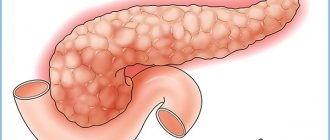
Pseudotumorous pancreatitis, or pseudotumoral, is one of the forms of chronic inflammation of the pancreas. The name of the pathology is due to the similarity of the symptoms of the disease with signs of parenchymal gland cancer. With pseudotumor pancreatitis, as in the case of a malignant tumor, the organ grows unevenly and its echogenicity changes; The patient's skin acquires a yellowish tint, and obstructive jaundice develops.
Hypertrophied areas compress the ducts, which leads to even greater disruption in the functioning of the organ and digestive processes in general. The pathology is most often diagnosed in smoking men over 40 years of age who regularly drink alcohol. But in recent years, gastroenterologists have noted a trend towards an increase in the number of patients diagnosed with “Chronic pseudotumor pancreatitis” among all population groups.
Content
Definition and general information [edit]
Acute pancreatitis is a systemic disease characterized by acute inflammation of the pancreas. Based on the pathological picture, two forms of acute pancreatitis are distinguished: edematous (interstitial) and hemorrhagic (pancreatic necrosis).
Etiology and pathogenesis[edit]
A. Trauma: blunt, penetrating; damage during surgery.
b. Infections caused by Mycoplasma spp., mumps, Coxsackie B, rubella, measles viruses; septic shock.
V. Systemic diseases: diabetes mellitus, SLE, periarteritis nodosa, uremia, hypercalcemia, hemorrhagic vasculitis, Reye's syndrome, inflammatory bowel disease, cystic fibrosis.
d. Exposure to drugs and toxic substances: azathioprine, thiazides, sulfonamides, furosemide, tetracycline, corticosteroids, asparaginase, ethanol.
d. Disorders of the outflow of pancreatic secretions
1) Congenital: absence of the pancreatic duct, absence of the common bile duct, stenosis of the papilla of Vater, accessory pancreatic duct, common bile duct cyst.
2) Acquired: trauma, cholelithiasis, tumors, false cyst, infection of the ducts, ascariasis.
e. Hereditary diseases: hyperlipoproteinemia (types I and V), hyperparathyroidism.
and. Other causes: postoperative pancreatitis, graft-versus-host disease, ulcer penetration, idiopathic pancreatitis.
Clinical manifestations[edit]
The clinical picture includes abdominal pain, nausea, vomiting, fever, intestinal obstruction, and shock. In addition, the disease can manifest itself as prolonged pain in the upper abdomen and pain in the epigastric region, ascites.
Acute pancreatitis, unspecified: Diagnosis[edit]
Examination and diagnosis
A. Amylase and lipase activities in serum and urine are measured. An increase in the activity of these enzymes indicates pancreatitis, but does not allow a final diagnosis to be made.
b. The activity of liver enzymes (AST, ALT, alkaline phosphatase) is determined.
V. A complete blood count is performed and serum levels of BUN, creatinine and electrolytes are determined.
d. Monitor blood glucose and calcium levels.
d. Ultrasound and CT are performed.
f. Chest radiography is indicated to detect pleural effusion and pulmonary edema.
Differential diagnosis[edit]
Acute pancreatitis, unspecified: Treatment[edit]
A. Eliminate hyperglycemia and water-electrolyte imbalance (hypovolemia, hypocalcemia).
b. Give total parenteral nutrition through central or peripheral veins until amylase activity decreases and pain resolves.
V. For pain relief, pethidine is administered intravenously every 3-4 hours (see Chapter 1, paragraph III.B.3).
d. To reduce stimulation of the pancreas and prevent paralytic ileus, the contents of the stomach are aspirated through a nasogastric tube.
d. Anticholinergics, antacids, and H2 blockers are sometimes prescribed, although the effectiveness of these drugs has not been proven.
e. The patient is closely monitored in order to identify signs of respiratory and renal failure in time.
and. One should remember about the possibility of late complications - false cyst and pancreatic fistula.
Prevention[edit]
Other [edit]
In Atlanta in 1992, at the International Conference on Acute Pancreatitis, it was decided to distinguish two forms of septic pancreatic necrosis:
• pancreatic (pancreatogenic) abscess is a limited accumulation of pus near the pancreas without or with a small amount of necrotic tissue.
Names used in clinical practice: pancreatogenic abscess, postematous acute pancreatitis, abscessing acute pancreatitis, pancreatic abscess, gangrenous acute pancreatitis, purulent-hemorrhagic pancreatitis, purulent-infiltrative pancreatitis, purulent-necrotic, purulent, diffuse purulent, phlegmonous pancreatitis, etc.
Pancreatogenic abscess occurs as a late complication of severe pancreatitis, usually no earlier than 4-6 weeks from the onset of the disease.
A pancreatogenic abscess can form both in the pancreas and in the omental bursa, retroperitoneal space, and abdominal cavity. The purulent cavity is limited by the infected walls of nearby organs. Pancreatic abscesses are small, sometimes multiple, and can be localized in any part, but mainly in the tail area. More often there is an abscess of the omental bursa. Infection of pseudocysts is characterized by a limited accumulation of pus. An abscess is an encysted collection of pus containing a small amount of necrotic tissue. Necrotic changes in the gland and retroperitoneal tissue are minimal.
One of the most common diseases of the digestive system is acute pancreatitis. Often this pathology requires emergency care. The development of the disease is based on the self-digestion of the pancreas with its own enzymes. The main risk factors for the development of pancreatitis are poor nutrition and alcohol intoxication.
The process of digesting food is very complex. To ensure it, the coordinated work of many organs (esophagus, stomach, intestines, liver) is required. Enzymes are needed to digest proteins, fats and carbohydrates. They are produced by pancreatic cells. Acute pancreatitis in children and adults is an inflammatory disease accompanied by swelling of the organ and the development of necrosis.
The purulent form of this pathology is the most dangerous. If not treated promptly, it leads to pancreatic necrosis. This is a dangerous condition that can cause sepsis, peritonitis and even death of the sick person. Among acute pathologies of the abdominal organs, pancreatitis ranks third in prevalence, second only to appendicitis and cholecystitis.
Every year, up to 800 new cases of this pathology are diagnosed per 1 million people worldwide. Males get sick more often.
This is due to an addiction to alcoholic drinks, spicy and fatty foods. The highest incidence rate is observed in the age category from 30 to 60 years. Recently, the number of patients has increased significantly. The ICD-10 code for this pathology is K85.
Therapy methods
Treatment of pseudotumorous pancreatitis is carried out in the gastroenterology department. The patient is prescribed a diet (table No. 5) , in severe cases - therapeutic fasting for several days. Drug therapy does not achieve recovery; it is used to alleviate the patient’s condition or as a preparatory step before surgery.
Conservative treatment
Pharmacological drugs for the treatment of pseudotumor pancreatitis are used to compensate for pancreatic insufficiency:
- Enzymes. The patient is prescribed to take pancreatin in combination with lipase.
- Antacids. The drugs help neutralize aggressive hydrochloric acid, which normalizes stool.
- Calcium preparations . Combined use with antacids eliminates steatorrhea (“fatty” feces).
- Antispasmodics . They are taken to relieve spasm from the pancreatic ducts, which improves the outflow of its secretions.
- Antibiotics. Antibacterial therapy is carried out during the acute phase.
- Painkillers . They help relieve pain and improve the patient’s well-being.
Surgical method
In cases where there is a significant enlargement of the head of the pancreas with compression of the common bile duct, the only way to eliminate the cause of the pathology and obtain stable remission is surgery.
Attention! Some patients with pseudotumor pancreatitis refuse surgery in favor of conservative treatment methods. Such a decision can only worsen the situation, because... Long-term use of medications will create additional stress on the liver, but will not bring healing.
The surgical method of therapy involves excision of the affected tissue and drainage of the pancreatic ducts.
Modern advances in medicine make it possible to obtain the desired results using minimally invasive techniques.
It is quite difficult to say exactly how long the recovery of a patient with pseudotumor pancreatitis after surgery lasts.
The duration of the recovery period directly depends on the severity of the disease, the age of the patient and other individual characteristics of the patient.
Important! The patient must strictly adhere to the doctor’s recommendations and diet throughout his life!
Types of acute forms of pancreatitis
The disease can be primary or secondary. In the latter case, the inflammatory process is caused by pathology of other digestive organs (liver, gall bladder). Every second acute pancreatitis is associated with cholecystitis. There are edematous (catarrhal) and necrotic forms of the disease. The difference is that in the first case there is no mass death of gland cells.
Pancreatic necrosis can be sterile or infected. There are also mild and severe degrees of the disease. In the first case, the prognosis is more favorable, since other organs and systems are practically not involved in the process. In severe cases, complications develop. Sterile pancreatic necrosis can be focal or widespread. There are fatty, mixed and hemorrhagic forms of this pathology. There are also drug-induced pancreatitis.
https://youtu.be/qwyTTwcpt3o
Symptoms of acute and chronic cholecystopancreatitis
The first symptom of the disease will be severe pain on the right side of the abdomen, under the ribs. As the inflammatory process spreads, the pain will spread to the back and become girdling, which is characteristic of pancreatitis. The man feels unwell and vomits. If urgent measures are not taken, the most undesirable consequences are possible. Cholecytopancreatitis, unfortunately, has a fairly high mortality rate.
Lack of medical care can lead to damage to nerve fibers, blockage of the bile ducts, and vein thrombosis. All these complications are fraught with an extremely serious condition – peritonitis.
The gastroenterologist reveals the following clinical picture:
- bloated stomach;
- constipation and loose stools alternately;
- belching;
- dryness and bitterness in the mouth;
- skin itching;
- dehydration.
Tests show signs of diabetes.
Why does the gland become inflamed?
The development of acute edematous pancreatitis in women and men is caused by different factors. The following causes of gland damage are distinguished:
- drinking alcohol;
- intoxication;
- eating fatty or fried foods on an empty stomach;
- abdominal injuries;
- cholelithiasis;
- overdose of certain medications (Tetracycline, Metronidazole);
- hyperparathyroidism;
- high levels of calcium in the blood;
- hepatitis;
- viral infections;
- mycoplasmosis;
- pancreatic surgery;
- congenital disorders of organ development;
- cystic fibrosis;
- gastroduodenitis.
The diagnosis of acute pancreatitis is very often made in people with alcohol dependence. The cause may also be a single intake of alcohol in a high dosage.
Its consumption on an empty stomach and combination with fatty foods have a particularly negative effect on the pancreas. Many young people like to drink beer and snack on chips.
The combination of alcohol with animal and vegetable fats quickly leads to pancreatitis. Every fifth case of acute inflammation of the pancreas is caused by existing pathology of the biliary tract. Pancreatitis is often combined with cholecystitis, which is why this disease needs to be treated promptly.
Instrumental methods for diagnosing cancer
Ultrasound methods
They are performed primarily on all patients with suspected cancer. They are considered the most informative and are available in almost every clinic.
- Ultrasound examination of the abdominal organs. It is carried out through the skin of the anterior abdominal wall. A direct sign of a tumor is the presence of a single volumetric formation or a heterogeneous cavity with a clear line between this formation and normal parenchyma. The head and body of the gland are best visualized, so tumors of this location are easier to diagnose in the early stages than tumors of the tail. Using ultrasound, you can detect a tumor from 1-2 cm. The ultrasound method allows you to assess the prevalence of the cancer process and the presence of metastases in the abdominal organs. Cancer germination is said to occur when there is germination of malignant cells into adjacent blood vessels and lymph nodes.
- Duplex scanning of pancreatic vessels. It is carried out in real time with simultaneous contrasting. Allows you to evaluate blood flow and the degree of vascularization of the tumor formation and parenchyma, the relationship of organ structures relative to each other. This study is performed on patients whose ultrasound showed signs of cancer cell growth in the blood vessels and aorta.
- Endoscopic ultrasound examination. A type of conventional transcutaneous ultrasound, only here an additional endoscopic sensor is used. This sensor is inserted through the esophagus and stomach into the lumen of the duodenum, where signals are received. The good thing about this method is that it allows you to diagnose tumors with a diameter of 5 mm or more, which cannot be detected with a regular ultrasound. In addition, the doctor evaluates the condition of adjacent organs and vessels for metastasis.
Mechanism of inflammation development
Acute destructive pancreatitis is a type of toxic enzymopathy. The development of this pathology involves the following processes:
- early activation of enzymes;
- direct toxic effect of substances on the gland;
- self-digestion of the organ from the inside.
In a healthy person, the enzymes formed are in an inactive form. When exposed to unfavorable factors, the process of their production is disrupted. They are activated ahead of schedule and begin to irritate the mucous membrane of the organ. Possible trigger factors are obstruction of patency in the area of the ampulla of the gland papilla, increased pressure in the ducts, and reverse reflux of bile.
Cell necrosis is caused by the action of lysosomal enzymes and proteinase. In the fatty type of acute pancreatitis, only lipids are affected. In hemorrhagic cases, vessels are involved in the process, which often leads to hemorrhage. Swelling of the gland due to alcohol intake is caused by an increase in the production of hydrochloric acid and pepsin, stimulation of secretin production and an increase in the tone of the sphincter of Oddi.
Predictions: How long can you live?
Survival rates vary widely and depend on the stage of the disease, so even the attending doctor cannot give an accurate prognosis. The average life expectancy for pancreatic cancer is as follows:
- After radical surgical treatment, the average survival rate is 1 to 2.5 years. About 20% of patients live more than 5 years.
- After palliative surgery, chemotherapy and radiation therapy, if the patient refuses surgery, the life prognosis is up to 1 year. On average 6-8 months.
Main clinical manifestations
Every surgeon and gastroenterologist knows not only the classification of acute pancreatitis, but also its symptoms. This disease is characterized by the following symptoms:
- pain syndrome;
- nausea;
- vomiting;
- fever;
- yellowness of the skin and sclera;
- decreased appetite;
- bloating;
- frequent bowel movements;
- the appearance of bluish spots.
An acute attack of pancreatitis lasts from several hours to a day or more. The main symptom is pain. It has the following features:
- associated with food or alcohol intake;
- acute;
- felt in the hypochondrium or epigastric region;
- sometimes it is shingles (with total inflammation of the organ);
- radiates to the left half of the body (hypochondrium, scapula, shoulder);
- very intense;
- combined with nausea;
- intensifies when a person is in a horizontal position;
- constant.
Acute destructive pancreatitis with severe necrosis can occur in such a way that acute pain disappears after some time while other complaints persist. This is an alarming symptom that indicates nerve death. Pain syndrome is not always eliminated by NSAIDs and analgesics. Severe pancreatitis requires the prescription of narcotic drugs.
Due to the accumulation of enzymes, patients' appetite decreases. Often there is an aversion to food.
A common symptom of the disease is repeated vomiting. It occurs after eating. The contents of the duodenum (undigested food and bile) are determined in the vomit. If the swelling is complicated by tissue necrosis, then symptoms of intoxication appear.
They indicate purulent inflammation. The following symptoms appear:
- fever;
- chills;
- tachycardia;
- rapid breathing;
- pale skin;
- cold sweat.
In severe cases, there are signs of dehydration. The reason is loss of fluid through vomiting. If left untreated, shock may develop. Its outcome could be death. When acute pancreatitis is combined with cholecystitis and liver pathology, signs of bile stagnation appear. The sclera takes on a yellow tint.
In this case, it is necessary to exclude acute biliary pancreatitis. Dyspeptic disorders in the form of heartburn and bloating are often observed. Pancreatic necrosis often manifests itself as blue spots in the abdominal area and hemorrhages. Acute catarrhal inflammation can resolve on its own without treatment.
Symptoms of pathology
The main signs of pathology are:
- weakness;
- fast fatiguability;
- insomnia;
- irritability;
- pain that is regular and prolonged;
- disturbances in the functioning of the dyspeptic system;
- nausea;
- vomit;
- decreased appetite;
- a sharp decrease in body weight;
- pallor, yellowness of the skin.
Video from Dr. Malysheva:
This form of pancreatitis is characterized by slow development. Sometimes the process can take more than 10 years. Making an accurate diagnosis is difficult, since the symptoms of the disease are similar to the manifestations of other diseases, and significant changes in the structure and appearance of the pancreas are not immediately noticeable.
This particular pathology can be suspected by changes such as:
- the presence of uneven growth of the pancreas (detected by palpation);
- enlargement of the head of the organ;
- disturbances in the exocrine function of the pancreas.
It is impossible to notice these features on your own, since this requires knowledge or special diagnostic procedures.
Consequences of acute pancreatic inflammation
In acute pancreatitis, the edematous form proceeds most favorably. With it, complications are rarely observed. Only a doctor knows how dangerous purulent (necrotizing) pancreatitis is. This pathology can lead to the following consequences:
- shock;
- sepsis;
- peritonitis;
- accumulation of fluid in the abdominal cavity;
- pseudocyst formation;
- multiple organ failure;
- the formation of abscesses;
- thrombosis;
The danger of this disease is that severe dehydration can develop. Against this background, hypovolemic shock occurs. The reason is a decrease in circulating blood volume.
Complications of acute pancreatitis can be early and late. The first group includes pulmonary dysfunction. Often the pleura is involved in the process.
Shock lung may develop. Pancreatitis is often complicated by pleurisy, acute respiratory failure and atelectasis. Necrosis of gland tissue can cause damage to the liver and kidneys. Toxic hepatitis and renal failure develop. Purulent damage to the pancreas causes heart damage. The brain also suffers. This manifests itself in the form of toxic encephalopathy.
Prognosis and possible complications
The prognosis for life with pseudotumor pancreatitis is favorable. The disease develops slowly, exacerbation occurs rarely, but in the absence of treatment the patient may experience the following complications:
- gland calcification,
- jaundice,
- vein blockage,
- peritonitis,
- diabetes,
- internal bleeding,
- degeneration of hypertrophied organ tissue into a malignant neoplasm.
Strictly following the doctor’s recommendations will allow the patient to save life and ensure stable remission.
Patient examination plan
Treatment begins after diagnosis. A sick child (adult) must be interviewed and examined by a doctor. The following studies are being carried out:
- auscultation;
- percussion;
- palpation of the abdomen (superficial and deep);
- Ultrasound;
- blood chemistry;
- study of water-electrolyte status;
- general clinical tests;
- radiography;
- CT scan.
A blood test reveals the following changes:
- increased ESR;
- decrease in hematocrit;
- leukocytosis;
- increased concentrations of glucose, lipase, amylase, C-reactive protein, urea;
- decreased levels of total protein, calcium, sodium and potassium.
About the clinic and diagnostics
Patients are most often bothered by dull pain, general weakness, periodic fever and an unclear formation in the epigastrium.
There can be very severe pain when the cyst presses on the nerve plexuses. But sometimes even a huge tumor does not bother the patient at all, and only occasionally does nausea and unstable stool occur.
In the same case, if a large find compresses the head of the gland, jaundice often occurs.
Taking into account modern research methods, it is not difficult to diagnose a cyst. A large structure can simply be palpated; sometimes enzymes in the urine and blood increase. But computed tomography and ultrasound are the best diagnostic tools. The main task of doctors will be to distinguish the cyst from malignant cystadenocarcinoma, and this may require puncture and histological examination.
Therapeutic tactics for pancreatitis
Every experienced doctor knows whether it is possible to die with acute inflammation of the pancreas. In order to reduce the risk of complications, patients should be treated as early as possible. If you suspect acute pancreatitis, you should do the following:
- provide the patient with peace;
- it is convenient to seat a person;
- exclude food intake;
- organize plenty of drinking;
- call a doctor or ambulance.
Enzyme preparations are contraindicated during an attack. It is not recommended to take painkillers. It is impossible to determine how long the attack will last. To alleviate the patient's condition, you need to give him a half-sitting position with his knees pressed. Medical assistance consists of the use of antispasmodics, novocaine blockade, and the use of enzyme inhibitors (Gordox, Trasylol, Aprotex).
Infusion therapy must be organized. It allows you to replenish fluid deficiency and restore electrolyte balance. Antibiotics are used to prevent purulent complications. All medications must be administered by injection. If an abscess or cyst forms, and if gallstone disease is detected, surgery is required.
Acute pancreatitis must be recorded in the surgical medical history. This is necessary so that in the future the doctor will have an idea about the inflammation of the pancreas suffered by the patient. After the course of treatment, you must follow a diet and give up alcohol. The doctor should tell the patient how long to adhere to proper nutrition.
Pancreatic cancer treatment
Treatment of pancreatic cancer is one of the most difficult areas in oncology. This situation is associated with many reasons, primarily with the predominantly elderly age of patients and the presence of concomitant pathologies. It is also important to note the difficulty of diagnosing a tumor with this location. Thus, patients are referred at late stages, when the tumor is considered inoperable, growing into vital anatomical structures and spreading metastases to distant organs.
ICD-10 in this reference book indicates all subtypes of the oncological process with one or another localization. Pancreatic cancer urolithiasis helps the doctor to accurately identify the location of the tumor in the organ and make the right decision on therapeutic measures.
Pancreatic cancer ICD 10 is designated by the following code:
C25.0 Malignant neoplasm of the head of the pancreas:
- C25.1 Bodies.
- C25.2 Tail.
- C25.3 Ducts.
- C25.9 Unspecified.
Principles of therapy
The main method of treatment for breast cancer remains unchanged - surgery. Whether it will be radical or palliative depends on the type of tumor, its stage and location.
Radical and palliative treatment
There are two main principles in the treatment of cancer patients:
- radical treatment, its essence is the complete removal of all malignant cells, which allows for a complete recovery in the future. In this case, it is important not to allow a single cancer cell to remain in the body, otherwise a relapse of the disease will occur. For these purposes, radical surgery is used to remove part or all of the pancreas, regional lymph nodes, gallbladder and its ducts, part of the stomach, duodenum, and possibly the spleen. After surgery, radiation or chemotherapy may be prescribed to make sure that no atypical cells remain;
- palliative measures are taken when the tumor is considered inoperable. As a rule, in the case of its germination into blood vessels, veins and other organs, as well as as a result of metastasis. In fact, it is a treatment for stage 4 and often stage 3 pancreatic cancer. The goal of palliative treatment is to prolong the patient’s life and improve its quality by partially relieving symptoms.
Therapy for resectable tumors
Unfortunately, at the stage when the tumor is considered operable, it is detected extremely rarely. In many cases, even when the operation begins and it is believed that the formation is resectable, nuances are identified that do not allow it to be completely removed. As a result, the operation turns from radical to palliative.
For radical therapy, the following operations for pancreatic cancer may be offered:
Surgery is the only effective treatment method
- pancreaticoduodenectomy or Whipple procedure. This resection is used when the head of the organ is affected. In this case, the head and part of the body of the gland, the gallbladder, its ducts, part of the small and duodenal intestines and the antrum of the stomach are removed. The Whipple procedure is a complex surgical procedure with a high mortality rate of approximately 10-15% of cases. Five-year survival rate, despite the radical method, still remains low at 5-8%;
- distal pancreatectomy is performed if the tumor is localized in the tail or body of the pancreas. The tail and body of the organ are removed, leaving only the head. Such an intervention is performed extremely rarely, since a tumor in the tail is almost always detected in an advanced stage. The average life expectancy for distal pancreatectomy is 10 months;
- A total pancreatectomy is performed if the entire organ or its head and body are affected. This type of surgery is characterized by complete removal of the gland, duodenum, spleen, antrum of the stomach, gallbladder and regional lymph nodes. Pancreatic cancer often progresses after surgery despite the radical nature of the procedure. This type of intervention is rarely performed due to disappointing results; the Whipple procedure is more often used.
Therapy for locally advanced cancer
In this case, surgery can only be performed as a palliative measure. To reduce the severity of pain in pancreatic cancer, eliminate bleeding or stenosis. If such symptoms are not observed or are not so pronounced, the operation may not be performed, so as not to once again put stress on an already weakened body.
In this case, chemotherapy is used for pancreatic cancer. The most common anticancer drugs that are administered intravenously when the gland is affected are Gemcitabine and 5-fluorouracil (5-FU). Radiation therapy may also be offered. These methods are not able to remove all cancer cells and lead to only partial regression of the tumor process.
Metastatic cancer and its therapy
Resection of the head of the pancreas
Pancreatic cancer treatment in this case is also palliative. Metastases from the main tumor spread far beyond the gland, affecting other structures and organs. Surgical intervention can be carried out only to reduce the tumor and, accordingly, intoxication in the body, as well as in cases of compression and stenosis of other organs.
Most often, chemotherapy is used in palliative measures, Gemcitabine is administered. Pancreatic cancer prognosis for existing metastases is negative, the average life expectancy of such patients is six months.
Other palliative methods
Additionally, in the treatment of inoperable patients the following is used:
- bile duct stents, they can help improve appetite, prevent severe weight loss and reduce itching;
- pancreatic cancer ASD 2 is a drug that, according to scientist Dorogov, can defeat even advanced stages of cancer. It was not recognized by official medicine, but in case of hopelessness, patients are ready for various experiments;
- antidepressants and narcotic substances such as morphine, which help relieve pain and the psychological state of the patient.
How long do patients with this diagnosis live with pancreatic cancer? The issue is ambiguous; with early detection, a positive outcome is possible, but no more than 10% of patients achieve it. As a rule, the life expectancy of such patients does not exceed one year.
Video: surgical treatment of pancreatic cancer. Robot-assisted and laparoscopic surgery
Be healthy!
onkolog-24.ru
Measures to prevent pancreatitis
The development of acute pancreatitis can be prevented. Cure does not mean that the disease will not develop again. To reduce the likelihood of relapse, you must follow the following recommendations:
- completely give up alcoholic beverages and smoking;
- exclude spicy snacks and dishes from the diet;
- eat a little 4-6 times a day;
- move more;
- drink at least 1.5 liters of water per day;
- do not overeat;
- eliminate stressful situations;
- treat diseases of the digestive system;
- monitor hormonal levels.
Proper nutrition and giving up bad habits are the main measures to prevent this disease. If pancreatitis does develop, you should consult a doctor on the same day. Thus, acute inflammation of the pancreas is a dangerous disease. In destructive forms of pancreatitis, even if assistance is provided, the fatal outcome reaches 50%.
Under the chronic form of pancreatitis, a constant inflammatory process of the pancreas is observed. During the acute course of the disease, replacement of the cellular elements of the organ with connective tissue and the formation of exo- and endocrine insufficiency of the organ functions is observed.
Diet and prevention for illness
The development of pseudoturmoid pancreatitis can be avoided by adhering to the following preventive recommendations:
- give up cigarettes and alcohol;
- promptly treat any infectious pathologies of internal organs, respiratory tract and oral cavity;
- for pancreatitis that has not yet entered the chronic stage, it is worth taking medications that inhibit the mechanisms of production of digestive enzymes in the pancreas.
You should also adjust your diet , and if it is not possible to completely give up your favorite foods, you need to include at least as many of the following products in your diet as possible:
- any cereals and pasta;
- fruits and vegetables after heat treatment;
- low fat fermented milk products;
- boiled fish and lean meat.
Any herbal teas, fruit drinks and compotes are recommended as drinks. In turn, it is necessary to exclude sour fruits, legumes, cabbage, baked goods, coffee, black tea and cabbage from the diet.
In the case of pseudoturmoid pancreatitis, you should not indulge yourself and drink alcohol in small quantities “on holidays”; you should also try to avoid any fatty foods and dishes.
Such a disease can worsen even with minimal provoking factors, and sometimes with such relapses even the intervention of a specialist who cannot prevent the death of the patient .
Classification of pancreatitis according to ICD 10
Healthcare, for the purpose of systematization and management, has developed a classification of diseases (ICD), which is revised once every 10 years. This is a normative document that provides a unified approach to the classification of diseases and serves as a mandatory classifier when making a diagnosis.
There are more than 40 classifiers of pancreatitis, which significantly complicates the communication between doctors when voicing a patient’s diagnosis. So that experts from different countries could easily share skills and understand each other, the International Systematization of Diseases (ICD) was established. Currently, the 10th revision system (ICD-10) is in effect, which is used to diagnose the disease.
According to the international classification, pancreatitis according to ICD 10 is divided into:
- K85 Acute pancreatitis.
- K86.0 Chronic pancreatitis of alcoholic etiology.
- K86.1 Other chronic pancreatitis.
There are 3 key types of chronic pancreatitis ICD code 10:
- Chronic calcific inflammation, often caused by alcoholism. With this inflammatory process, changes in the structure of the ducts of the organ and thickening of secretion are observed, which leads to blockage of the ducts.
- Chronic obstructive inflammation. It is characterized by a narrowing of the main ducts of the gland or its large branches.
- Acute inflammation of pancreatitis is not common and is an exacerbation of chronic pancreatitis.
In some cases, biliary or biliary-dependent pancreatitis is observed, which develops against the background of existing diseases - pathologies of the liver, gallbladder or biliary tract.
What it is?
Pseudotumorous pancreatitis (ICD-10 disease code – K86.1) is a chronic pathology, which is actually a complication of acute pancreatitis as a result of improper treatment or its absence.
The name of the disease is translated as “false tumor” and is explained by the fact that it is characterized by signs of a developing pancreatic tumor, although such formations do not appear in it.
This disease does not develop on its own: it always occurs against the background of chronic pancreatitis, in which fibrous tissue . When performing radiography during the examination, you can notice that with this disease the head of the pancreas enlarges (it increases significantly in size).
Etiology
The prerequisites for the occurrence of chronic pancreatitis according to ICD 10 are quite diverse. The formation of pain syndrome is caused by a number of factors:
- pathologies of the digestive system (ulcerative and cholelithiasis, cholecystitis, duodenitis, gastritis);
- excessive intake of alcoholic beverages, lack of protein in food;
- viral lesions, allergic reactions and toxic poisoning;
- surgical interventions;
- pathology of metabolic and hormonal processes;
- heredity.
Chronic pancreatitis ICD 10 (K86.0) often occurs with chronic alcoholism. In second place in terms of the purity of detection of this disease are dysfunctions of the biliary tract, duodenum and stomach disease.
Mechanism and causes of the disease
When a large number of enzymes that are usually involved in digestion accumulate in the affected organ, these compounds begin to digest the gland itself , resulting in tissue necrosis.
Fibrous tissue appears as a consequence of the protective reaction of the body, which thus tries to limit the spread of pathological processes.
In this case, pseudocysts appear at the site of such foci, the walls of which become calcified, as calcium salts settle on them. But such processes do not help avoid intoxication.
If nothing is done in time, death is possible.
Such processes can develop over years, during which the pancreas increases in size and begins to compress large arteries, the gallbladder and the duodenum. This leads to dysfunction of these organs.
The reasons for the development of such a disease may be:
- pathological processes in the biliary tract;
- autoimmune diseases and immune disorders;
- some viral lesions and injuries to internal organs (including those caused by negligence as a result of surgery);
- long-term treatment with antibiotics, corticosteroids and diuretics;
- abuse of fatty foods and alcohol.
This disorder is considered the last stage of development of chronic pancreatitis , and if treatment is not started when diagnosing the pathology, the outcome will be the most unfavorable. However, in some cases, even qualified treatment cannot prevent the death of a patient at an advanced stage of development of the disease.
Treatment of chronic pancreatitis
If pancreatitis is not treated promptly, it will lead to dysfunction of other organs. If you are diagnosed with chronic pancreatitis and its symptoms worsen, then therapy must be carried out immediately.
The patient is treated in a hospital, where he is prescribed a set of measures:
- Following a strict diet. For the first time, fasting is practiced. When the patient is allowed to eat, the food should be taken in small portions.
- Elimination of pain and spasms.
- Normalization of the digestive process.
- Replenishment of enzyme deficiency.
- Stop the inflammatory process.
- Restore damaged organ tissue.
- Carry out preventive measures.
When treating the chronic form, antibiotics are used if infection is present. This course lasts approximately 7 days. In case of inflammation of the ducts, Amoxicillin is prescribed to facilitate the outflow of bile; this allows the inflammatory focus to be stopped and prevent it from developing further.
Anti-inflammatory drugs can relieve pain. Only a doctor can competently select the dose of the drug.
“No-shpa” and “Drotaverine” will help to cope with spasms.
Chronic pancreatitis ICD code 10 is accompanied by digestive pathology, for this reason the patient must adhere to a strict diet and take enzymes.
In complex treatment, medications are prescribed to reduce the level of acidity (Almagel, Maalox).
Injections of Ringer, the drug “Hemodez” and saline have proven themselves to be effective in reducing intoxication in the body.
If therapeutic measures do not have the desired effect, then the patient is prepared for surgery.
Mechanisms of appearance of the main symptoms
In seventy percent of patients, pseudotumor pancreatitis is diagnosed already at the complication stage, since its symptoms are similar to the development of cancer, cholecystitis and other diseases. Among the most pronounced:
- systematic pain in the left side, worsening at night;
- disruption of the digestive system, changes in stool;
- a sharp decrease in body weight;
- decrease in the level of the hormone insulin;
- periodic nausea, vomiting;
- yellowing of the sclera of the eyes and skin.
The pancreas produces insulin and food enzymes. They begin to actively break down food when it enters the duodenum.
The danger of the disease is that the formation of scar or fatty tissue begins in the areas of damage. The functioning of the gland is disrupted, and the production of enzymes and insulin in the required quantities stops.
Inflammatory processes begin in the pancreas, which cause complications and provoke the development of diabetes mellitus or cancer in a person. Due to the growth of scar tissue in the organ, pancreatic necrosis appears, which can spread over almost the entire area of the organ.
If a patient has chronic pancreatitis, he is diagnosed with K 86.