Lung abscess is an inflammatory disease, otherwise called abscess pneumonia.
Infectious lung diseases are one of the most common reasons for patients to visit a doctor. Most often, the infection manifests itself as pneumonia. One of the most dangerous inflammations is a lung abscess, which has a clear clinical picture and quickly worsens the patient’s general condition.
Lung abscess is characterized by purulent-destructive manifestations. During the inflammatory process, one or more internal abscesses (cavities) are formed in the lungs (in the parenchyma) with pus. Inflammation is accompanied by intoxication and fever.
According to statistics, the pathology is most often diagnosed in men of working age. Moreover, the majority (2/3) of the patients abused alcohol. This is food for thought.
Lung abscess - what is it?
For reference. An abscess is a local purulent inflammation that looks like a cavity filled with pus.
The very name of the pathology in Latin is written abscessus - which means abscess. From a medical point of view, it is customary to say that the same abscess is formed by melting tissue. A cavity is formed, bounded by a film (pyogenic membrane). And inside this cavity pus collects.
Abscesses can occur in all parenchymal organs, as well as in the skin, subcutaneous tissue and other soft tissues. They arise due to the penetration of pyogenic microorganisms into the tissue and only under the condition of intact immunity.
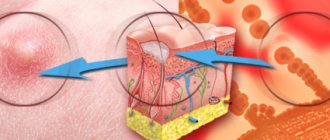
A lung abscess is a situation in which bacteria penetrate the parenchyma of the organ.
This happens in three ways - through the bronchi, with the blood flow or with the lymph flow. Once in the lung tissue, microorganisms provoke inflammation and destroy the parenchyma.
For reference. Immune cells, primarily neutrophilic leukocytes, rush to the site of penetration of foreign agents. They limit inflammation by creating a leukocyte wall. This is the wall of the abscess, called the pyogenic membrane.
A lung abscess is an inflammation in which a cavity is formed filled with pus, which can empty (drain) on its own through the adjacent bronchus.
Some abscesses are characterized by recurrent filling with pus after a bowel movement.
Description and etiology of the disease
An abscess is a limited cavity that fills with pus (visible in the photo). The abscess wall performs a protective function - it limits the spread of infection to surrounding tissues.
The reason for its formation is the entry of bacteria into the lung tissue, which leads to its purulent melting.
There are several ways of spreading the infection: contact, bronchogenic, hematogenous and lymphogenous.
In most cases, acute abscess develops as a complication of pneumonia. The causative agents are nonspecific microorganisms: streptococci, pneumococci, Staphylococcus aureus.
Several factors contribute to the development of infection:
- Complication of pulmonary infarction (secondary infection).
- The patient has chronic diseases that reduce local and general immunity: diabetes mellitus, alcoholism, lung diseases, bronchiectasis, HIV infection.
- Aspiration of infected contents of the nasal cavity, paranasal sinuses, tonsils.
- Aspiration of vomit.
- The entry of bacteria into the lung tissue by hematogenous route (with blood flow) from foci of osteomyelitis.
- Entry of bacteria by the lymphogenous route (with lymph flow) with furunculosis, phlegmon in the facial area.
Lung abscess - causes
The etiological factors of an abscess can be pyogenic bacteria, fungi, or, less commonly, protozoa. The latter includes
amoebic abscess.
The causes of a lung abscess may be as follows:
- pneumonia and pneumonitis;
- bronchiectasis;
- tuberculosis process;
- heart attack and gangrene of the lung;
- purulent diseases of the dental apparatus, for example, caries;
- aspiration of stomach contents during vomiting;
- sepsis in the stage of septicopyemia.
For reference. A lung abscess is most often a secondary disease, meaning that somewhere in the body there is a focus of endogenous infection.
Very rarely, primary abscesses occur when microorganisms enter the lungs from the environment and inflammation immediately follows the path of abscess formation.
Microorganisms can enter the lung parenchyma in three ways:
- Bronchogenic. In this case, the pathogen either initially enters the body through the bronchi, or is located in the oral cavity, from where it enters the lung along with the air.
- Lymphogenic. This path is carried out if the source of infection is in the lungs or nearby tissues and the microorganisms move through the lymph.
- Hematogenous. The process of spreading the pathogen through the bloodstream is called sepsis. If purulent foci occur in different organs due to the movement of microorganisms through the blood vessels, they speak of septicopyemia.
For reference. Separately, we can consider the option when the abscess is the result of resolution of pneumonia or pneumonitis. In this case, the lung abscess is not a complication, but an outcome of another disease.
Complications
Acute lung abscess can lead to some (often life-threatening) complications. These are:
- transformation of acute lung abscess into chronic;
- breakthrough of the abscess not into the bronchus, but into the pleural cavity with the formation of purulent pleurisy or pyopneumothorax (this danger is fraught with peripheral abscesses located at the borders of the lung);
- bleeding into the bronchial cavity (occurs if purulent masses melt the wall of a blood vessel) - in severe cases, when there is a lot of blood, it blocks the lumen of the respiratory tract and asphyxia occurs - the person suffocates);
- spread of pus into healthy bronchi with further formation of abscesses there;
- entry of the pathogenic microorganism into the bloodstream with the subsequent formation of abscesses in remotely located organs, including the brain;
- bronchopulmonary fistulas;
- bacteremic shock, RDS syndrome.
Complications develop mainly in the absence of timely treatment of the abscess or in the case of an immunodeficiency state in the patient.
Lung abscess - symptoms
For reference. The symptoms of this disease can be divided into two syndromes:
- general infectious,
- respiratory.
The first occurs as soon as the disease begins. It manifests itself as fever, weakness, aching muscles and joints, and fatigue. An abscess, especially of bacterial origin, is characterized by severe intoxication with high temperatures.
Respiratory syndrome is manifested by a cough with sputum production. A productive cough is evidence that the abscess is draining through the bronchus. The amount of sputum depends on the size of the abscess and the diameter of the bronchus with which it is connected.
Attention! The larger the abscess cavity and the wider the bronchus, the more sputum patients can cough up both at one time and throughout the day. Sometimes up to 1000 ml of yellow-green sputum with an unpleasant odor can be discharged per day.
Other symptoms may also develop, but they are less common and only if certain conditions are met. Chest pain of severe intensity associated with the act of breathing occurs if the abscess is located close to the pleura.
A dry cough, even before the contents break into the bronchus, can occur if a large abscess compresses the bronchial tree.
It is worth considering that the general infectious syndrome is well expressed in the first phase of the disease, when the abscess is closed. In the second phase, when the outflow of pus occurs, intoxication decreases significantly, and body temperature gradually normalizes.
Symptoms
Patients with lung abscess are bothered by chest pain, unproductive or unproductive cough, and shortness of breath.
During a single abscess, as a rule, there are 3 stages:
- maturation, or infiltration;
- rupture of an abscess into the bronchus;
- outcome.
The first stage is accompanied by acute inflammation of a section of lung tissue and its purulent melting. In terms of symptoms, it resembles pneumonia. The patient complains of general weakness, chills, sweating, and increased body temperature. All these are symptoms of intoxication of the body with substances released by bacteria. The person also notices chest pain and shortness of breath (it occurs both due to intoxication and due to the fact that part of the lung does not function and respiratory failure develops).
Objectively, the chest on the affected side lags behind the healthy half in the act of breathing. Over the forming abscess, percussion (tapping) reveals a dullness of sound, palpation (palpation with fingers) reveals a weakening of vocal tremor, and auscultation (listening with a phonendoscope) reveals rapid, hard breathing, dry or moist fine-bubble rales over the affected area. Tachycardia is recorded (heart rate exceeds normal). The abscess usually matures within 2-3 weeks.
The beginning of the second stage of the disease can be considered a breakthrough of the abscess into the bronchial cavity. At the same time, the contents come out of it, and, in the literal sense, a mouthful. During the day, the volume of purulent sputum can reach 1.5 liters and this process is accompanied by an unpleasant and often fetid odor. After the abscess breaks through, the patient’s condition improves - body temperature drops to subfebrile levels, chest pain becomes less pronounced, shortness of breath is less intense. Objectively, as the abscess is freed from pus, an increasingly tympanic percussion sound and auscultatory amphoric breathing with moist small-, medium- and large-bubble rales are determined.
At the exodus stage, the opened abscess is gradually replaced by connective tissue. The patient notes that there is less sputum, coughing less frequently, and body temperature values have returned to normal.
If the drainage of sputum is impaired for any reason (for example, the bronchus into which the abscess ruptured is small in diameter and located in the upper part of the cavity), purulent inflammation drags on, chronic purulent bronchitis is formed, and after 60-90 days the abscess is also regarded as chronic .
Multiple lung abscesses: features of the course
They are usually difficult. They occur predominantly against the background of destructive pneumonia. The inflammatory process affects large areas of the lung. Children and young people get sick more often.
The person's condition is getting worse every day. Already in the first days, a pronounced intoxication syndrome is detected, after which sepsis often develops.
A breakthrough of one of the purulent foci into the bronchus does not lead to relief of the patient’s condition. Foci of necrotic tissue quickly increase in size. Purulent bronchitis develops with a large amount of foul-smelling sputum. The patient's condition rapidly deteriorates, and multiple organ failure soon develops. Delay in surgery leads to the death of almost all such patients.
Features of the course of the abscess
An abscess goes through several phases in its development - from the formation of inflammation to its resolution, from filling the cavity to its emptying and healing.
Under the influence of an etiological factor, inflammation gradually spreads from the center to the periphery. Dead neutrophilic leukocytes, together with fragments of necrotic lung and dead bacteria, form pus.
For reference. Around the pus, a so-called pyogenic membrane appears, consisting of living neutrophilic leukocytes and other immune cells.
Thus, a cavity is formed, the walls of which are several rows of immune cells closely located to each other, and the contents are purulent exudate.
Over time, the abscess can break through the wall of the bronchus, causing the contents of its cavity to come out. Drained abscesses gradually empty and then either heal or become chronic.
For reference. An abscess is cured by organizing it, that is, replacing the cavity with connective tissue formed by fibroblasts.
Fibroblasts are cells that synthesize collagen, the main element of connective tissue; they are always present in the wall of a lung abscess. If the cavity is emptied and there is no longer inflammation in it, it heals.
If the lung abscess is not completely sanitized and the pyogenic membrane continues to produce pus, the connective tissue begins to grow along the periphery of the abscess. Thus, the outermost layer, fibrous, appears in the wall of the cavity. This is how a chronic abscess occurs.
Symptoms
The clinical picture of a lung abscess depends on the form and stage of the disease. In the acute phase, symptoms differ before and after opening the abscess. The abscessation process lasts on average a week and a half and is accompanied by severe manifestations.
Patients suffer from fever, chills, sweating and shortness of breath. The cough is dry and insignificant at first, then becomes annoying and is accompanied by chest pain. When you press on the chest in the area of inflammation, severe discomfort is felt. If the purulent cavity is shallow, hard breathing and moist rales can be heard. When infected with aerobic bacteria, the symptoms are more pronounced.
A couple of days before opening the cavity, a small amount of mucus and pus is released, and hemoptysis is possible. There is an unpleasant odor from the mouth. A breakthrough of the abscess is accompanied by copious discharge of yellow-green sputum. You may expectorate brown mucus. It comes out full of mouth, 250-400 ml of pus and mucus are released per day. In some cases, the volume of discharge reaches a liter. The patient's general condition improves, the fever subsides.
Sputum from a lung abscess is stratified. If you hold it in a container, at the bottom there will be a thick and dense layer of gray color with particles of lung tissue. Next comes liquid sputum mixed with saliva. The surface of the mass is foamy and consists of serous fluid.
Symptoms of chronic lung abscess depend on the number of cavities, the size of the capsules, and the degree of pneumosclerosis. The clinical picture may be blurry and consist of a cough with sputum and a slight increase in temperature. In other cases, the patient's condition is more severe. They experience hemoptysis and secrete a large amount of foul-smelling purulent mucus. At the same time, signs of fever, chills, shortness of breath, and sweating remain. Patients lose weight. Increased fatigue is noted.
External signs include changes in the hands. The phalanges thicken, the fingers become like drumsticks. Nails take on the appearance of watch glass. Patients also develop an unhealthy blush.
The main tool for diagnosing lung abscess is radiography.
Lung abscess - classification
According to the flow, abscesses are divided into two types:
- Acute - arose less than two months ago, has a thin pyogenic membrane, has opened or not opened into the bronchus;
- Chronic - existing for more than two months, having a thick capsule with proliferation of connective tissue along the periphery, usually periodically drained by the bronchus.
For reference. An acute abscess does not necessarily become chronic. If the cavity is completely emptied, the process can be resolved.
The pyogenic membrane gradually resolves, and a patch of connective tissue forms at the site of the abscess. If the cavity was small in diameter, after it has healed, no residual effects may be visible. If the cavity was large, an area of fibrosis remains.
Chronic lung abscess is more dangerous; it has a protracted course and can exist for decades.
The danger of chronic pathology
For reference. Chronic lung abscess is characterized by a recurrent course. The cavity is either filled with pus or emptied. Exacerbations may occur several times a year.
Each exacerbation is accompanied by the same symptoms that are characteristic of an acute abscess. At the same time, connective tissue gradually grows around the pathological focus, forming coarse fibrous cords.
Attention. The danger of the chronic course of the disease lies in the possibility of developing respiratory failure.
A long-term pathological focus in the lung leads to disruption of the functioning of the bronchopulmonary system. Symptoms such as constant shortness of breath, exercise intolerance, and cyanosis of the skin develop. Over time, the cardiovascular system also begins to suffer, which can lead to heart failure.
The presence of a cavity in the lung for a long time creates a risk of damage to the pleura. Any trauma to the chest can lead to rupture of the abscess wall and the formation of pneumothorax, which will have to be treated surgically.
For reference. Another danger is the development of complications associated with the long-term existence of a source of chronic infection in the body. These complications include amyloidosis of parenchymal organs, decreased immunity, and the gradual development of multiple organ failure.
Types of suppurative lung disease
Depending on the nature of inflammatory lung disease, the following types are distinguished:
- Acute abscess (another name is abscess pneumonia). It is expressed in putrefactive lesions and melting of painful tissues in the lung.
- Gangrenous abscess is the period between the development of gangrene of the lungs and the appearance of an organ abscess.
- Chronic lung abscess is diagnosed if the disease lasts more than 2 weeks and the patient's condition worsens. Accompanied by febrile exacerbations, acute pain in the side, profuse sputum.
- Purulent pathology is expressed in the form of gangrene of the respiratory organ.
go to top
Diagnostics
For reference. Lung abscess is diagnosed by collecting complaints, medical history, objective and additional research methods. Moreover, the last two listed points have the greatest diagnostic significance.
The diagnosis of lung abscess can be made using the following research methods:
- Physical. If the abscess has a small diameter and is located deep enough in the lung, it is impossible to detect it using physical examination methods. Large and superficial abscesses can be identified by auscultation and percussion. On auscultation, weakened bronchial breathing is heard over an undrained abscess, and amphoric breathing is heard over a drained abscess. Percussion over a filled abscess determines the dullness of the sound, over an empty abscess - its boxy tone.
- Laboratory. A general blood test does not confirm or refute the presence of an abscess, but allows you to see inflammatory changes in the blood. In this case, there is an increase in neutrophil leukocytes and a shift in the leukocyte formula to youthful forms. In severe cases, anemia may develop.
- Plain radiography of the chest organs. The radiographic picture depends on the stage of the pathological process. An undrained abscess looks like a rounded darkening with clear, even contours. A drained abscess looks like a cavity with a horizontal level of fluid. If the cavity is thin-walled, the abscess is acute; if its walls are thick, it is chronic. As the disease progresses, signs of fibrotic changes appear around or inside the abscess.
- Computer or magnetic resonance imaging. They are the same methods for visualizing the lungs as x-rays. However, CT and MRI make it possible to view lung tissue layer by layer and create a three-dimensional projection. This is necessary to determine the exact location and size of the abscess.
- Sputum analysis. It is carried out in a special laboratory after collecting sputum in a sterile container. Using microscopy, it is possible to detect a large number of neutrophilic leukocytes and bacteria in sputum. In addition, a bacteriological study is carried out to identify the type of pathogen and its sensitivity to antibiotics.
- Bronchoscopy. This type of research is performed very rarely. It is necessary in cases where it is necessary to speed up the process of draining an abscess or carry out a differential diagnosis with bronchial diseases.
Etiology of the disease
The main reason for the development of an abscess is the penetration of bacteria into the lung by the bronchogenic route: Staphylococcus aureus, Escherichia coli, pneumococcus, peptococcus. Another pathology develops due to the entry of a foreign body into the bronchi. Thus, an abscess is caused by the following diseases and conditions:
- periodontal disease;
- tonsillitis;
- gingivitis;
- pulmonary infarction;
- wounds and direct damage to the chest;
- thrombophlebitis;
- bronchiectasis;
- septicopyemia;
- lobar or viral pneumonia;
- tumors, scars that narrow the lumen of the bronchus;
- entry of vomit into the bronchi.
Flow options
The process of abscess formation of lung tissue can occur in different ways. In total, there are three main variants of the course of this destructive pathology:
| Flow option | Description |
| Abscess formation type 1 | It develops approximately 1.5–3 weeks after the onset of pneumonia against the background of the usual dynamics of inflammation. The patient's condition improves, but then the temperature rises again, chest pain appears, and intoxication increases. It all ends with the release of purulent sputum. |
| Abscessation type 2 | Occurs within 3–4 weeks after the onset of pneumonia and looks like its protracted form if treatment is unsuccessful. The patient has a constantly high temperature and intoxication. The amount of purulent sputum is constantly increasing. |
| Abscessation type 3 | Destruction in the lung occurs from the very first days of the disease, an abscess occurs after 5–10 days. Pathology leads to aspiration processes. |
Treatment of lung abscess
Lung abscess is treated conservatively or using surgical methods.
For reference. The possibility of drug treatment of a purulent lesion in this case is due to the fact that it drains independently.
As a rule, with any purulent infection, surgeons are forced to proceed with surgical intervention in order to ensure the outflow of pus. An abscess can empty on its own.
Acute drained lung abscess can be treated conservatively. First of all, etiotropic therapy is used, affecting the causative agent of the infection. For this purpose, broad-spectrum antibiotics are used first, and then based on the results of an antibiogram.
Additionally, nonsteroidal anti-inflammatory drugs, such as ibuprofen, are prescribed. They help reduce the temperature and speed up the healing process.
An important condition for recovery is complete rest for the patient and a high-calorie diet rich in protein foods and vitamins.
Methods of surgical treatment
For reference. A lung abscess is treated surgically if it does not drain on its own or becomes chronic.
An abscess can be drained through the bronchial tree. To do this, drainage is carried out using a bronchoscope and the contents of the cavity are sucked out. It can then be sanitized by introducing antibacterial drugs into the cavity.
Chronic abscesses must be removed. As a rule, it is not possible to isolate them on your own. To do this, a segmentectomy is performed - removal of a segment of the lung or lobectomy - removal of a lobe.
If more than one lobe is involved in the pathological process, a pneumonectomy is performed - removal of the lung. The last of these operations for an abscess is performed extremely rarely.
Diet
During the treatment of a lung abscess, diet therapy is of great importance, helping to strengthen the body during the fight against the disease and speed up recovery. When starting treatment, try to follow the following rules:
- Limit your salt intake. Since salt retains fluid, which, in turn, causes stress on the cardiovascular system, you need to reduce its daily amount in the diet.
- Avoid alcohol, which has a harmful effect on body tissue. In this case, it is important to determine whether the patient previously suffered from alcoholism, since this disease greatly worsens the prognosis of treatment for a lung abscess.
- Eat protein foods of animal origin regularly.
- Include foods containing calcium in your diet. These can be various dairy products. The daily consumption of this element should be at least one and a half grams.
- Focus on vegetables and fruits rich in minerals and vitamins A and.
- Introduce yeast into your diet as an additive to various dishes. They contain a large amount of vitamin B, which is so necessary during the treatment of purulent diseases. In addition, yeast contains carbohydrates, fats, folic acid, and various minerals. It is best to simmer the yeast in a water bath, mixing it with water at the rate of 2.5 parts liquid to one part yeast.
Trofimova Yaroslava, medical observer
14, total, today
( 189 votes, average: 4.58 out of 5)
Open pneumothorax: causes, signs, treatment
Breathing exercises for coughing for adults and children
Related Posts
Prognosis and prevention
For reference. The prognosis of the disease with timely treatment of acute abscess is favorable.
Complete recovery or minor residual effects may occur. With a chronic abscess, the prognosis is questionable, since it is quite difficult to treat and poses a health hazard. If irreversible complications of the disease develop, the prognosis is poor.
Prevention of lung abscess, first of all, is the treatment of primary foci of endogenous infection. For this, it is important to timely consult a doctor if your health worsens and general infectious manifestations occur.
Risk factors
There are several factors that increase the risk of abscess formation:
- elderly age;
- heart diseases;
- diabetes;
- immunodeficiency;
- hypothermia;
- alcoholism;
- addiction;
- smoking;
- tuberculosis;
- COPD;
- lungs' cancer;
- Chronical bronchitis;
- influenza and other colds;
- immobility in bedridden patients;
- long-term use of potent drugs: cytostatics, corticosteroids, etc.;
- inflammatory diseases of the nose and throat;
- bronchiectasis.
Questions for the doctor
Causes of pathology
3 months ago I fell ill: my temperature rose and I started coughing. I thought it was a simple cold, I was treated as usual - Paracetamol, took cough drops. Then it got worse, the temperature stayed at 40-41 degrees, it was not going well, and shortness of breath began. They took me to the hospital, did an x-ray, and it turned out there was an abscess in my right lung.
Now I'm on antibiotics and I feel much better. But I have a couple of questions. This is an infectious disease, right? So, did I get it from someone? Can I get it again?
Hello! An acute abscess is more likely a complication of an infectious disease - bronchitis, bronchiolitis or pneumonia. Indeed, some pathogen entered your body (probably through airborne droplets) and caused inflammation of the lower respiratory tract, which you mistook for a cold. Without proper treatment, the immune system could not cope with the infection on its own and “reacted” to it in a similar way - by forming a cavity filled with pus.
Repeated abscess formation of lung tissue is possible. To avoid this, try to follow the principles of a healthy lifestyle and treat lung infections in a timely manner. Be healthy!
Treatment options
Treatment of a lung abscess can be medicinal and surgical. The choice of tactics depends on the severity of respiratory damage and the effectiveness of medications.
Conservative treatment
It is carried out in a hospital in the pulmonology department. In some cases, the discharge of sputum emits such a stench that therapy in the general ward is impossible. Patients are prescribed antibiotics in large doses. The drugs are administered intravenously; in uncomplicated disease, oral administration is possible.
Mucolytics thin the mucus, and expectorants promote its better removal. These drugs are taken in the form of tablets and inhalations. Immunomodulators are also needed to strengthen the body's defenses.
To improve the discharge of mucus and pus, a drainage position is used. To do this, the patient lies on a bed, the foot of which is raised by 20-30 cm. Postural drainage, vibration chest massage and physiotherapy are usually not used, since these manipulations contribute to the spread of infection and the occurrence of airway obstruction.
To wash the bronchi, use lavage with antiseptic solutions. About 10% of patients who do not respond to medications require sputum drainage using bronchoscopy. The procedure is also advisable for the development of gangrene. Its essence lies in the introduction of antibiotics, antiseptics and thinning drugs into the cavity of the bronchial tree using a special apparatus under anesthesia.
A special diet plays an important role. It helps strengthen the immune system and speed up recovery. Of course, you need to give up alcohol. You should reduce your salt intake, as it retains water in the body, which puts additional stress on the heart and blood vessels. It is necessary to include more animal protein in your diet. Of the microelements during this period, the body needs to replenish the deficiency of calcium, vitamin A and B.
A special protein diet plays an important role in treatment
Surgical intervention
If there are no results from conservative treatment, after 6-8 weeks the patient is transferred to the surgical department. There he undergoes sanitation of the abscess cavity. To do this, an incision is made in the chest, a tube is inserted into it, and the pus is drained from the lung. This method is indicated for small sizes of the source of infection and its location in the marginal parts of the organ.
With a single cavity of small size, partial resection of the affected tissue is possible. If there are multiple lesions or gangrene has begun, the affected lung is completely removed.
Prevention measures
There is no specific prevention. General measures include quitting smoking and drinking alcohol. It is important to avoid hypothermia and promptly treat colds and inflammatory pathologies of the lungs, bronchi and trachea.
Don't forget about oral hygiene. Regular sanitation of the oral cavity and adequate treatment of caries, gingivitis and other pathologies of teeth and gums are necessary.
Foreign objects should be prevented from entering the respiratory tract. This is especially true for young children and patients with swallowing dysfunction. Proper care for bedridden patients is also necessary. You should remember the existing risk factors and, if they exist, regularly visit a pulmonologist or therapist.
Lung abscess is a dangerous disease. It causes physical and mental suffering and threatens with dangerous complications, including death. It is important to follow prevention recommendations and seek medical help at the first symptoms. The earlier the pathology is diagnosed, the easier it is to get rid of it without consequences.
What diseases can it be associated with?
It is clear to even the average person that this pathology does not appear out of nowhere. It occurs either against the background of some concomitant or previously suffered painful conditions, or in people from the so-called risk groups.
These include:
- people who abuse alcohol;
- smokers;
- people exposed to constant hypothermia;
- patients who have had the flu;
- patients with weakened immune systems.
Attention! If the body's defenses are reduced, then the likelihood of an abscess increases significantly. Therefore, if you have one or more symptoms, as well as belonging to one of the above categories, you should immediately consult a specialist.
The disease can also develop due to or against the background of:
- sepsis;
- bronchial obstruction;
- as a result of foreign bodies and stomach contents entering the airways;
- a history of pneumonia;
- disorders in the circulatory system;
- tonsillitis;
- pulmonary infarction;
- prostatitis;
- diabetes mellitus;
- periodontal disease.
Differential diagnosis
Chronic abscess must be differentiated from tuberculosis, actinomycosis, and cavitary form of peripheral lung cancer. The main diagnosis is carried out according to the same principles as when an acute form of purulent inflammation is suspected. Most patients with a chronic abscess have a history of previous purulent-destructive inflammation. Diagnostics includes the following studies:
- general urine analysis;
- general blood analysis;
- study of the hemostasis system;
- spirography;
- fibrobronchoscopy;
- X-ray examination;
- computed tomography of the lungs;
- biochemical blood test;
- electrolyte composition of blood.
Consequences of pus in the lungs
If a person is not provided with qualified assistance in a timely manner, pus can spread to the pleural cavity. Along with this, air also accumulates in it. As a result, the patient begins to experience shortness of breath and acute pain. When the disease progresses to an advanced stage, scars begin to form on the lung and bronchiecstasis develops. Inflammations begin to recur regularly and periodically become seriously aggravated.
Additional diagnostics
A purulent process in the lung can be assumed based on clinical data, but additional methods can confirm it. Laboratory and instrumental procedures help to clarify the pathogen and find out the nature of the disease:
- General blood test (leukocytosis, shift of the formula to the left, toxic granularity of neutrophils, acceleration of ESR).
- Blood biochemistry (indicators of the acute phase of inflammation, liver tests, protein, coagulation and immunogram).
- Sputum analysis (cytology, culture, antibiotic sensitivity).
- Chest X-ray.
- Bronchography and bronchoscopy.
- CT scan.
- Spirometry.
Electrocardiography and cardiac ultrasound are also becoming necessary diagnostic elements. And having established the reason why pus accumulates in the lungs, you can begin to treat the pathology.
During additional diagnostics, the causative agent of the infection, the nature of the disease and accompanying changes are determined.
Classification
A generally accepted classification of the disease has not yet been developed. The main ways of dividing it according to various criteria are presented in the table below.
Table 1: Classification of pulmonary abscesses:
| Classification | Description | Possible types |
| Etiological | Based on the isolation of the infectious agent | Pneumococcal |
| Staphylococcal | ||
| Streptococcal, etc. | ||
| Pathogenetic | Based on how the lung tissue became infected | Bronchogenic |
| Hematogenous | ||
| Post-traumatic | ||
| Topographical | Based on assessment of the location and number of purulent cavities | Central |
| Peripheral | ||
| Unit | ||
| Multiple | ||
| Unilateral | ||
| Double sided |
The photo shows a macropreparation with a fresh decay cavity