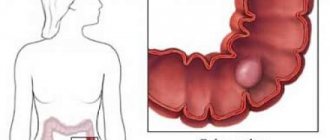
Adenocarcinoma is a malignant neoplasm of the sigmoid colon, arising from glandular epithelial tissue. Oncological disease develops in the lower part of the organ, where feces accumulate. Processed food, which releases toxins and carcinogens, comes into contact with the walls of the sigmoid colon, causing the development of glandular cancer - adenocarcinoma.
Causes
Colon adenocarcinoma belongs to the group of colorectal cancers. There are a number of provoking factors for cancer:
An unhealthy lifestyle, stress, exposure to chemicals, and poor heredity become the causes of colon adenocarcinoma.
- benign tumors or intestinal polyposis;
- unhealthy diet (lack of fiber, predominance of fatty, spicy foods, fast food);
- smoking, alcoholism;
- frequent contact with household chemicals;
- work at a chemical enterprise;
- heredity;
- constant stress;
- fecal stones, constipation;
- ethnic characteristics (belonging to the group of Eastern Europeans and Central Asians);
- low mobility during the day.
Malignancy caused by a mutation in intestinal cells can be provoked by any factors associated with motor dysfunction of this department or circulatory disorders. As a result of these processes, stagnation of food masses occurs, which creates favorable conditions for malignancy. Disease provocateurs that cause a precancerous condition:
- ulcerative colitis;
- inflammation of the gastrointestinal tract (Crohn's disease);
- diverticulitis;
- polyposis
Stages of the disease
According to the international classification, the following stages are distinguished:
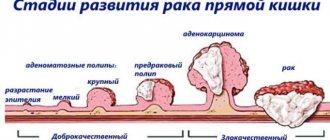
- 0 – the formation is small, does not increase in size, there are no metastases.
- 1st - up to 2 cm, does not extend beyond the mucous membrane.
- 2nd - can increase up to 5 cm, grows into the intestinal wall.
- 3rd – spreads to nearby organs, affecting the lymph nodes.
- 4th – metastases appear in distant organs.
https://www.youtube.com/watch?v=ffr-sE0Fpm0
Metastases to organs can spread: through the lymph flow, through the bloodstream, or with direct tissue damage. In colon cancer, metastasis occurs according to the following scheme: lymph nodes - liver - lungs - bone tissue.
Adenocarcinoma of the rectum develops gradually. At the first stage, it is very difficult to suspect pathology; the symptoms are very weak. However, damage occurs to the mucous and submucosal tissues of the large intestine.
In the second stage, the tumor begins to penetrate the intestinal muscle tissue. The malignant formation protrudes 1 cm into the inner part of the intestinal lumen. Gradually, these parameters increase, and the patient begins to worry about constipation.
The third stage is characterized by more extensive lesions. The tumor formation affects the entire intestinal wall, while the lymph nodes are not affected, but over time, metastases begin to penetrate into the lymph nodes. The malignant tumor grows in the tissue of the serous membrane, where the nerve fibers are located, so the patient begins to experience excruciating pain.
The fourth stage is characterized by many metastases, the lymph nodes are first affected, then nearby organs begin to suffer.
Adenocarcinoma of the rectum can be provoked by the following factors on the human body:
- smoking;
- stress;
- obesity;
- inactive lifestyle;
- hereditary predisposition;
- poor nutrition;
- bad ecology;
- consumption of carcinogenic products;
- contact with heavy metals;
- infection with oncogenic viruses;
- the presence of a focus of chronic bacterial infection;
- traumatization;
- previous surgery;
- precancerous diseases;
- long-term inflammatory process;
- intoxication;
- lack of vitamins;
- autoimmune process;
- constipation or diarrhea;
- disruption of antitumor protection;
- alcoholism.
Classification
Colon adenocarcinoma comes in several types:
- Mucinous form, when the neoplasm includes mucus and epithelial cells. Mucinous cancer is characterized by:
Colon adenocarcinomas come in varying degrees of damage to tissues, cells, and neighboring systems.
- unclear boundaries;
- metastases to nearby lymph nodes;
- increased recurrence;
- resistance to radiation.
- Signet ring cell form. It is one of the most aggressive types, as it is detected when metastases are present in the liver and lymph nodes. Characterized by:
- germination inside the intestine;
- affects young people.
- Squamous form, formed from flat cells of the anal canal. Characterized by:
- high degree of malignancy;
- germination into the bladder, prostate, vagina;
- low survival rate;
- high recurrence.
Mortality is more than 50% of patients within 3 years. There is a standard classification according to which they distinguish:
- highly differentiated;
- moderately differentiated;
- low-grade;
- undifferentiated;
- tubular cancer.
Highly differentiated
Highly differentiated formations in the colon do not change the structure of cells and have a favorable outcome.
Well-differentiated colon adenocarcinoma is characterized by unchanged cellular structure, but with elongated nuclei. The cells are similar to healthy ones, since they do not change their composition and fulfill their purpose. The outcome is usually favorable.
If adenocarcinoma is diagnosed in an elderly patient, metastases are rarely found in regional organs. In young people, relapses occur more often, so after surgery to remove mucinous cancer, the 5-year survival rate is 50%.
The difficulty of diagnosis lies in the slow progression and similarity of cancerous and healthy cells.
Moderately differentiated
Moderately differentiated adenocarcinoma of the colon is characterized by serious consequences due to the rapid proliferation of malignant epithelial cells, causing intestinal obstruction. Large tumors rupture the intestinal wall, causing severe bleeding. The course of cancer is aggravated by the risk of fistula formation with peritonitis.
Treatment is effective only in the early stages. In this case, surgery in combination with radiation and chemotherapy gives a good result. Severe mucinous cancer always affects nearby organs.
Poorly differentiated
Poorly differentiated colon adenocarcinoma is characterized by extensive cell mutations.
Poorly differentiated adenocarcinoma of the colon is aggressive, characterized by strong cellular polymorphism with early spread to nearby organs. Cellular cancer is characterized by:
- lack of boundaries;
- unfavorable outcome.
At an early stage, surgery to remove the tumor followed by therapy can achieve long-term remission . The poorly differentiated type occurs in 20% of cancer patients.
Undifferentiated
The anaplastic or undifferentiated form is characterized by cells atypical for cancer, which are difficult to attribute to the available histological types. Cancer is characterized by:
- infiltrative growth;
- very early metastasis to regional lymph nodes;
- extremely disappointing prognosis with minimal likelihood of successful treatment.
Tubular
Tubular adenocarcinoma in the colon is difficult to diagnose and provokes hypersecretion of mucus.
This form of adenocarcinoma is not diagnosed due to the absence of symptoms in the initial stages, but can be discovered incidentally. The tumor is characterized by:
- implantation into fibrous stroma;
- branching structure;
- cylindrical or cubic cells.
As it progresses, hidden bleeding develops with signs of anemia. When the right conditions occur, the mucinous tumor begins to produce large amounts of mucus enriched in cancer protein and potassium, which causes hypokalemia and hypoproteinemia. The cancer is difficult to treat and the prognosis is poor.
Glandular cancer
This type of cancer is divided into four types. Here's how it's presented:
| Mutationous | In this case, the tumor has no defined boundaries. Metastases pass to the lymphatic system. Radiotherapy does not work, so relapse rates are high |
| Cricoid cell | In this case, there is high aggression in its course. If a person becomes ill and consults a doctor, then usually there are metastases in the lymph and liver. Usually young people suffer from this disease, in this case the entire organ suffers. |
| Squamous | This tumor forms in the anus and consists of flat epithelial cells. In this case, people live up to three years; no more than thirty percent live to five. This happens due to the high mortality rate in this type of disease, because the disease has a high rate of relapse |
| Tubularity | In this case, the presence of tubular structures of the tumor leads to the fact that although the contours are blurred and the formations themselves are small, after surgery patients feel better in fifty percent of cases |
Symptoms at different stages
The early stage of adenocarcinoma is nonspecific and uncertain. Frequent patient complaints:
- periodic pain in the abdomen;
- alternating constipation with diarrhea;
- refusal to eat;
- nausea.
Bloody and mucous inclusions in the stool may appear, which, as the disease progresses, are replaced by purulent ones.
Immediately the symptoms are constant, but not pronounced. As it progresses, the symptoms increase. A growing tumor can be felt through the abdominal wall. It will take the form of a dense, lumpy compaction with high mobility. General clinical picture:
- paroxysmal aching pain in the lower abdomen;
- poor appetite due to constant nausea;
- rapid weight loss;
- weakness, fever;
- changeable stool;
- flatulence, difficulty with bowel movements;
- pale skin;
- blood, mucus and pus in the stool.
As the mucinous tumor grows, gastric disorders appear in the form of a feeling of heaviness, constant heartburn, and vomiting. The pain is increasing. Due to constant irritation of the tumor by fecal matter, it ulcerates, which provokes infection. As a result, symptoms of intoxication appear:
- heat;
- quantitative and qualitative changes in blood;
- pain in the lower back due to the spread of infection into the retroperitoneal tissue.
Signs of peritonitis appear.
Main symptoms
In the early stages of the onset of pathology, pronounced signs are not observed. The disease can be detected only through instrumental research. Severe symptoms of sigmoid colon cancer, coinciding with signs of pathology of the gastrointestinal tract and abdominal organs, appear in the last stages of development.
The main signs of adenocarcinoma are:
- Stage I: flatulence, gas formation, rumbling in the stomach, unstable stool (a series of diarrhea and constipation);
- Stage II-III: excretion of feces mixed with pus, blood and mucus, cramping pain in the left side of the ileum, belching, nausea, severe vomiting;
- Stage IV: exhaustion, increased liver volume, development of jaundice, anemia.
Internal damage to the colon leads to pain due to partial blockage of the lumen by cancerous tumors. Dyspeptic disorders are characteristic oncological symptoms of adenocarcinoma. Cancer intoxication in the final stages leads to weakness, fatigue, decreased appetite, weight loss, high fever, and increased abdominal circumference. Colon adenocarcinoma is the cause of the development of abscesses of the abdominal organs.
Diagnosis of colon adenocarcinoma
Detection of adenocarcinoma occurs in several stages using a large number of methods:
- Examination, history taking, analysis of patient complaints, external palpation.
- General tests of blood, urine, feces.
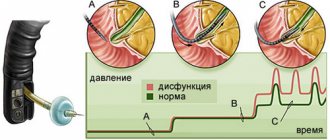
- Digital and endoscopic (sigmoidoscopy) rectal examinations, which provide results in the early stages of cancer detection.
- X-ray with contrast. The method allows you to determine:
- changes in relief in the intestinal mucosa;
- incorrect filling;
- expansion of the wall over the pathological protrusion;
- strengthening motor skills.
- Endorectal or transcutaneous ultrasound. Ultrasound allows you to identify the tumor focus and distant metastases.
- Endoscopic biopsy with collection of biomaterial from affected tissues for analysis. The type, degree, stage, differentiation of cancer in histological preparations is determined.
- Colonoscopy. The method allows you to visualize a tumor regardless of its location in the colon.
- MRI and CT make it possible to determine the structure and localization of tumor formation, assess the level of damage to nearby organs, and see distant metastases.
Adenocarcinoma requires differential diagnosis with polyps, diseases of the kidneys, liver, ovaries, spleen, and ureter.
Diagnostic methods
To identify adenocarcinoma of the sigmoid colon, basic diagnostic methods are prescribed, including laboratory tests and instrumental examination:
- sigmoidoscopy;
- colonoscopy;
- irrigoscopy;
- ultrasound examination, magnetic resonance imaging of the intestine.
The first way to diagnose the disease is to donate blood for a general, biochemical analysis, and collect stool to detect internal effusion. A cause for concern is a decrease in protein content, hemoglobin concentration and an increase in haptoglobin.
During the consultation, the doctor performs a manual examination - palpation. The procedure involves maximum palpation of the abdominal organ.
One of the main diagnostic methods is sigmoidoscopy, a feature of which is a visual examination of the sigmoid colon using a probe with an optical camera. The structure of the device allows you to assess the condition of the surface of the mucous membrane and collect cells for laboratory tissue analysis. Colonoscopy involves inserting a device through the anus to examine the entire large intestine and take biological material for testing for tumor markers.
Irrigoscopy - radiography using barium sulfate. The introduction of a contrast agent makes it possible to identify the localization zone, the nature of the malignant neoplasm, and establish a possible narrowing of the intestinal lumen. Ultrasound examination and magnetic resonance imaging give an idea of the possible spread of metastases and the tumor process to the lymph nodes. Colonoscopy is contraindicated for patients with intestinal diverticulosis, so MRI is the only approved diagnostic method for identifying the etiology of the pathology.
Treatment
The therapeutic regimen for colon adenocarcinoma is determined by stage and form. A combined technique is usually used:
- Radiotherapy is used to reduce tumor size and improve the quality of surgery by reducing the risk of tissue inflammation and cancer cells entering the bloodstream.
- Chemotherapy. The following drugs are used:
Colon adenocarcinomas are eliminated through complex therapy with tablets, hardware treatment, folk remedies, and diet.
- 5-fluorouracil, Leucovorin, Irinotecan;
- "Capecitabine", "Ftorafur", "Raltitrexid".
- Diet therapy based on enriching the menu with fresh fruits and vegetables, vitamins, and drinking plenty of fluids.
- Treatment with folk remedies is necessary as an auxiliary measure, but requires consultation with a doctor. Popular recipes:
- A mixture of 25 g of calamus root, 90 g of potato flowers, 35 g of calendula, 100 g of wormwood root in 500 ml of boiling water. The product is infused for 6 hours. Drink 100 ml before meals.
- Therapeutic enema with water and copper sulfate (100 ml of concentrate in 2 liters of water). Course - 2 weeks.
- 25 g of celandine in 250 ml of boiling water. The product is infused for half an hour. Drink 25 ml three times a day before meals.
- Gopher fat. There are 100 g distributed throughout the day. You can cook food on it.
Clinical picture
As a rule, the clinical picture of the disease is represented by symptoms of acute intestinal obstruction, which develops when the tumor completely or partially blocks the lumen of the sigmoid colon. This condition is characterized by the following symptoms:
- Lack of gas and bowel movements . If the tumor develops over a long period of time, the patient may have a tendency to become constipated and may pass small amounts of blood or mucus in the stool.
- Nausea and vomiting . Symptoms characterize the late stages of the oncological process, when the tumor completely blocks the lumen of the intestine and its contents cease to pass through the digestive tract.
- General weakness , malaise, weight loss and loss of appetite almost always accompany patients diagnosed with adenocarcinoma of the sigmoid colon.
Metastasis
Adenocarcinomas metastasize to nearby and distant tissues, organs, and lymph nodes in the early stages. There are three ways cancer spreads:
- lymphogenous (through the lymph nodes, occurs in 60% of cases);
- hematogenous (through blood, occurs in 10% of cases);
- implantation (when the tumor comes into contact with healthy tissues, occurs in 30% of cases).
If adenocarcinoma has spread to nearby tissues, isolated metastasis may not occur. Most often, cancer cells affect the liver, regional lymph nodes, and less often the lungs and pelvic bones.
Adenocarcinomas of the colon can be complicated by fistulas, peritonitis, obstruction, tissue rupture, and infection of neighboring organs.
Where do metastases penetrate?
They can affect other organs. Cancer cells spread to them through the bloodstream. The appearance of malignant cells in the lymph nodes is also likely. Penetration of cancer cells through the bloodstream occurs in 10 percent of cases.
Metastases significantly aggravate the prognosis of the disease. With metastasis, other complications arise:
- bleeding that is difficult to treat;
- addition of a secondary infection;
- cachexia;
- intoxication of the body with tumor decay products;
- perforation of the affected area of the intestine;
- partial or complete obstruction.
Forecast
The outcome of colon adenocarcinoma depends on:
- stage and type of disease;
- depth of tumor germination;
- prevalence;
- presence and number of metastases.
About half of people have a favorable outcome after treatment for colon adenocarcinoma.
The next 5 years after surgery are critical due to the possibility of relapse. A survival rate of more than 90% is allowed with radical removal of most of the rectum. With metastasis to the lymph nodes, the survival rate is 50%. The outcome depending on the type of differentiation is as follows:
- The highly differentiated form is characterized by a favorable prognosis with a 5-year survival rate of more than 50% in elderly patients, 40% in young patients.
- The moderately differentiated form is practically incurable due to the difficulty in selecting effective chemotherapy drugs. The operation is effective with proper concomitant treatment.
- The poorly differentiated form is the most dangerous due to its aggressiveness and high germination rate. The outcome is less favorable.
How does the pathology manifest itself?
In the presence of the disease, factors such as a constant feeling of insufficient bowel movement and tenesmus appear.
Colon adenocarcinoma combines the following clinical symptoms:
- Asthenization of the body. Patients experience constant weakness, drowsiness, weakness and depression.
- Diffuse pain in the abdominal cavity. More often it is localized to the right and left of the navel.
- Feeling of insufficient bowel movements. No matter how many times a person goes to the toilet, he always wants to visit the team again.
- Lack of appetite. The patient begins to feel a particular disgust for meat products.
- Rapid weight loss. Patients lose tens of kilograms of weight within six months or even several months.
- The presence of a large amount of mucus and blood in the stool. Unlike stomach bleeding, the discharge here does not change color.
- Tenesmus. This term refers to painful sensations, cramps and the urge to defecate in the absence of feces.
- Persistent low-grade fever. The temperature rarely exceeds 38 degrees Celsius, but lasts for a long time.
Nutrition
The success of rehabilitation depends on the correct organization of postoperative nutrition. The basic rules of diet therapy are as follows:
- Food should be fresh, easily digestible, enriched with vitamins, plant fiber, and micronutrients.
- Food should not provoke nausea and flatulence.
- The composition of the dishes should facilitate the ease of excretion of feces. A vegetarian diet is recommended. It is possible to consume small amounts of rabbit and turkey meat.
- Meals should be fractional and portions should be small.
- Food should be consumed warm.
- Preferred culinary processing is boiling, steaming.
- You should eat slowly and thoroughly chew, which increases salivation and improves digestion.
- Drinking should be plentiful.
- Exclusion from the menu of foods that promote fermentation, such as legumes, dairy products, yeast bread, alcohol.
Diet
A proper diet for adenocarcinoma is one of the factors that increases the effectiveness of treatment. Patients diagnosed with glandular cancer should eat fresh and easily digestible foods that contain plenty of vitamins, minerals and nutritional components.
All food consumed should be “light” so that there are no delays in the stomach, as this can cause attacks of nausea and increased gas formation. It is worth noting that the structure of all dishes consumed should improve the excretion of feces. All types of foods that can cause fermentation should be excluded from the patient’s diet:
- beans;
- dairy products;
- alcohol;
- yeast types of bread.
It is recommended to eat lean meats.
Approximate menu
- On an empty stomach:
- non-carbonated mineral water with lemon juice.
- Breakfast:
- vegetables and fruits (separately or in combination);
- nuts;
- 100 ml low-fat kefir.
- Dinner:
- weak chicken soup;
- a fresh vegetable salad;
- boiled fish.
- Afternoon snack:
- non-concentrated fruit juice;
- whole grain biscuit.
- Dinner:
- vegetable stew;
- sprouted vegetable grains;
- pasta.
- Nighttime snack:
- juice from vegetables or fruits.
Symptoms of the disease
Adenocarcinoma is a dangerous disease. This is due to the fact that in the initial stages, when the tumor is formed, there are no symptoms. But even when cancer begins to manifest itself, the symptoms are so general that it is difficult to attribute them to the intestines. Therefore, in the early stages of the disease, the correct diagnosis is rarely made. The first symptoms of adenocarcinoma are weakness, fatigue, pallor, and sometimes nausea and abnormal bowel movements. Later they are joined by lack of appetite and weight loss.
At later stages of the disease, symptoms appear that indicate the focus of the tumor. Among them are impurities in feces and intoxication of the body. As a result, the patient's liver becomes enlarged and the skin appears yellow. If after such symptoms the disease is not treated, then bleeding and intestinal obstruction occur.
The danger of poorly differentiated adenocarcinoma
The best results can be achieved with a highly differentiated tumor at the initial stage of formation. The diagnosis is determined based on the results of the above tests. Treatment is selected individually for each case and depends on the degree of development of the oncological process, differentiation, area of damage and the presence of secondary foci.
After the operation, a course of chemotherapy is prescribed. It finishes off malignant cells in all systems and organs. By introducing itself into cancer DNA, the drug stops cell division and prevents its spread. Treatment is prescribed in courses because the drugs used negatively affect healthy cells.
Radiation therapy affects the tumor site with absolute precision. Like chemotherapy, it is used in preparation for and after surgery. Ionizing radiation slows down the growth of atypical cells and destroys their structure. In the postoperative period, rays have a positive effect on wound healing and relieve pain.
Immunotherapy involves taking drugs to activate the body's natural defenses.
For inoperable rectal adenocarcinoma, the patient is prescribed palliative treatment, including radiation and chemotherapy. The task of doctors is to slow down the oncological process, relieve symptoms of intoxication and prolong the patient’s life.
Poorly differentiated adenocarcinoma usually has a very rapid, often fulminant course. And it is she who is very difficult to treat. In turn, well-differentiated adenocarcinoma of the sigmoid colon has a very good therapeutic response, in particular to conservative measures.
It is very important to distinguish such tumors by stage:
- At the first stage, the tumor spreads only in the mucous and submucosal part of the intestine. There are practically no clinical manifestations of this disease.
- In the second stage, the cancer begins to penetrate the muscular lining of the intestine. This already affects the general condition of a person and, in particular, the functioning of the digestive tract. Already at the second stage, adenocarcinoma reaches five centimeters in diameter.
- At the third stage, adenocarcinoma penetrates all layers of the intestine. Spread (metastases) to other organs is not observed at this stage.
- The fourth stage indicates the advanced stage of the cancer process. Most often, such a tumor penetrates into neighboring tissues - the liver and other organs of the abdominal cavity.
Moderately differentiated sigmoid colon carcinoma is a type of glandular cancer. Occupies an intermediate position between highly differentiated and poorly differentiated cancer. The reasons for the development of such intestinal damage are quite difficult to determine, since this disease is multifactorial.
You need to pay attention to the following signs:
- Aching pain in the abdominal area;
- Unpleasant sensations in the oral cavity;
- Belching, nausea, vomiting and other signs of dyspepsia;
- The appearance of blood and mucus in the stool;
- Decreased appetite;
- In some cases, the patient develops hyperthermia, or fever.
The lower the degree of cell differentiation, the less chance the doctor has for treatment. It happens that a surgical operation is the trigger after which metastases develop in the patient’s body.
First of all, the danger of such a disease is that tumor cells have a high degree of aggressiveness. The tumor is growing very quickly. And it often happens that the time elapsed from identifying the disease to the start of treatment is no longer enough to achieve a high therapeutic effect.
The doctor should pay special attention to the methods of diagnosing and treating such a tumor so that surgery does not provoke a metastatic process. That is why often with such a diagnosis, the doctor does not recommend surgery to his patients. Other treatment methods are suitable for the patient, in particular radiation or chemotherapy.
The easiest way to determine if a person has a tumor is to palpate it. You can study the condition of the sigmoid colon in more detail through colonoscopy, an unpleasant but very informative procedure with which a doctor can determine whether a patient has cancer.
For diagnosis, fluoroscopy of the sigmoid colon is used. This procedure is also called irrigoscopy. X-ray diagnostics are used using a contrast agent. This way, a specialist can determine not only the presence of a tumor-like body in the body, but also the contour, thickness of the intestine, relief of the mucous membrane and other features.
For this diagnosis, the doctor does not use harmful x-rays. MRI makes it possible to determine the presence in the intestine not only of the formation itself, but also of its source and type.
Treatment of this disease must necessarily take place in several stages. The first stage involves complete removal of the malignant neoplasm. For normal results, approximately 0.7 meters of intestine is removed. If the patient had intestinal obstruction, then the closest part of the intestine is brought out with the further use of a colostomy bag.
Chemotherapy can be prescribed after the first intervention. It is also indicated for poorly differentiated types of tumor. The goal of chemotherapy is to prevent the development of relapses. As an alternative to chemotherapy, radiation treatment is prescribed. Its purpose and therapeutic effects are similar.
In advanced cases, patients are provided with palliative care.
Treatment of adenocarcinoma of the sigmoid colon is carried out using conservative methods and surgery. Chemotherapy is given after or before intestinal surgery to reduce the size of the tumor. After surgery, residual cancer cells and metastases are destroyed using various drug regimens.
During the operation, part of the sigmoid colon is resected. Adenocarcinoma develops slowly. In the early stages, metastasis is unlikely, so an operation is performed that will help to completely cure and require resection of only a small part of the intestine. Surgery at later stages may reduce the risk of complications.
Chemotherapy
Treatment of bowel cancer with chemotherapy
Chemotherapy for adenocarcinoma of the sigmoid colon may include the following treatment regimens:
- After the operation, systemic chemotherapy is prescribed: 5-FU 450 mg/m², intravenously for 5 days, once a week for a year Levamisol 150 mg/day, 3 days, every two weeks for a year.
- Antitumor drugs are combined with biomodulators: 5-FU, Leucovorin, Interferon-alfa2b.
Chemotherapy can be carried out according to regimens used for adenocarcinoma of the colon and other parts of the intestine. If inoperable or advanced adenocarcinoma of the sigmoid colon is detected, chemotherapy treatment will not completely destroy the tumor, but will slow its growth. In any case, removal of adenocarcinoma of the sigmoid colon is necessary.
The disadvantage of chemistry is the unpredictability of results and pathological side effects. These factors have become a topic of debate among researchers about the advisability of using chemistry for adenocarcinoma of the sigmoid colon. On the other hand, chemistry accelerates the fight against metastases affecting the liver and other organs.
Complex and combined treatment includes exposure to chemicals and radiation; the following are prescribed: 5-fluorouracil, telegram therapy, Fluorouracil. The mass of the tumor is significantly reduced, and the frequency of complications after surgery does not increase. However, it is impossible to completely remove all lymph nodes in areas of metastasis.
An approximate protocol for prescribing a chemotherapy regimen for adenocarcinoma of the sigmoid colon:
- Capecitabine (Xeloda), 1000 mg/m², orally 2 times a day, days 1-14;
- Oxaliplatin 130 mg/m², intravenously, 1 day;
The interval between courses is 2-3 weeks.
- Fluorouracil 400 mg/m² infusion, then 600 mg/m² drip for 22 hours, on days 1 and 2;
- Leucovorin 200 mg/m² intravenously before fluorouracil on days 1 and 2;
- Oxaliplatin 85 mg/m² intravenously on day 1.
The interval between courses is 2 weeks.
- Irinotecan 200 mg/m² intravenously, on day 1;
- Oxaliplatin 85 mg/m² intravenously, on day 1;
The interval between courses is 3-4 weeks.
- Fluorouracil 425 mg/m² intravenously on days 1-5;
- Leucovorin 20 mg/m² intravenously on days 1-5;
The standard first-line chemotherapy regimen for colon cancer, including sigmoid colon, may include one of the following regimens: FOLFOX (5-FU, Leucovorin, and Oxaliplatin) or FOLFIRI (5-FU, Leucovorin, and Irinotecan). If Bevacizumab (Avastin), a monoclonal antibody, is added, then it cuts off the supply of nutrition to the tumor, and by suppressing the growth of blood vessels (anti-agionesis), survival improves.
Treatment with monoclonal antibody drugs is also used: Cetuximab (Erbitux) and Panitumumab (Vectibix). They target epidermal growth factor receptor (EGFR) inhibition and improve survival when treated alongside chemotherapy if patients do not have a RAS mutation.
Complications
Concomitant pathologies of moderately differentiated adenocarcinoma appear mainly in the late stages of the malignant process and the tumor is localized in any organ. First of all, they are associated with its growth. Increasing in size, adenocarcinoma begins to exert excess pressure on neighboring tissues - nerve endings, blood vessels and organs, causing pain, problems with blood flow and other disorders.
https://www.youtube.com/watch?v=iRyspsTsEY0
The specific stage of the oncological process also has a negative effect on the pathology. We are talking about metastases, relapses of the malignant process, general cancer intoxication and deterioration of the patient’s well-being.