At an early stage, a tumor forms on the body of the organ, which affects only the upper layers of the epithelium. Due to the small size and small area of the lesion, there are no pronounced symptoms of uterine cancer, so it is difficult to recognize the pathology at the 1st stage of development.
- At stage 2, the neoplasm affects the cervix and cervical area.
- As grade 3 progresses, the malignant tumor spreads to the parametrial tissue. In addition, metastasis to nearby lymph nodes is observed. It will be more difficult to cure the disease at such a time, especially if oncology is diagnosed in old age.
- Stage 4 uterine cancer is characterized by the growth of a malignant neoplasm beyond the pelvis. Damage to the bladder and intestines is also observed. Advanced stage 4 is considered inoperable; the disease develops quickly, leading to intoxication of the entire body.
What symptoms are you worried about?
While the tumor is small in size, the disease practically does not manifest itself in any way. The first signs appear after the malignant cells of the deep layers of the organ are damaged and the formation increases in size. As endometrial cancer progresses, it has the following symptoms:
Constant pain in the lower abdomen may be a signal of an increase in the number of cancer cells and the progression of the disease.
- bleeding not associated with menstruation, in this case, blood discharge during menopause should be alerted, when menstruation should be completely absent;
- weakness, lethargy;
- causeless increase in body temperature;
- weight loss;
- lack of appetite;
- pain localized in the lower abdomen, in the lumbar region;
- inflammation and enlargement of lymph nodes;
- disruption of intestinal function if oncology progresses with metastases.
Blood discharge from cancer leads to iron deficiency anemia, as a result of which the patient complains of increased fatigue, dizziness and headaches. In addition, in such cases, an increase in heart rate and breathing is observed, thus the body compensates for hypoxia and poor circulation in the internal organs.
Causes
There are a number of factors that can trigger the disease. These include:
- the presence of gynecological diseases that were not detected and treated in time;
- disruptions in the menstrual cycle, as well as its cessation (menopause, postmenopause);
- taking medications containing large amounts of estrogen;
- the disease is hereditary. If anyone in the family suffered from this disease, then there is a high probability that one of the relatives will subsequently suffer from uterine precancer;
- prolonged absence of sexual intercourse;
- having more than one sexual partner and changing them frequently;
- repeated artificial termination of pregnancy;
- early onset of the monthly cycle (under 12 years);
- late pregnancy and childbirth. Especially if a woman carries her first child after thirty years;
- the presence of obesity, which subsequently leads to diabetes;
- alcohol abuse and long-term smoking;
- immunosuppression for one reason or another;
- ignoring visits to the gynecologist for preventive purposes;
- frequent stress;
- Strict dietary restrictions, that is, all kinds of diets, can lead to decreased immunity and hormonal imbalances in the body.
There may be several reasons for the formation of the disease, but one thing is clear: endometrial cancer is formed due to an imbalance in the hormonal background of a woman.
Life expectancy for uterine cancer
The prognosis depends on the type of tumor, stage, and the effectiveness of the treatment. At the first stage, in almost all cases, the prognosis is favorable, a cure is possible; the diagnosis will not have a noticeable impact on the length of life. With greater organ damage, the survival rate reaches 75% or more, especially if the general condition of the body is good and all doctor’s instructions are followed with maximum accuracy. Stage 4 is characterized by multiple lesions of internal organs, in which in most cases death occurs within 1-3 years.
No one can give accurate predictions about life expectancy; it depends on many factors. A woman’s moral attitude plays an important role in this. If she is determined to fight for her life and health, then the chances increase several times. And early diagnosis will help to identify dangerous changes in time and take the necessary measures.