Chronic bronchitis is actually an independent disease of the respiratory system (primary bronchitis); much less frequently, the disease occurs after acute bronchitis or other ENT diseases (secondary bronchitis).
In chronic bronchitis, the inflammatory process begins under the influence of harmful components that irritate the airways.
As a result, the function of the bronchial glands increases, and the amount of sputum they produce increases. An obsessive, constant or periodic cough appears.
Doctors diagnose chronic bronchitis when the patient coughs for at least 3 months a year and when this repeats for 2-3 years.
Among people suffering from chronic bronchitis, the highest percentage are “hard” smokers. It is they who voluntarily cause damage to their respiratory system, leading the bronchial tree to a painful state.
In this case, serious complications of the disease can arise - the appearance of hemoptysis, emphysema and respiratory failure, which in a chain reaction leads to memory impairment, heart failure, etc.
In addition, over time, simple ordinary chronic bronchitis is dangerous because it can turn into a purulent form, when purulent mucus is coughed up when coughing.
Chronic bronchitis affects not only smokers. Let's figure out what other reasons there are that cause the appearance of this disease.
What is chronic bronchitis
Chronic bronchitis is a long-term disease of the bronchi, characterized by the presence of cough with sputum for 2-3 months over the next 2 years. Chronic bronchitis (clinical guidelines were developed by practicing doctors) is a disease that can be treated, but it is better to prevent it.
Its prevalence increases in the age group of people 55–69 years old. Among this group, 15% of urban men and 23% of those living in rural areas suffer from the disease. Almost every second man over 70 years of age living outside the city has signs of chronic bronchitis.
WHO diagnostic criteria
The World Health Organization defines chronic bronchitis as a disease in which there are repeated episodes of persistent productive cough lasting at least 3 months for 2 or more years.
This is the main diagnostic criterion, but there are others:
- During auscultation, a typical picture is heard: breathing is hard, rough, wheezing is scattered, can be dry and wet, exhalation is prolonged;
- Bronchoscopy reveals inflammatory changes in the bronchi;
- a study of external respiration function shows the presence of bronchial obstruction;
- Based on the results of differential diagnosis, other diseases are excluded, which are also characterized by protracted periods of productive cough that manifest themselves over years. These are tuberculosis, bronchiectasis, chronic lung abscess and a number of others.
A cough with sputum production that occurs over long periods is not always a symptom of chronic bronchitis. If, in its presence, there are inconsistencies with the WHO criteria, especially the first one (duration from 3 months), the reason may be:
- smoking (smoker's cough);
- harmful working conditions, as a result of which the respiratory tract is irritated;
- pathologies of the nasopharynx that cause coughing;
- acute bronchitis with a prolonged or recurrent course;
- contact with volatile irritating substances that cause respiratory discomfort and cough;
- a combination of several factors.
Anamnesis is also taken into account - a high frequency of colds is the basis for a diagnosis of chronic bronchitis.
Types of chronic bronchitis
Bronchitis can be acute or chronic. The first is a wet cough that produces mucus in combination with a cold or upper respiratory tract infection. Damage to the bronchi is transient. In the chronic form, there is also a wet cough and thick mucus, but the disease lasts a long time and is long-lasting.
The chronic type of the disease is characterized by the presence or absence of obstruction in the airways:
- Obstructive is characterized by swelling and narrowing of the airways, increased production of mucus, which prevents air from entering the lungs.
- The non-obstructive nature of the disease occurs with the release of mucus and sputum, but without ventilation disturbances.
Each type has its own characteristics of sputum:
- mucous;
- mucopurulent;
- purulent.
Auscultation
The following types of breathing are determined by auscultation:
- vesicular;
- bronchial;
- hard;
- saccaded;
- amphoric.
Breathing will be increased and decreased. Wheezing is heard over pathologically changed areas. According to the acoustic characteristics, wheezing is usually divided into dry (buzzing and whistling) and wet (large, medium, and fine bubbles).
Auscultation for bronchial diseases is important for diagnosis, dynamic monitoring, and identification of complications. Each variant of bronchitis is accompanied by characteristic physical features.
For chronic bronchitis
This type of bronchitis is characterized by hard breathing, coughing, dry wheezing during auscultation, and prolongation of exhalation.
The presence of wheezing is due to the viscosity of sputum, and the tonality depends on the size of the bronchus. Low-pitched sounds are heard over the large bronchi during the inhalation phase.
When the process is localized in small-caliber bronchi, dry wheezing will be heard during the exhalation phase.
A distinctive feature of wheezing due to inflammation of the bronchi is its variability (it changes or disappears when coughing). The presence of moist rales may indicate the development of pneumonia.
For acute bronchitis
Increased vesicular breathing is heard in patients. Dry wheezing of various tones is determined by the level of damage to the bronchial tree. Listening to crepitus is not a pathology of the bronchial tree. This auscultatory picture is characteristic of pneumonia.
For obstructive bronchitis
A distinctive feature of obstructive processes in the bronchi in adults is noisy and wheezing breathing that can be heard from a distance.
With obstructive bronchitis, adults experience noisy and wheezing breathing.
The auscultatory picture will be represented by dry wheezing and prolonged exhalation. In infants, obstruction is also accompanied by distant wheezing. Dry and varied moist rales are heard above the surface of the lungs. Inhalation prevails over exhalation. Shortness of breath develops quickly.
Stages and degrees of chronic bronchitis
The classification of the disease is based on indicators of the functional state of the lungs.
Based on these indicators, 4 stages of the disease are distinguished:
- light;
- moderate;
- heavy;
- extremely heavy.
As practical medicine has shown, such a division does not always reflect all cases of the disease. In therapy, the transition from one stage to another is often not distinguishable.
Classification of COB by severity:
| Degrees of the disease | Severity of the leak | Description of symptoms |
| 0 | No | Shortness of breath during strenuous exercise |
| I | Light | Shortness of breath when walking quickly on level ground |
| II | Average | Due to shortness of breath, walking on level ground slows down, breathing is intermittent, with stops, when walking on level ground at a moderate pace |
| III | Heavy | Severe shortness of breath after walking 100 m or several minutes on level ground |
| IV | Very heavy | The patient is suffocating when dressing and undressing, severe shortness of breath, making it impossible to leave the house |
Complications of bronchitis are divided into two groups:
- associated with infection: pneumonia, non-allergic bronchitis, asthmatic, bronchial dilatation;
- associated with the progressive development of bronchitis: emphysema, pulmonary, respiratory failure, pulmonary pneumosclerosis, development of cor pulmonale.
Causes and risk factors
Absence of temperature is most often observed in acute obstructive bronchitis of non-infectious etiology. Bronchitis often occurs without fever in patients with weakened immune systems. In pediatric practice, this form of the disease often develops in premature infants or in infants with perinatal pathology of the heart or respiratory system.
In some cases, the clinical picture of bronchitis without fever also does not include a cough. This may indicate an early stage of the disease, significant damage to the bronchioles, or a non-standard course of the disease.
The occurrence of bronchitis without an increase in temperature, especially in children, more often leads to the disease becoming chronic.
One of the leading risk factors for the development of bronchitis without fever is the uncontrolled use of antibacterial drugs during the treatment of respiratory infections.
Bronchitis caused by microscopic fungi usually occurs without fever, but is rare. Typically, this form of the disease is diagnosed in weakened patients, especially after treatment with antibacterial drugs.
Symptoms of chronic bronchitis
The primary ailment with which patients go to clinics is cough, sputum, mucus released during expectoration, and shortness of breath is often present. Symptoms are pronounced in the morning, after waking up. During cold seasons, such patients are prone to frequent colds. Sometimes doctors diagnose them with “smoker’s bronchitis,” thereby delaying the start of treatment.
But at the first stage, cough is the only symptom of a developing disease.
During the period of exacerbation of the disease, additional symptoms appear:
- scattered wheezing in the lungs;
- decreased performance;
- heavy sweating;
- weakness;
- headache;
- myalgia.
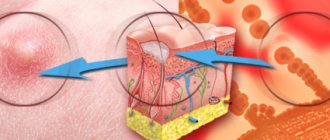
The diagram lists the symptoms and causes of chronic bronchitis.
In the obstructive form, signs are found:
- shortness of breath;
- dry cough without sputum production;
- high-pitched wheezes.
During periods of remission, patients continue to cough with sputum production, but shortness of breath and other symptoms disappear.
Differential diagnosis
A number of symptoms of chronic bronchitis without obstruction are similar to the symptoms of other diseases of the respiratory system. They must be distinguished from each other in order to prescribe adequate treatment.
Prolonged, recurrent acute and chronic form.
- In the first case, symptoms of bronchitis persist for more than 2 weeks, but less than 3 months.
- In the second, the episodes are shorter, but repeated frequently, at least 3 times a year.
- Chronic bronchitis is characterized by a duration of exacerbations of 3 months.
Bronchiectasis. Chronic bronchitis develops in adulthood; cough is not always accompanied by purulent discharge. For bronchiectasis:
- long periods of coughing have been observed since childhood;
- a large amount of purulent sputum is released;
- the phalanges of the fingers and nails acquire a characteristic thickened shape;
- bronchography reveals dilatation of the bronchi.
Bronchial tuberculosis. Night sweats and low-grade fever are characteristic of both tuberculosis and chronic bronchitis in the acute phase. But with tuberculosis:
- weakness, fatigue are more pronounced, loss of appetite and weight are possible;
- the sputum is not purulent, but hemoptysis is observed;
- Koch bacilli are found in sputum and washing waters;
- bronchoscopy reveals scars and fistulas on the mucosal surface.
Bronchial cancer is the most dangerous disease, which is important to distinguish from bronchitis as early as possible. For cancer:
- cough is more persistent, often with hemoptysis;
- atypical cells are detected in the sputum;
- in the later stages, severe pain appears in the chest, rapid weight loss is observed;
- biopsy results confirm oncology.
Expiratory collapse of the trachea and large bronchi:
- the cough is dry and paroxysmal, has specific sound characteristics;
- occurs under the influence of provoking factors (laughter, stress, sudden change in body position);
- possible attacks of suffocation, dizziness, fainting;
- fibrobronchoscopy and spirometry demonstrate characteristic changes.
Causes of chronic bronchitis
According to WHO, this disease is the fourth leading cause of death in the world. The consequences of smoking, both active and passive, play a big role in the occurrence of non-obstructive bronchitis.
Daily irritation of the bronchial mucosa causes increased mucus production. This disrupts the protective function of the bronchi and the supply of the required amount of oxygen.
In addition to smoking, the causes of bronchitis may be:
- prolonged inhalation of dust, chemicals;
- acid reflux;
- infections that suppress the immune system;
- age (after 60 years the risk of the disease increases).
Causes of obstructive form:
- severity of bronchial insufficiency;
- excess body weight;
- poor nutrition;
- frequency, severity of attacks;
- pulmonary hypertension.
In the absence of treatment, causes of death arise:
- respiratory failure;
- lung cancer;
- tumors of various localizations.
What are the reasons?
Chronic bronchitis is based on almost the same reasons as its acute form, but in a slightly different sequence.
Read more about acute bronchitis.
If most doctors place the infectious process in the first place as the main cause of acute bronchitis, then for chronic bronchitis the infection is often secondary. The main role here is played by constant exposure of the respiratory tract to irritating substances, namely tobacco smoke, dust, gases and chemicals.
So, here are the main causes of chronic bronchitis:
— tobacco smoke when smoking and its passive inhalation . Constant inhalation of tobacco smoke reduces the natural protective resistance of the bronchial mucosa to damaging environmental factors, leading to a chronic inflammatory process. Almost 90% of all patients are active smokers or have smoked for a long time. Every second smoker over 40 years of age suffers from chronic bronchitis. It is believed that the more cigarettes a person smokes per day, the higher the risk of developing this disease. For example: after stopping smoking, respiratory function indicators improve within 6 weeks.
— inhalation of harmful industrial substances . These include sulfur oxides, products of industrial combustion, coal, oil, and natural gas. Under conditions of constant inhalation of dust, gases and vapors of harmful substances, the self-cleaning mechanism of the bronchi does not have time to remove all accumulated harmful substances, leading to the development of the inflammatory process. As a rule, this is typical for people working in hazardous working conditions, for example, miners, workers in the paint and varnish industry, etc., and is classified as an occupational disease.
- genetic predisposition and congenital characteristics of the bronchial tree . Such people are characterized by increased sensitivity of the bronchi to irritating substances from the outside.
— climatic conditions. Very rarely they are the root cause, but they create a favorable background for the development of the disease. Most often it develops in the so-called off-season: autumn-spring.
- infections. Even now, there is active debate among doctors whether infection plays a primary or secondary role in the development of the disease. But they still tend to believe that the primary role is played by the constant inhalation of irritating substances, and infection is crucial in exacerbating symptoms. Moreover, the trigger for this can be viruses (ARVI, influenza, etc.) and bacteria (mycoplasma, streptococci, Haemophilus influenzae, etc.). It should also be noted that the development or exacerbation of the disease can be caused by infections from the ENT organs: sinusitis, tonsillitis, otitis, etc., when the infection from them spreads to the bronchi. A disrupted process of self-cleaning of the bronchi creates favorable conditions for the proliferation of viruses and bacteria.
- a decrease in the protective function of the immune system creates a favorable background for the exacerbation of the disease and the proliferation of infection.
Diagnosis of chronic bronchitis
Chronic bronchitis (clinical guidelines developed by the Federal Center for Diagnosis and Treatment of COPD) involves the following diagnostic methods:
Laboratory:
- blood analysis;
- sputum cytology examination;
- microbiological and bacteriological examination of sputum.
Instrumental:
- chest x-ray;
- bronchoscopic examination;
- electrocardiography to exclude colds
- echocardiography to rule out heart disease.
Functional:
- bronchodilator method, for diagnostics, special drugs, bronchodilators are prescribed and their effect on the body is assessed;
- monitoring of lung function is carried out in patients on mechanical ventilation;
- spirometry, to assess the severity of the disease, allowing you to measure lung volume, inhalation volume in one second and expiratory speed.
Laboratory tests are carried out in municipal clinics or private medical centers, the cost of which is estimated:
- blood test: 200–300 rubles;
- cytological tests, microbiological: from 500 to 1 thousand rubles.
Instrumental diagnostics can be carried out in a district clinic or in a private medical center, the cost of which will be from 1 thousand to 2 thousand 700 rubles. The cost of functional studies, for example, spirometry, ranges from 700 to 1 thousand 200 rubles.
The degree of severity is determined using diagnostic procedures:
- Pulse oximetry. A non-invasive method that determines the degree of oxygen saturation in the blood. It is carried out using a pulse oximeter machine. Cost of the procedure: 500 –1 thousand. rub.
- Peak flowmetry. A test method that determines the maximum rate at which a person can exhale after taking a full, deep breath.
- Pneumotachography. Using this method, the volume of the flow rate of inhaled and exhaled air is determined. The volume is recorded in quiet and forced breathing. Cost of service: from 360 rub.
Diagnosing chronic bronchitis is not an easy task. At the initial stage, instrumental and laboratory tests do not always confirm the presence of the disease.
X-ray
Pulmonologists use various x-ray techniques to diagnose lung diseases. Basic types of research include the following:
- radiography and fluorography;
- tomography;
- bronchography;
- pneumopolygraphy;
- CT scan.
The generally accepted scheme for describing radiographs reflects:
- the nature of the pulmonary pattern;
- condition of the lung tissue;
- contours and position of the diaphragm;
- condition of the roots of the lungs;
- features of the heart shadow;
- condition of the chest skeleton.
The scheme for describing radiographs reflects the condition of the lung tissue and the features of the cardiac shadow.
For accurate analysis, radiographs are taken in two projections.
When to see a doctor
After acute bronchitis, if it has been treated properly, the walls of the bronchi restore their previous structure and continue to work as usual. The mucociliary apparatus, responsible for the cleanliness of the respiratory tract, is restored.
If the therapy was of poor quality, then bronchitis can become protracted and chronic. Any inflammation in the bronchi does not completely disappear; the damage that was caused to them remains. With each subsequent exacerbation, the area of inflammation expands.
Therefore, after the disease, you should pay attention to whether symptoms remain that do not stop or recur:
- frequent attacks of acute bronchitis;
- a wheezing cough that does not go away within several weeks;
- shortness of breath;
- increased amount of dark yellow or green mucus when coughing;
- chest pain when inhaling and exhaling.
At the first sign of illness, you should visit a doctor.
Prevention
If bronchitis often occurs without fever, you need to pay attention to preventive measures:
- since inflammation of the bronchi can be a consequence of an acute respiratory disease, it is necessary to treat all infections in a timely manner;
- it is necessary to increase immunity, namely take vitamins, follow the recommendations of proper nutrition, lead an active lifestyle, play sports;
- prevent hypothermia of the body;
- vaccinate before the epidemic season;
- observe the rules of personal hygiene.
It is also recommended to stop drinking alcohol and smoking.
Prevention of chronic bronchitis
Primary prevention consists of active treatment of the first protracted inflammatory process in the lungs and includes the following measures:
- Short courses of GCS (glucocorticosteroid therapy) 1–2 times a year.
- Taking Atrovent.
- To give up smoking.
- Pneumotropic bacterial vaccines.
- High protein diet.
- Carrying out gymnastics according to Kuznetsov.
During periods of exacerbation of chronic bronchitis, it is correct to:
- take only those antibiotics that are sensitive to pathogens (drugs are prescribed based on the results of a sputum test);
- include protein-rich foods in your diet;
- perform breathing exercises according to Kuznetsov.
You cannot take the same antibiotics year after year and abuse carbohydrate foods.
Diagnostic methods
In addition to studying the medical history, patient complaints, examination, auscultation and other physical diagnostic methods, a number of laboratory tests and instrumental studies are usually prescribed. Depending on the characteristics of the patient’s condition, suspicions of a disease other than acute bronchitis, the doctor may prescribe different tests.
Lab tests
In chronic bronchitis, blood and sputum are examined.
- A general blood test does not reveal any significant changes. The most pronounced signs of the inflammatory process are during exacerbation of chronic bronchitis and the development of its purulent form. But even in this case, leukocytosis and increased ESR are moderate.
- A biochemical blood test allows you to determine how far the inflammatory process has gone.
- Sputum is subjected to macroscopic and bacteriological examination. Its color, consistency and structure, cellular composition are assessed. These data make it possible to determine the form of chronic bronchitis and distinguish it from other diseases with similar symptoms. When inoculating the microflora, pathogens of the disease are identified. In addition, their sensitivity to antibiotics is determined. This is important for prescribing the correct effective treatment regimen.
Instrumental studies
The main method of instrumental diagnosis for chronic bronchitis is fluoroscopy and radiography. Other studies can be prescribed by a doctor according to indications, usually for the purpose of differential diagnosis. In uncomplicated chronic bronchitis, there are no radiological signs of the disease.
They appear in people who have been suffering from chronic bronchitis for several years, especially if other diseases are associated:
- the pulmonary pattern is more pronounced and deformed according to the loop-cellular type;
- lung fields are more transparent than normal;
- the shadows of the roots of the lungs are expanded;
- if peribronchial pneumosclerosis develops, the image may show thickening of the bronchial walls;
- lesions of the bronchi manifest themselves in the form of changes in their contours, caliber and direction.
Bronchography is a type of x-ray examination using a contrast agent. It is used primarily for differential diagnosis purposes, for example, with bronchiectasis or tuberculosis. Allows you to identify dilations of the peripheral bronchi, evaluate the pattern of contours, and the patency of the lateral branches. In the absence of bronchiectasis, the smallest bronchi are not filled with contrast agent.
Bronchoscopy is an invasive diagnostic method. A fiber-optic system is inserted into the bronchi, making it possible to examine them from the inside and collect material.
The most informative analysis of sputum obtained using bronchoscopy. They resort to it if it is not possible to collect sputum for analysis due to its scarcity and viscosity. This method is also used for indications for mucosal biopsy.
During bronchoscopy, the condition of the mucous membrane is assessed according to the following criteria:
- color (pale pink, bright red, purple-bluish);
- the nature of the secretion covering the walls (mucus, pus);
- thickness (thinning or thickening);
- bleeding (absent, sometimes observed, severe).
Based on the totality of these signs, the severity of the disease and the degree of inflammation can be assessed.
loading…
Differences between obstructive and non-obstructive chronic bronchitis
To differentiate these two forms of chronic bronchitis, they resort to studying the function of external respiration and blood gas composition
FVD study:
- spirometry. Determination of forced expiratory volume, vital capacity of the lungs, their ratio, residual volume. Changes occur with the development of obstructive bronchitis and become more pronounced as it progresses;
- pneumotachometry – assessment of air flow velocities during inhalation and exhalation. With obstructive phenomena, exhalation slows down significantly;
- peak flowmetry - determination of peak expiratory flow. Allows you to identify bronchial asthma.
In non-obstructive chronic bronchitis, most of these indicators are within normal limits. There may be an increase in residual lung volume and a decrease in volumetric velocity, while vital capacity and peak velocity remain normal.
Determination of the gas composition of the blood is carried out in cases of respiratory obstruction and suspicion of the development of an obstructive form of chronic bronchitis. In the early stages of this disease, changes in gas composition are minor. As it progresses, the concentration of carbon dioxide increases and the oxygen content decreases.
Treatment methods for chronic bronchitis
Chronic bronchitis (clinical recommendations primarily concern the prevention of progressive development) is treated according to the following scheme:
- Non-drug effects: reduction of risk symptoms; educational programs.
- Drug treatment.
The first group includes activities:
- smoking cessation, including medicinal methods;
- increased physical activity;
- vaccination against pneumococcal infection and influenza.
Patients with non-obstructive chronic bronchitis are treated on an outpatient basis.
Medications
Chronic bronchitis is treated with medications, the choice of which depends on the clinical symptoms, frequency of exacerbation, and doctor’s recommendations. In most patients, exacerbation of the disease is influenced by non-infectious factors. In 35% of patients this happens due to a respiratory viral infection. In this case, the doctor draws up a pharmacological treatment regimen.
- Therapy with antibacterial agents.
- Bronchodilators.
- Auxiliary treatment methods.
The first group includes oral drugs with 1-2 single cycles of administration per day.
- 2nd generation cephalosporins.
- Amoxicillin with clavuanic acid. Active against gram-negative and gram-positive aerobes. Dosage is calculated depending on the patient's weight. For patients weighing more than 40 kg, the dose is suggested from 250 mg to 500 mg, depending on the severity of the disease. Price 45 rub.
- Clarithromycin (Fromilid). Acts against certain bacteria. Dose: no more than 500 mg. Price7a: from 70 rub.
Antibacterial therapy is prescribed after receiving the results of a mucus test, or when other drugs are ineffective. The second group of drugs includes b2-sympathomimetics, anticholinergics and theophylline. Drugs and their dosage are prescribed depending on the severity and form of the disease.
Bronchodilator drugs are available in the form of aerosols, usually in dosed doses; treatment is also carried out with nebulizers. They are used in cases of severe bronchial obstruction.
Prescribed drugs:
| Medicine price (in rub.) | Inhaler dose | Nebulizer solution | ||
| Single dose in mg | Daily dose in mg | Single dose in mg | Daily dose with mg | |
| Salbutomol 90 –100 | 0,1–0,2 | 0,4–1,2 | 2,5–10,0 | 10,0 |
| Terbutaline | 0,25–0,5 | 1,0–3,0 | 0,5 | 2,0 |
| Fenoterol 270 | 0,2–0,4 | 0,8–2,0 | 1,0 | 4,0 |
| Ipratropium bromide 280-360 | 0,02– 0,04 | 0,08–02 | 0,25– 0,5 | 1,0–20 |
Mucoregulatory agents are also used:
- Ambroxol. A mucolytic drug that thins mucus and promotes its removal from the bronchi. Prescribed in tablet form, intravenously or via nebulizer. Dose – no more than 30 mg, divided into 3 doses. Price: from 20 rub. for 10 tablets.
- Acetylcysteine. Stabilizes the process of sputum removal, increases its volume, and inhibits the production of cytokines. Prescribed doses: 600–1200 mg per day. When using the drug in a nebulizer, 300–400 mg is used 2 times a day. Price: from 60 rub.
- Carbocysteine. Improves the quality of sputum, stimulates the restoration of the mucous membrane. Daily dose: 1500–2250 mg.
Drugs for basic therapy of mild chronic disease:
- Atrovent. Bronchodilator, prevents the development of bronchospasm. Price: from 200 rub.
- Vitamin C. Taken for vitamin deficiency at 1000 mg per day. Price from 250 rub.
- Ribomunil. Activates antiviral immunity. For the treatment or prevention of chronic bronchitis, a single dose of 0.75 mg is suggested, which corresponds to 3 tablets. Initially taken for 4 days in a row, and then drunk for 5 months, every 4 days of the new month. Price: from 260 rub.
- Prednisolone. Prescribed for obstructive airway disease. Taken orally in the morning, either the entire daily dose at once, or a double dose every other day. The doctor prescribes the medication regimen. Price: from 20 rub. for 10 tab.
- Amoxicillin.
Drugs related to glucocorticosteroids are used when basic drugs are ineffective. But they often lead to side effects: steroid gastrointestinal ulcers, steroid diabetes, osteoporosis.
Traditional methods
Alternative therapy for chronic bronchitis involves improving lung function and reducing the severity of symptoms.
Herbal infusions that help with chronic cough:
- Ginger loosens and breaks up thick mucus and helps with breathing. Can be used as a tincture, fresh for brewing.
- Thyme. Reduces congestion and allows you to breathe normally. Can be added as a tea leaves by combining thyme with honey.
- Marshmallow root.
- Ledum.
- Plantain leaves.
- The leafy part of the coltsfoot grass.
- Liquorice root.
To prepare infusions, you should brew the herbs with boiling water, let them brew for several hours, and then take them several times a day, diluting them with water. Certain minerals may help combat the symptoms of bronchitis. A beneficial mineral would be zinc, taken in the form of zinc gluconate, 15 to 25 mg per day.
Home remedies used to treat bronchitis include:
- Honey. You can add one spoon to tea, or make a paste with crushed ginger and 1-2 pieces. carnations. The paste should be taken 1 tsp. 2–3 times a day.
- Turmeric. Its anti-inflammatory properties help reduce the amount of mucus. To do this, add 1 tsp. powder into a glass of milk. Stir, cook a little. Drink the hot mixture twice or thrice a day.
- Oil inhalations , for example, with eucalyptus oil. Add a few drops to a cup of hot water and, covering your head, inhale the vapors for several minutes.
Other methods
For non-obstructive forms of the disease, treatment methods help:
- vibration chest massage;
- breathing technique according to Strelnikova;
- postural drainage, which helps free the bronchi from mucus;
- sanatorium-resort treatment in boarding houses in central Russia.
Chronic bronchitis (clinical recommendations include various therapeutic methods), obstructive form, is treated with pulmonary rehabilitation methods.
These include:
- Oxygen therapy. The procedure is prescribed when there is a strong decrease in oxygen in the blood. In this case, the risk of cardiac arrhythmias increases, especially during sleep, and pulmonary hypertension develops. This method can reduce mortality in patients with obstructive chronic bronchial disease.
- Home ventilation. Oxygen concentrators are used to carry out the procedure at home. They are needed for better ventilation of the lungs, prevention of nocturnal hypercapnia (a condition of the body caused by an increased amount of carbon dioxide in the arterial blood), and improved sleep quality.
- Surgery. Lung volume reduction surgery is performed by removing part of the organ to reduce hyperinflation and improve the functioning of the pumping muscles. It is used in patients with chronic bronchitis complicated by emphysema.
Folk remedies
Traditional medicine remains the main method, but additional recipes can be used. They are easy to prepare at home from food, herbs and other available ingredients. The advantages of this treatment are safety, low price and lack of side effects.
Lemon with glycerin
One of the most gentle folk medicines is suitable for use at any age, as well as during pregnancy. The ripe fruit must be brought to a boil in a pan of water, then cooled and the juice squeezed out of half the fruit. It is better to immediately use a container with a volume of 0.25 liters. A few tablespoons of glycerin are also added here (to soften and moisturize the mucous membranes), and the rest of the space is filled with honey. This drug is intended for oral use, a spoon half an hour before each meal. It has no contraindications, so you can drink it until you get the desired result.
Black radish
The juice of this root vegetable is considered healing for coughs and other symptoms of respiratory system diseases. It needs to be prepared in a certain way. To do this, take a medium-sized vegetable and make a cut on top in the form of a recess. A full spoon of honey is placed there, covered and left to infuse for at least a day. During this time, liquid is released from the radish pulp. It can be taken out and consumed orally, 100-150 ml before meals. The course of taking the drug lasts at least 1-2 weeks, then it can be repeated as necessary. The radish is kept in the refrigerator and taken out only before the procedure. When honey runs out, it should be replaced with a new portion.
Onion
This plant contains phytoncides. They determine the pronounced antibacterial properties and effectiveness of the spicy vegetable for various respiratory diseases. In addition, the product perfectly strengthens the body's immune defense. The easiest way to use it is to consume it fresh orally as a seasoning for any dish. You can also clean it, leave it in hot water, and when it cools down, breathe in the fumes. Such inhalations clear the bronchi of mucus and remove it with a cough.
There are also combined recipes based on onions. Several small heads are brought to a boil in the sugar liquid, and then continued to simmer for another 15-20 minutes. During this time, they are reduced by half, and the water receives all the useful components. The decoction is taken a few tablespoons before meals.
An equally effective way to treat bronchitis is an infusion of milk with onions. The ingredients need to be boiled, during which the plant turns into mush. Next, it remains to add a little honey, it is also useful for easing breathing and strengthening the immune system. The product tastes sweet and is allowed for use at any age without contraindications. They drink it every hour for several days.
Herbal decoctions
Many herbs have proven beneficial in treating bronchitis and other inflammatory diseases of the respiratory system. Thus, pine needles are considered a simple and safe way to relieve spasms of smooth muscles and prevent emphysema. It is used as part of healing decoctions and infusions, soothing baths and steam inhalations. The essential oils of this tree are also popular. They are recommended for use in rooms where asthma patients are often present.
Conifers are not the only way to cure chronic bronchitis. There are recipes based on thermopsis, licorice, coltsfoot, and many other ingredients. Dry crushed raw materials just need to be brought to a boil or poured with hot water and kept warm for several hours. Plants can also be infused with alcohol or vodka, and then taken orally or used for rubbing the chest.
Possible complications
Bronchitis can lead to pneumonia.
Repeated frequent attacks of simple bronchitis lead to the development of chronic obstructive pulmonary disease, which can lead to many complications over time:
- pulmonary heart disease or heart failure;
- high blood pressure;
- breathing problems, swelling of the legs and ankles;
- pulmonary hypertension;
- pneumothorax (accumulation of air in the space between the lung and chest wall).
Chronic bronchitis with an aggravating factor such as emphysema is part of the leading group of chronic diseases, which in 30% are combined with other pathologies.
Diseases that often develop against the background of chronic bronchitis:
| Disease | Incidence rate percentage |
| Depression | 34 –41 |
| Lower respiratory tract infection | 68 –73 |
| Sleep apnea syndrome | 18 –27 |
| Cataract | 32 –333 |
| Impotence | 38 –44 |
| Osteoporosis | 29 –33 |
In recent years, cases of diabetes mellitus in patients with chronic bronchitis have become more frequent.
Chronic obstructive bronchitis is a long-term, intractable disease. Compliance with all clinical recommendations at the initial stage, in the non-obstructive form, helps to slow its progression, control symptoms, and achieve recovery.
Author: Belyaeva Anna
How is everything going?
Normally, in a healthy person, every 2 hours the surface layer of the bronchial mucosa is renewed due to the self-cleaning mechanism. The cilia on its surface remove all accumulated particles of dust and harmful substances from the bronchi (small, medium and large) towards the trachea and larynx, thereby preventing the development of inflammation in the bronchi.
In this case, this mechanism is disrupted due to constant inflammation of the mucous membrane and loss of the ability of the cilia on the mucous membrane to remove harmful substances. In addition, their mucus production in the bronchi increases, its composition changes and its viscosity increases.
The disease occurs when the bronchial mucosa repeatedly becomes irritated and inflamed. Constant irritation and swelling can damage the airways and cause sticky mucus to build up, making it difficult for air to move through the lungs. This leads to difficulty breathing, which gradually worsens. Inflammation can also damage the cilia, which are hair-like structures. They help protect the airways from germs and other irritants. When cilia do not work properly, the airways often become a breeding ground for bacterial and viral infections.
After a long period of inflammation and irritation in the bronchi, several characteristic symptoms occur, including a persistent, severe cough that causes mucus to leak from the lungs. The mucus may be yellow, green or white.
Mucus accumulates in the lumen of the bronchi, and in conditions of impaired functioning of the cilia on the bronchial mucosa, it is poorly excreted and stagnates, creating conditions for the proliferation of bacteria and viruses in it. The constant inflammatory process disrupts the normal process of warming, humidifying and purifying the inhaled air, thereby increasing the irritating effect of harmful substances on the bronchi.
Over time, the amount of mucus gradually increases due to increased mucus production in the lungs. Mucus eventually accumulates in the bronchi and restricts airflow, causing difficulty breathing. This shortness of breath may be accompanied by wheezing, which gets worse with any type of physical activity.
In the later stages of the disease, the skin and lips may become bluish due to lack of oxygen in the blood. Decreased oxygen levels in the blood can also lead to peripheral edema, swelling in the legs and ankles.
As the disease progresses, symptoms may also vary in severity and frequency. For example, the cough will go away temporarily, followed by a period of more intense coughing.
One of the adverse consequences is the occurrence of obstruction, i.e. “blocking” the lumen of the bronchi for one reason or another. Namely: thickening of the bronchial mucosa due to inflammation and swelling, proliferation of connective tissue, blockage of the bronchial lumen with mucus, spasm of the bronchi, their collapse on exhalation. Moreover, the process involves both small bronchi and bronchioles, as well as medium and large bronchi. Most of these causes are reversible and may disappear with recovery.
Main symptoms
What is chronic bronchitis? This is one of the most common diseases of the respiratory system, most often caused by an infection of viral or (less often) bacterial origin. The main symptom of chronic bronchitis in adults and children is a prolonged cough. The cough continues for more than four weeks, accompanied by constant production of sputum of various types (purulent, mucous, watery). At first, attacks are more often observed in the morning; during the day, the patient may cough after physical activity or when going out into the cold. In the later stages of the disease, shortness of breath appears.
Other symptoms of chronic bronchitis (ICD code 10, which the specialist notes in the patient’s card - J42) are wheezing and extraneous sounds during breathing, increased body temperature, cyanosis (blueness) of various parts of the body. Cyanosis occurs due to weakened gas exchange in the lungs and lack of oxygen. This may manifest itself as periodic dizziness, nausea, insomnia, and headaches. In children, chronic bronchitis most often occurs due to infection against a background of weak immunity. Therefore, the disease may be accompanied by a clinical picture characteristic of influenza infection (streptococci, pneumococci, staphylococci, respiratory syncytial infection).
Antibacterial therapy for illness
The issue of the use of antibiotics for chronic bronchitis (ICD code 10 - J42) is controversial and is decided exclusively individually. Antibacterial therapy is advisable for complicated viral bronchitis or concomitant diseases, bacterial bronchitis. Macrolides, penicillins, and cephalosporins are used. The choice of a specific drug depends on the characteristics of the disease and sensitivity. But still, in most cases, antibacterial drugs do not have the necessary effect, and can also cause bronchial obstruction syndrome - blockage of the bronchi caused by swelling of the mucous membrane.
The main symptom that indicates the need for antibiotics is purulent sputum. If such a symptom occurs, an additional examination is prescribed, based on the results of which a suitable medicine is selected. In case of chronic bronchitis, you should never choose an antibiotic on your own. The possible harm from using the wrong medicine may significantly exceed the expected effect. Acute inflammation is almost always successfully treated with topical drugs, but antibiotics are not the key means of therapy.
How to treat?
Many readers doubt whether chronic bronchitis can be cured?
Doctors answer positively: the chronic form is curable, but this will require a lot of effort.
The principles of treatment should be divided depending on the stage of the disease at which therapy is carried out.
During exacerbation, treatment differs little from that of the acute form. This implies a whole range of measures:
- taking antiviral drugs and antibiotics;
- bronchodilators and antispasmodics in the form of tablets and inhalations;
- corticosteroids;
- immunostimulating therapy;
- folk remedies.
If the temperature rises above 38 degrees, you can give your child antipyretics.
Among the antibiotics suitable for treatment are the group of macrolides and cephalosporins. The most common ones include:
Depending on the nature of the cough, mucolytics and other expectorants are prescribed:
Saline and alkaline solutions for inhalation are excellent. You can add Borjomi or saline solution to the nebulizer. Pulmicort or Fluimucil are used as expectorants.
Don't forget about breathing exercises and massage. These measures are very useful during periods of exacerbation of the disease.
In severe forms, the child undergoes treatment in a hospital. When remission occurs, the baby needs continued treatment in a sanatorium. Doctors advise taking children to the sea and to the forest. A sanatorium is preferable because the baby will receive medical care there.
If a child has chronic bronchitis, treatment with folk remedies can be continued at home.
Manifestation of exacerbation: symptoms
The main symptom of chronic bronchitis is cough. When it intensifies, we can talk about a relapse of the disease. Sometimes the cough becomes painful and provokes a severe headache.
During remission of bronchitis, the cough becomes dry, and little mucus is released. The cough may be accompanied by wheezing. If chronic bronchitis is in the acute stage, then the volume of sputum increases sharply.
Chronic bronchitis is a pathology during the development of which the bronchial mucosa functionally changes:
- the mechanism of bronchial mucus secretion is damaged;
- the mechanism for clearing mucus in the bronchi is deformed;
- bronchial immunity weakens;
- the walls of the bronchi become inflamed and thicken.
Chronic bronchitis develops quite quickly, since the bronchial mucosa is constantly affected by viruses that are in the air.
The main symptoms of exacerbation of chronic bronchitis:
- shortness of breath even when walking;
- nausea;
- sweating;
- weakness of the body;
- wheezing during breathing;
- the tips of the nose and ears, fingers and toes turn blue;
- sleep is disturbed;
- the level of performance decreases;
- dizzy;
- increased heart rate even at rest;
- Strong headache.
A cough in chronic bronchitis can be dry or wet. The volume of sputum produced per day is less than 150 grams. Sputum has a different character: watery, transparent, mucous, with blood or purulent impurities.
During an exacerbation, greenish pus forms in the mucous membrane. When such sputum appears, the microbial flora is activated. In this case, you should immediately consult a doctor so that he can adjust the treatment.
Wheezing almost always occurs during an exacerbation, due to the fact that the lumens of the bronchi are clogged with mucus.
During an exacerbation, the patient most often suffers a viral or bacterial infection. He is its carrier. The doctor assesses the severity of the disease based on severe symptoms and external respiration indicators.
Symptoms and signs
- Sore throat.
- A constant cough that lasts for quite a long time.
- Plaque in the throat on the tonsils, but the throat does not turn red.
- Appetite disappears, skin turns pale.
- At times the patient gets better, but symptoms may recur.
When bronchitis is dangerous:
- treatment started late;
- recommendations prescribed by the doctor are not followed;
- the patient's immunity is weakened;
- smoking and bad habits.
To prevent complications, you need to consult a specialist in time. It is best to get tested, then the cause of the disease will be clear. If it turns out that bronchitis is obstructive, then you need to take a course of antibiotics. If the cause is viruses, then antiviral drugs will help.
We recommend that you read about the treatment of bronchitis with antibiotics in adults in this material.
Features of treatment of bronchitis without fever
Symptoms of bronchitis, not accompanied by fever, with proper treatment disappear within 1-2 weeks. It is difficult for young children to cough up mucus themselves, so the disease lasts longer, about a month.
Therapy is carried out in the same way as for ordinary bronchitis accompanied by fever:
1. Bed rest. Regardless of the type and degree of development of the pathology, the patient must be prescribed bed rest.
2. Nutritional features. All sweet and sour foods are removed from the patient’s menu, as they have an irritating effect on the mucous membranes. If a child is sick, feeding is done only at his request.
3. Drinking plenty of fluids. To thin the mucus and improve the process of its removal, you need to drink as much warm liquid as possible; you should avoid drinking hot drinks.
4. Humidity of air masses. The air in the room should not be dry. Very humid air also has a negative impact on health.
5. Ventilation. It is imperative to ventilate the entire home and the room where the patient is located as often as possible.
6. Features of breathing. The child should inhale and exhale air through his nose. If nasal congestion is detected, then medications are taken to constrict blood vessels (Tizin, Nazivin). Rinsing the nose can be done with Aquamaris and Aqualor; if they are not available, then a saline solution is perfect.
7. Antibacterial drugs. The disease can only be treated with antibiotics in combination with probiotics; if you use other groups of medications, there is a high probability of developing dysbiosis.
8. Antiviral agents. Used only in situations where the disease is caused by viral infections.
Medicines must be prescribed by doctors. In the case of self-medication in infants, complications may arise that simply cannot be avoided without hospitalization. Therefore, before using any folk remedies, you need to consult a doctor.
Recommendations for patient care
In the first week of illness, it is recommended to stay at home and stay in bed or semi-bed rest. After this, if the person feels normal, he can go outside, however, avoiding excessive physical activity, since with bronchitis it is recommended to spend more time in the fresh air.
People with bronchitis should drink more fluids than usual. An adult patient is recommended to drink up to 2-3 liters of water per day. Berry teas, mint, linden tea, juices are useful. During illness, it is advisable to limit the consumption of drinks containing caffeine. The patient needs to eat more vegetables and fruits, dairy products, as well as cereals and broths. Spicy and salty foods are excluded from the diet.
The room in which a patient with bronchitis is located must be well ventilated. Dr. Komarovsky recommends maintaining air humidity in the room at least 60% and ensuring that the patient does not overheat (the air should be cool).
Patients who have had bronchitis are advised to undergo sanatorium-resort treatment and visit salt mines.
Treatment
By medication
The following groups of drugs are used to treat chronic bronchitis:
- Antibiotics. They are prescribed for exacerbation of the disease, in which symptoms of intoxication occur, the temperature rises, or a large volume of mucopurulent sputum is released. Here are some names of antibiotic tablets for bronchitis in adults:
- Semi-synthetic aminopenicillins (Augmentin, Amoxiclav).
- Macrolides (Azithromycin).
- Cephalosporins (Ceftriaxone, Cefuroxime).
- Fluoroquinolones (Lefofloxacin, Avelox).
Antibiotics are prescribed only after the results of sputum culture.
- Expectorant drugs (ACC, Lazolvan, Flavamed, Bromgesin). These medications are always prescribed for the treatment of chronic bronchitis. There are two groups of expectorants: sputum disintegrants (thin sputum) and expectorants (improve mucociliary clearance).
- Bronchodilators and anti-inflammatory drugs. They help improve bronchial patency due to the fact that they expand the lumen of the respiratory tract.
- Relaxes the smooth muscles of the bronchi (Theophylline, Neophylline).
- Anticholinergics (Atrovent, Spiriva).
- Adrenergic receptor agonists (Berotec).
- Reducing inflammation and secretion of bronchial mucus (Fluticasone).
- Combined medications for bronchitis and cough in adults (Seretide, Berodual).
In addition, treatment can be supplemented with inhalation procedures and physiotherapy.
Folk remedies
Let's consider several effective folk remedies that can complement the main treatment of bronchitis:
- Pour one glass of milk into an enamel pan, add one tablespoon of dry sage herb, cover with a lid and boil over low heat. After this, cool and strain. Then boil again. Drink a hot drink before bed.
- Boil the potatoes in their skins, mash, add one tablespoon of vegetable oil and two or three drops of iodine. Mix everything. Place the mixture on a cloth and apply to your chest. Wrap something warm on top. It is advisable to carry out the procedure at night.
- Drink a teaspoon of fresh cabbage juice with sugar several times a day.
- Pour one tablespoon of linden flowers into one glass of boiling water, cover, leave for an hour, strain. Drink one glass two to three times a day.
This article will answer the question of whether chronic bronchitis can be cured forever.
Diagnostics
Bronchitis requires targeted treatment, that is, it is not enough to suppress the disease with antibiotics. Perhaps bronchitis will recede in this case, but most likely it will return again at the slightest weakness of the immune system.
Various types of infectious pathogens can cause bronchitis in humans:
- bacteria;
- viruses;
- mushrooms.
Expectorants for bronchitis
To eliminate cough, medications are needed to stimulate expectoration and drugs that dilute sputum. The action of secretomotor agents is aimed at irritating the mucous membrane, due to which the work of the cough and vomiting centers of the brain is enhanced, the production of liquid secretion is increased and the cough reflex is strengthened. The main drugs in this group are ammonium chloride, thermopsis herb, and some essential oils. The drugs have a short-term effect, and an overdose can lead to lacrimation, nausea and vomiting, and nasal congestion.
Mucolytics (medicines that dilute sputum, but do not lead to an increase in its quantity) are usually prescribed as follows: Bromexin, Trypsin, Ambroxol, Alteyka, Doctor MOM, Ambrobene. "Trypsin" has an anti-inflammatory effect and is contraindicated only in case of individual intolerance to the components. "Ambroxol" is a classic mucolytic that significantly facilitates expectoration of sputum. The variety of release forms allows the drug to be used even for the treatment of newborns, and Ambroxol has almost no side effects.
"Bromhexine" has no contraindications (except for the first trimester of pregnancy), does not have a toxic effect on the body and is quite effective. “Doctor MOM” expands the lumen of the bronchi and additionally has an anti-inflammatory and anti-edematous effect. The medicine can cause allergies, so it can only be used as prescribed by a doctor. “Alteika” is a plant-based preparation (marshmallow root). You cannot use Alteyka for a dry cough, because the composition stimulates the cough, vomiting and respiratory centers (the cough may intensify).
Folk treatment of chronic bronchitis is actively used. A good expectorant is milk with onions. To prepare the medicine, you need to chop half an onion, pour a glass of milk and cook over low heat for ten minutes. The milk should turn beige-yellowish. Afterwards, the boiled onion must be removed. Take the medicine warm or hot before bedtime. You can prepare another (folk) remedy for chronic bronchitis: chop the head of an onion, mix with honey in equal proportions, take a teaspoon after each meal. The mixture should be stored in the refrigerator.
Lifestyle and regimen of a patient with bronchitis
For chronic bronchitis, doctor's recommendations include changes in routine and lifestyle. It is necessary to provide the most comfortable environment for the natural restoration of the respiratory system. Drinking plenty of fluids (water, juices, herbal teas, fruit drinks at a comfortable temperature), using humidifiers, bed rest (especially in the first days of illness) and lack of physical activity are recommended. Short walks are permissible only after the patient’s condition has improved. It is important to completely stop smoking, because inhaling tobacco smoke can not only slow down recovery, but also cause complications.