In 1832, the scientist Hodgkin described a strange disease, accompanied by severe enlargement of the lymph nodes, fever and severe exhaustion. The disease developed slowly, affected other organs, did not respond to treatment and usually ended in the death of the patient. The disease soon received the name “lymphogranulomatosis” or Hodgkin’s disease. What kind of disease is this, what are its underlying causes and manifestations, and how is it treated today?
What is Hodgkin's lymphoma
The disease is a malignant increase in the volume of lymphoid tissue. The primary localization of the tumor is a human lymph node (usually men aged 14–40 and over 50 years). Atypical cells begin to divide uncontrollably, the size of the tumor quickly grows, interfering with the normal functioning of the body. Benign neoplasms (such as lymphangiomatosis) also interfere with the functioning of organs.
During a malignant process, the functioning of the system is disrupted very quickly. The disease spreads from one node to another. Lymphomas differ from each other in terms of their level of aggressiveness (the degree of suppression of normal body functions). Follicular ones can be distinguished as slow-growing and well-treatable. Burkitt's lymphomas are considered aggressive.
Hodgkin's disease (the second name is lymphogranulomatosis) has code C 81 according to the International Classification of Diseases, 10th revision (ICD-10). It differs from other lymphomas in the presence of special Hodgkin cells and multinucleated Sternberg cells. The disease is similar to cancer, but differs from it in the following:
- the prognosis is favorable;
- Hodgkin's disease does not kill healthy cells;
- It is not the connective tissue that changes (as in the case of cancer), but the lymphoid tissue.
How to diagnose the disease?
To identify Hodgkin lymphoma, it is recommended to use the following types of diagnostics:
- Examination of the nasopharynx and tonsils by an otolaryngologist;
- Carrying out an excisional biopsy from a newly emerging lymph node;
- Palpation of lymph nodes of various locations and the spleen;
- Measurement of the rate of growth of lymph nodes;
- Studying the degree of intoxication of the body;
- Ultrasound examination (ultrasound) of the lymph nodes: neck, groin and thighs, supraclavicular and subclavian, axillary, peritoneum, as well as checking the spleen and liver;
- Study of platelet, erythrocyte and ESR levels;
- Computed tomography of cervical, thoracic, hip lymph nodes;
- Osteoscintigraphy of the skeleton (radionuclide visualization of the osteoarticular apparatus using the introduction of radiopharmaceuticals);
- X-ray of bones;
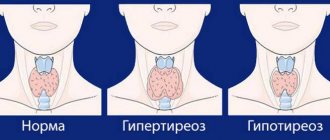
- Study of the level of thyroid hormones in case of damage to the cervical lymph nodes;
- Emission tomography (PET) is a radionuclide method for studying internal organs. According to the 5-point Deauville scale using PET, the effectiveness of diagnosing Hodgkin lymphoma is 5 points.
Causes
There is still no clear answer to the question of why lymphoma begins to develop. Oncologists name the following factors that stimulate the process:
- genetic predisposition;
- Epstein–Barr virus infection;
- poor environment, work in production with increased harmfulness;
- weakening of the immune system due to HIV infection, long-term use of medications, and immunosuppressive diseases.
Classifications
According to the generally accepted international classification, Hodgkin's disease has the following morphological variants:
- Lymphoid predominance, designated C81.0 (temporary form)
- Nodular sclerosis with code C81.1. The most common form, accounting for 50% of all cases, is characterized by the appearance of dense connective tissue strands dividing the lymphatic organs into “nodes.” During pathomorphological examination, the obligatory elements of this form are Berezovsky-Sternberg cells and lacunar cells. This form of lymphogranulomatosis is more common in women.
- Mixed cell type according to ICD C81.2. Corresponds to the second and third stages of the disease and accounts for approximately 30% of all cases. When studying biological material, many forms of lymphocytes, plasma cells, fibroblasts, etc. are determined. A different cell pool contributes to accelerated generalization of the pathological process.
- Lymphoid depletion C81.3
- Other forms of Hodgkin's lymphomas C81.7
- Hodgkin's disease, unspecified, coded as C81.9
Each variant of lymphogranulomatosis has stages of progression that reflect the prevalence of the pathological process throughout the human body.
- The first stage of Hodgkin lymphoma is characterized by local involvement in the pathological process of lymph nodes from one anatomical group and damage to 1 organ outside the lymph nodes.
- With stage 2 lymphogranulomatosis, lymph nodes from 2 or more groups on one side of the diaphragm, as well as organs and lymph nodes with similar localization are affected.
- Hodgkin's lymphoma stage 3 is characterized by damage to the lymphoid tissue on both sides of the diaphragm, both with and without involvement of the spleen and internal organs.
- Stage 4 Hodgkin's lymphoma diffusely affects the organs of the abdominal, thoracic cavities, bone marrow, etc. and multiple lesions of lymph nodes from different anatomical areas or without involving the latter in the oncological process.
Symptoms
The main symptom of lymphogranulomatosis is a severe enlargement of the lymph nodes in the neck, axillary or groin areas. This is clearly visible in the photo. The tissue of the nodes is elastic, they do not hurt when palpated. Other symptoms of Hodgkin lymphoma:
- difficulty breathing, persistent cough;
- causeless weakness;
- regular fever and heavy sweating at night;
- skin itching;
- sudden weight loss for no apparent reason.
Itching with lymphoma
One of the early symptoms of the disease is the occurrence of painful itching . It can appear long before changes in the lymph nodes, accompanied by a small rash on the surface of the skin of the chest or abdomen, arms and legs, and head. Unbearable itching can be localized in the area of the lymph nodes. This condition is very difficult for patients to tolerate and causes sleep disorders and mental health problems.
Temperature
A common symptom of the first stage of the disease is attacks of causeless acute fever. The temperature rises almost daily to febrile levels (38.5-40°C) and remains at this level for several hours. After a short-term chill, the patient sweats profusely, and the temperature drops to low-grade levels. As the disease progresses, the interval between attacks decreases.
Articles on the topic
- Melatonin - instructions for use of tablets, dosage, contraindications and reviews
- What are antibodies in the blood - why are they produced and what do they affect in the body, determination test
- What is lymphoma in adults and children
Symptoms and stages
Symptoms of Hodgkin lymphoma vary at different stages of the disease. The development of the disease occurs gradually, in several stages:
- At the first stage, damage to one group of lymph nodes is detected.
- On the second - 2 or more on one side of the diaphragm.
- The third is characterized by an increase in lymph nodes on 2 sides.
- The last, fourth stage occurs with the appearance of disorders in the liver, bone marrow and internal organs.
Important information: Signs of drug (oil) embolism and what to do to prevent it
The effectiveness and method of treating Hodgkin lymphoma depends on the degree of neglect of the pathological process.
Enlarged lymph nodes (lymphadenopathy)
They are most often affected in the area of the neck and lower jaw. Upon palpation, they are distinguished by elasticity, non-adhesion to tissues and lack of pain (these are the main symptoms of lymphogranulomatosis and its difference from infectious diseases). Lymphadenopathy begins earlier than other signs, most often against the background of absolute well-being.
Later, the lymph nodes can become large, the process begins to spread downward, and nodal formations of the mediastinum, abdomen, pelvic organs, and limbs are involved. Their compression of neighboring organs causes the main symptoms of lymphogranulomatosis:
- Irritation of the bronchi causes a constant non-productive cough, which does not go away after the use of antitussives.
- Lack of air. A mechanical obstruction does not allow sufficient oxygen to enter the lungs, and shortness of breath develops. Initially, it manifests itself during physical activity, and then at rest.
- Swallowing problems. When the lumen of the esophagus narrows, problems arise with eating solid food, and it gradually becomes difficult even to drink liquid.
- Compression by the lymph nodes of the inferior genital vein, which brings blood from the lower part of the body to the heart, stagnation occurs, then through the dilated vessels the liquid part of the blood leaks into the tissue and the development of edema.
- Problems with the passage of food through the intestines manifest themselves in the form of indigestion, alternating diarrhea and constipation, necrosis and obstruction.
- Damage to the kidneys (failure) and nervous system (impaired sensitivity and movement of the limbs) is much less common.
Symptoms due to damage to internal organs
Any tumor has a tendency to metastasize as it progresses. Hodgkin's disease is no exception. The appearance of an accumulation of lymphoid cells in the internal organs gives symptoms of their damage in lymphogranulomatosis:
- The spleen and liver enlarge, and liver failure develops.
- The process of hematopoiesis is disrupted when the bone marrow is damaged. This manifests itself in the form of aplastic anemia with a decrease in the level of all blood elements.
- The structure of the bones is disrupted, pain and fractures occur. The most commonly affected bones are the pelvis, sternum, ribs and vertebrae. Much less commonly, the problem affects the tubular bones of the limbs.
- On the part of the lungs, shortness of breath, persistent cough, and respiratory failure are noted.
- An increase in blood bilirubin, as well as the release of histamine from areas of inflammation, leads to severe skin itching.
These signs of Hodgkin lymphoma are nonspecific and can manifest themselves individually in each patient.
Systemic manifestations
General changes also characterize lymphogranulomatosis. The body is depleted, immunity decreases, and recovery reactions in the later stages do not work. Symptoms in adult patients with this disease are as follows:
- Increase and decrease in temperature. As you rise, you experience muscle aches and chills, and when you fall, copious amounts of cold sweat are released.
- Weakness, decreased performance. This happens in the later stages, when cancer cells grow rapidly and take away all the body’s strength. The person becomes sleepy, lethargic and apathetic.
- Weight loss. The sign indicates the last stage of the disease. First, the subcutaneous tissue disappears, and then the muscle fibers atrophy.
- Attachment of infections (viruses, fungi, pathogenic bacteria) as a result of decreased immunity and exhaustion. When using radiation and aggressive substances during treatment, the body's defenses are reduced even more.
Lymphogranulomatosis in children
Hodgkin's syndrome is not very common among children; it is diagnosed in only 1 in 100 thousand babies and never in infants under 1 year of age. The course of lymphogranulomatosis in children is different in that the disease affects most of the lymphatic system and affects many organs. The lymph nodes of the cervical region are the first to suffer, this provokes frequent inflammatory processes in the nasal and oral cavities. Then the tumor spreads, abdominal lymphomas appear, the spleen enlarges, the lungs and liver are affected.
The following symptoms should be the reason for a thorough examination of the child:
- shortness of breath, prolonged coughing attacks accompanied by chest pain;
- cardiac dysfunction;
- general weakness, fatigue;
- hyperthermia, increased sweating.
Causes
The reasons for the development of lymphogranulomatosis are not fully understood. There is a possibility that the disease is associated with the Epstein-Barr herpesvirus. The assumption of its involvement is based on special studies, according to which the virus gene is detected in 20% of biopsies.
Lymphoma often occurs due to a deficiency of the immune system (HIV)
According to statistics, regions with a high incidence of Hodgkin lymphoma include African countries, the USA, and Japan. It can occur at any age, but the peak of the disease occurs in two periods: from 15 to 35 years, or after 50 years. With the exception of children under 10 years of age, who are predominantly boys, the distribution of cases by gender is almost the same.
Lymphogranulomatosis in children accounts for almost 10% of the total number of cases. Hodgkin's lymphoma in adults over 50 years of age usually occurs with complications.
Risk factors for the disease:
- among the sick, 60-70% are men from 15 to 35 years old, or from 50 years old;
- burdened heredity: Cases of the disease occur three times more often in families where relatives have already had the disease, which suggests a genetic predisposition. However, children born to a sick mother do not develop the disease;
- conscious (for example, due to antitumor chemotherapy) or acquired (HIV) immunosuppression;
- Hodgkin's lymphoma in adults who work with radiation (eg, health care workers) or carcinogens.
During pregnancy
Hodgkin's disease during pregnancy involves one of 2 possible options:
- The primary focus is found in a pregnant woman.
- Pregnant patient diagnosed with lymphogranulomatosis.
In both cases, modern medicine tries to save the life of the mother and the unborn child. If the disease is detected for the first time, the examination and treatment of a woman becomes significantly more difficult, since the state of pregnancy excludes the possibility of radiation therapy. In the later stages, if the disease does not progress at an accelerated pace, doctors wait until the pregnancy is carried to term close to childbirth, and begin treatment immediately after. In this case, lactation must be artificially stopped .
Pregnancy developing during the disease is often complicated because the tumor affects the lymphatic system. In patients treated while expecting a child, the following occurs:
- dropsy –23%;
- anemia – 23%;
- pyelonephritis – in 20%;
- gestosis, varicose veins of the legs - less than 5%.
Etiology and pathogenesis of HL
The combination of features of the inflammatory response and features of malignant disease in Hodgkin lymphoma has led to debate about which features are neoplastic and which are infectious in origin.
It is believed that viral infection during adolescence may trigger the proliferation of precancerous lymphoid cells. In the USA, in 50% of cases of HL, integration of EBV into the genome of tumor cells was detected. However, since not all cases of HL are positive for EBV, it appears that it is only a cofactor for an as yet unknown causative factor.
The clinical picture in EBV-positive patients with HL does not differ from that in EBV-negative patients. This suggested that EBV causes genetic instability in predisposed patients.
A number of studies have shown that CB-III pathognomonic for Hodgkin lymphoma in 80% of cases originate from mature, slowly proliferating B cells of the germinal centers of lymph node follicles, in 20% they are derivatives of cytotoxic T lymphocytes.
The B cell origin of Hodgkin cells and KB-III cells was confirmed by clonal rearrangement of Ig genes with the absence of surface Ig expression. Somatic mutations with rearrangement of Ig genes are detected in B cells of germinal or post-germinal centers in the precursors of CB-III, although they can also occur at other stages of B-lymphocyte development.
It can be assumed that Hodgkin and KB-III cells, having lost the ability to express Ig and, having avoided apoptosis, gained the ability to uncontrolled proliferation. Since these cells with unwanted mutations do not undergo apoptosis, one can think about the dysfunction of genes that control apoptosis, namely the p53, BCL-2, MYC genes, or the blockade of the transmission of the “death signal” through the CD30 receptors on the surface of the CB-III.
Since CB-III in most cases belong to the B-lymphocyte lineage, they have the phenotype CD30+, often CD15+, CD25+, in most cases CD45-, CD20-. Additionally, these cells have dendritic cell markers. The reaction with anti-CD30 antibodies is typical for HL, but not specific, because it is positive with activated lymphoid cells and anaplastic large cell lymphoma cells.
Kinds
The form of lymphogranulomatosis determines the prognosis of the disease and the course of treatment chosen by the doctor. It can be established on the basis of a microscopic examination of histological preparations from tumor cells. The following types of disease are distinguished:
| Type of lymphogranulomatosis | Peculiarities | |
| Nodular type of lymphoid predominance | One of the aggressive lymphomas. It is more common in men over 35 years of age. Affects the cervical, axillary, and inguinal lymph nodes. The prognosis is extremely favorable. | |
| Classical Hodgkin's disease | Lymphoid predominance | In the affected organs, lymphocytes predominate over Sternberg cells. More common in teenagers. The prognosis is very favorable. |
| Sclerosing nodular (nodular sclerosis) | The most common form. Nodules of wide collagen fibers are located in the affected tissues. The prognosis is favorable. More common in young women. | |
| Mixed cell | The number of lymphocytes, eosinophils and Sternberg cells is approximately the same. Treatment includes a course of polychemotherapy. More common in men over 50 years of age. | |
| Lymphoid depletion | The rarest option. The number of lymphocytes is very small. The prognosis is the most unfavorable - the disease is difficult to treat. More common in older patients. | |
Leading clinics in Israel
Assuta
Israel, Tel Aviv
Ikhilov
Israel, Tel Aviv
Hadassah
Israel, Jerusalem
In medical practice, there are five types of Hodgkin lymphoma, four of which are included in the group called “classical lymphogranulomatosis”:
- Nodular category with lymphoid dominance. Of the total number of forms of this disease, this type of Hodgkin lymphoma accounts for 5% of patients. The predominant category consists of young men and those over forty years old. A distinctive feature of this type of Hodgkin lymphoma from classic lymphogranulomatosis is the histological picture and course of the disease. The affected area is the lymph nodes in the armpits, neck and, less commonly, the groin. With this form, the clinical course of the disease is weak, with periodic relapses, but negative development of the disease and unfavorable outcome are extremely rare (5%);
- Classic lymphogranulomatosis includes:
- Classic Hodgkin's lymphoma with an excess of lymphocytes (lymphoid predominance). With this form, a reduced number of Reed-Sternberg cells and an increased number of B-lymphocytes (cells that secrete antibodies and provide immunity) are observed. The number of annual diseases with the classic type of Hodgkin lymphoma is 95%. People with acute viral disease and human immunodeficiency virus are especially susceptible to the disease. The predominant location of lesions is in the lymph nodes: mesenteric, mediastinal, neck, axillary, groin, retroperitoneal space;
- Nodular Hodgkin's lymphoma (a variant of nodular sclerosis). This form occurs in 65% of people, with localization of the formation in the middle part of the chest (heart, aorta, bronchi), affecting the lymph nodes and thymus gland. As a result, 20% of patients suffer from damage to the spleen with further spread to the liver and bone marrow. This type of development of Hodgkin's lymphoma has a slow course, in which it affects: at stage I, groups of lymph nodes and lymphoid tissue, at stage II - several groups of nodes and one side of the diaphragm, at stage III - the lymphoid structure on both sides of the diaphragm, at stage IV - the liver and Bone marrow. Sclerosing nodular Hodgkin lymphoma is characterized by such symptoms as: increased sweating at night, chills and weight loss;
- Hodgkin's lymphoma of mixed cell type. Identification of this type of disease is carried out by diagnosing the cells that form the follicles. With a sluggish nature, lymphogranulomatosis can appear several years after diagnosis, however, it happens that lymphadenopathy has transient manifestations, which requires immediate treatment. Practice shows that the follicular form of Hodgkin's lymphoma, which by its nature has a low probability of developing into malignant neoplasia, has recently increasingly transformed into a heterogeneous abnormal cellular lymphoma of enormous size. Treatment, as a rule, leads to long-term remission and significantly increases the chances of recovery;
- Hodgkin's lymphoma with lymphocyte deficiency (lymphoid depletion) is the rarest form of the disease in question (5%) and is observed mainly in patients over the age of 50 years. The tumor consists predominantly of Rydsternberg cells with small streaks of lymphocytes.
Stages
Depending on the degree of spread of the pathology in the body, there are 4 stages:
- Stage 1 – the primary tumor is localized within 1 organ or 1 lymphoid area;
- Stage 2 – 2 or more organs or lymph nodes on one side of the diaphragm are diseased, the lungs are damaged;
- Stage 3 – the disease has affected areas on both sides of the diaphragm, the spleen is affected, changes in the stomach and intestines are recorded;
- Stage 4 - diseased organs are located diffusely throughout the body, the pathological process has moved from the lymphoid tissue to the surrounding tissue, the tumor affects the bone marrow, the digestive organs and bone tissue have metastasized.
Clinical picture
Typical for the initial stage of HL is a gradual enlargement of one or more lymph nodes, most often cervical, less often axillary.
Involvement of the inguinal or femoral lymph nodes at the onset of the disease is detected in less than 10% of cases. Lymph nodes have a dense elastic consistency, are not fused to the skin, and are painless. In 2-5% of cases, pain is observed in the affected lymph nodes after drinking alcohol; 10% of patients develop nonspecific skin itching. In the early stage of the disease, lymph nodes may spontaneously regress.
A fairly typical manifestation of the disease is enlargement of the mediastinal lymph nodes, which is often detected during a random chest x-ray, with or without shortness of breath.
Enlargement of the abdominal lymph nodes or spleen may manifest as abdominal discomfort, pain in the lumbar region, or be asymptomatic. The lungs can be involved in the process during dissemination of the disease or infiltratively when the tumor spreads “per contuitatem”.
Lung damage is both focal and infiltrative in nature, sometimes with decay and the formation of cavities; cB-III is extremely rarely found in sputum. The auscultatory picture is extremely poor. There are no pathognomonic signs of liver damage, and the diagnosis can only be reliably established by histological examination of a biopsy of liver tissue. Bone marrow involvement occurs in less than 5% of patients.
It can be assumed in the presence of a persistent tendency to anemia, thrombocytopenia and leukopenia, however, in the absence of these symptoms, bone marrow damage is determined only by trepanobiopsy; Sternal puncture is in most cases uninformative. Approximately 1/3 of patients have undulating fever with repeated waves at various intervals.
It is believed that the intoxication syndrome is caused by cytokines secreted mainly by KB-III: IL-1, which causes fever and profuse night sweats in HL; tumor necrosis factor (TNF)
-a and TNF-b, produced by cells of the same line, as well as increased activity of prostaglandin E2, can cause intoxication syndrome.
Deficiency of cellular immunity in Hodgkin lymphoma may result from the immunosuppressive effects of transforming growth factor (TGF) β
.
Damage to the central nervous system at the time of diagnosis is detected extremely rarely and is usually observed with progression in the later stages of the disease (ingrowth of the tumor from the lymph nodes along the myelin sheaths).
There are no characteristic changes in the peripheral blood. Some patients experience an increase in erythrocyte sedimentation rate (ESR)
, sometimes a tendency to neutrophilic leukocytosis or lymphocytopenia.
A biochemical study reveals dysglobulinemia, increased levels of fibrinogen, haptoglobin, ceruloplasmin, acute phase proteins, which are not specific, but reflect the activity of the process. Lactate dehydrogenase (LDH)
levels rarely increase.
Diagnostics
To diagnose lymphogranulomatosis, determine its type and stage, even an experienced doctor does not need an external examination of the patient, an analysis of his condition and medical history. A number of studies need to be carried out:
- General and biochemical blood test - in the tests of patients, the level of bilirubin, globulins, liver enzymes is increased, anemia and thrombocytopenia are detected.
- Lymph node biopsy - removal of cells from tumor tissue with a special needle.
- Trephine biopsy (taking a sample of bone marrow tissue) – if the last stages of the disease are suspected.
- Palpation of the cervical and supraclavicular lymph nodes - with lymphomas they are enlarged, although painless.
- X-ray – to detect pathology of the lymph nodes of the mediastinum (the space in the middle part of the sternum);
- magnetic resonance imaging or computed tomography of the neck, chest, abdomen.
Diagnosis of Hodgkin's disease
The diagnosis of Hodgkin lymphoma is established by laboratory and instrumental methods.
Laboratory diagnosis of lymphogranulomatosis
The purpose of diagnosis is to study blood parameters in the CBC, LBC, and ELISA.
Thus, a general analysis (using the Coombs test) allows one to identify symptoms of lymphoma such as:
- thrombocytopenia;
- anemia;
- eosinophilia;
- red blood cell adhesion;
- increase in ESR.
Biochemical analysis determines:
- liver tests (bilirubin, ALT, AST);
- the presence of proteins in the blood (alpha and gamma globulin, fibrinogen, C-reactive protein, etc.), which are traces of the inflammatory process;
- iron level;
- transferrin concentration.
Enzyme immunoassay detects ferritin, transferrin and erythropoietin receptors.
Tests are taken in the morning on an empty stomach.
Instrumental diagnostics
To make a diagnosis, the following instrumental methods are used:
- radiography;
- Ultrasound;
- CT (MRI);
- endoscopy (bronchi, esophagus, stomach, large intestine);
- laparoscopy (a minimally invasive method of examining the abdominal organs and lymph nodes;
- myelography;
- angiography;
- scintigraphy.
Puncture and histology of Hodgkin lymphoma
Bone marrow puncture and histology are considered the most accurate confirmatory methods for diagnosing lymphoma:
- During bone marrow puncture, red BM cells are collected from the bone canal.
- LN histology is carried out using one of three methods: puncture of the contents of the lymph node;
- aspiration biopsy with sampling of node tissue cells;
- incisional biopsy (complete removal of the node);
- biopsy during laparoscopy of lymph nodes.
Treatment of Hodgkin's lymphoma
At any stage of the disease, treatment is aimed at complete cure or achieving stable remission (in later stages). The prognosis for patients with lymphogranulomatosis is favorable in most cases. The following methods and their combinations are used for treatment:
- radiation therapy;
- chemotherapy;
- bone marrow transplant (in difficult cases).
Much attention is paid to preventing the development of relapses of the disease. To do this, it is necessary to undergo prescribed courses of maintenance therapy and adhere to the doctor’s recommendations. After recovery and during the remission stage, patients are prohibited from undergoing physical therapy, staying in places with high radiation levels, or working in hazardous industries.
Radiation therapy
Irradiation (radiation or radiotherapy) is a mandatory stage in the treatment of Hodgkin's disease, which involves exposing the affected tissue to ionizing radiation. In the early stages, it can be used independently, without a course of chemotherapy. Diseased lymph nodes are exposed to a dose of radiation of 40-45 Gy. The preventive dose of irradiation of the zones is 30-35 Gy. Organs and tissues not involved in treatment are protected with lead filters. The course of treatment lasts 2 – 3 weeks.
Nutrition
During and after treatment, patients are advised to adhere to a diet aimed at increasing immunity and maintaining the hematopoiesis process at the required level. The principles of nutrition for patients are as follows:
- ensure the consumption of foods rich in potassium but excluding sodium;
- reduce sugar intake, but do not eliminate carbohydrates completely, to avoid hypoglycemia;
- exclude fast food and other foods rich in trans and saturated fats;
- maintain sufficient drinking regime.
Forecast
A patient can be said to be cured if no signs of the disease are observed for 10 years or longer.
Today, lymphadenoma is treated successfully, and in 70-84% of cases it is possible to achieve complete remission, cancer relapses are observed only in 30-35%.
But it is worth noting that rather aggressive treatment methods, in the vast majority of cases, do not go away without leaving a trace. Of course, each person experiences therapy completely individually.
But what should you be wary of when dealing with radiation and chemotherapy?
- Male infertility. Doctors strongly advise young men who do not yet have offspring, but plan to have one in the future, to stock up on the genetic fund before therapy. With the development of current technologies, it is possible to place sperm in liquid nitrogen and use them for fertilization in the future, the shelf life allows.
- Infectious diseases. Since treatment involves irradiation of the lymph nodes, their possible removal and suppression of the immune system as a whole, cases of infection are not uncommon. Immunity boosting methods and antibacterial therapy are recommended for early signs of infection.
- Pneumonia, pulmonary fibrosis. With a long course of radiation therapy, inflammatory processes can develop in the lungs, affecting the pleural cavity. Liquid accumulates in the cavity. If inflammation is left untreated, normal lung tissue is replaced by fibrous tissue, and fibrosis is diagnosed. If complications develop, antibacterial and anti-inflammatory drugs are prescribed, as well as drugs that improve blood circulation in the lungs.
- Risk of return of malignant tumors. Relapse of the disease is much more difficult to treat. The calculation of new therapy and radiation is carried out taking into account the doses already administered.
Stages of disease development
When diagnosing a disease, its malignancy and stage of the disease are determined. The malignancy may be high, low or intermediate. As for the stages, there are four of them.
Stage I
At the initial, first stage of the disease, only a separate inflamed lymph node can be observed; general symptoms (weakness, poor health, hyperthermia) are not observed.
Stage II
At the second stage of a disease such as non-Hodgkin lymphoma, the tumors become multiple. General symptoms gradually begin to appear. If we are talking about the B-cell form, then at this stage the neoplasms begin to be divided into those that are subject to and those that are not subject to removal.
Stage III
At this stage of development of the disease, tumors often spread to the diaphragm, abdominal cavity, and chest. Tissues are affected, as well as all or almost all internal organs.
IV stage
The last and most severe stage of the disease. The prognosis in this case, unfortunately, is very disappointing. The disease affects not only organs, but also the bone marrow, reaching the central nervous system and bones. If the treatment was delayed so much that the lymphoma entered this stage, then there can be no talk of recovery.
Therapy with folk remedies
In addition to medications, you can take natural medicines. Some plants really have an excellent healing effect, for example, aloe. Here is one of the recipes that contains aloe juice: 500 gr. juice of this plant, 700 gr. honey and only 20 gr. mumiyo. Leave for three days.
Also a supportive therapy is a drink from a plant such as red root or periwinkle.
But you need to understand that taking herbs cannot be the main treatment for such a serious disease as lymphogranulomatosis. Treatment with folk remedies is secondary; The primary thing is radiation and drugs.
Consequences and complications
Chemotherapy drugs have a negative effect on the heart
HL is treatable, but provokes a number of complications, which in most cases is not associated with the disease itself, but with the consequences of chemotherapy and radiation, since these methods have an increased oncogenic potential. The more courses of therapy were carried out, the greater the risk of severe complications. Cancer of the breast, stomach, bladder, intestines, uterus and other organs causes 13-15% of deaths after therapy for HL.
Male infertility is a common consequence of therapy; before undergoing courses of treatment for HL, men are offered a sperm cryopreservation procedure. Cardiovascular disease occurs due to the cardiac toxicity of HL treatment. Complications of therapy also include diseases of the endocrine system, pulmonary pathologies, and severe infectious diseases.
Nutrition for Non-Hodgkin's Lymphomas
Nutrition for non-Hodgkin lymphoma should be as follows:
- adequate in energy consumption to prevent weight gain;
- as varied as possible: with vegetables and fruits, animal meat, poultry, fish and products derived from it, seafood and herbs.
- with minimal consumption of pickles and fermented foods, table (sea or table) salt, and smoked meats.
Meals should be tasty, frequent and in small doses. Each patient should be approached individually so as not to exclude hypernatremia (excess sodium salts). This retains fluid in the body and forms swelling. In this case, salt and smoked foods should be excluded so as not to increase salt K in the blood. If the patient cannot eat fresh food, his appetite spoils, then you can add a minimum amount of caviar, olives and other pickles to the menu, but in combination with drugs that remove sodium. It should be borne in mind that after chemotherapy for diarrhea and vomiting, sodium salts, on the contrary, are very necessary for the body.
Symptoms of lymphogranulomatosis
It is impossible to identify Hodgkin's disease (lymphogranulomatosis) without testing. But you need to be careful and look out for signs of illness.
The symptoms are as follows:
- For no particular reason (no infection or fever), the lymph nodes become enlarged. There is no pain on palpation.
- Shortness of breath due to the spread of the disease to the mediastinum. Enlarged lymph nodes in the chest area compress the lungs.
- Violent night sweats.
- Fast weight loss. The person “disappears” before our eyes.
- Abdominal pain may occur.
- Some patients (30–35%) complain of terrible itching of the skin.
- Weakness and temperature. Usually up to 380 C.
- When the spleen increases in size over time, the patient feels heaviness in the left hypochondrium.
Patients usually do not care how their disease is classified, but they are concerned about the survival rate. The question of whether lymphogranulomatosis is cancer or not is more of a medical nature. It is important for people not involved in medicine to know the main signs of lymphogranulomatosis and understand that the disease is actually serious and can be fatal.
Lymphogranulomatosis. Is it cancer or not?
Lymphogranulomatosis is undoubtedly a very serious disease. It is commonly referred to as lymphoid tissue cancer. But, in fact, is lymphogranulomatosis cancer or not? Epidemiologically and clinically, such lymphoma differs in some respects from real cancer.
What differences can you name?
- The prognosis for the treatment of Hodgkin's disease is favorable. If the pathology is found at stage 1, and there are no other concomitant diseases, then lymphoma is curable.
- There is no localized tumor characteristic of cancer.
- Cancer cells “eat” healthy cells. This is not the case with lymphogranulomatosis.
- Cancer begins with the transformation of connective tissue cells. In lymphoma, the development of tissue of a different nature (lymphoid tissue) is disrupted.
However, just like cancer, Hodgkin's disease leads to death if left untreated. Lymphoma spreads throughout the body and can lead to damage to other organs. At stages 3 and 4, the tumor is already large and all the lymph nodes in the body are affected: under the arms, in the chest, in the groin. And treatment also involves irradiation.
Classification of the disease
ICD 10 classifies the disease non-Hodgkin lymphoma as follows:
- Nodular or follicular
- Peripheral and cutaneous T-cell
- Diffuse non-Hodgkin's lymphoma (common)
- Unrefined and other forms
Classification by cellular composition
Most often in oncological practice, the classification adopted by the World Health Organization is used, which is based on cellular composition. According to this classification, lymphoma is divided into two types:
- Non-Hodgkin B – cell lymphoma. As the name implies, B lymphocytes, which are responsible for producing antibodies that are responsible for the humoral immune response, are affected.
- Burkitt's lymphoma most often affects men aged about 30 years. Cureability reaches 50%.
- MALT - marginal zone lymphoma. It affects the stomach, grows very slowly, but is difficult to cure.
- Small cell lymphocytic, slow growing, but not very sensitive to treatment.
- Primary mediastinal (mediastinal) or thymic large B cell lymphoma most often affects women 30-40 years old. Curable in 50% of cases.
- Splenic and nodal lymphomas grow slowly.
- Large cell diffuse B - cell lymphoma, characterized by rapid aggressive development of the disease, is typical for men over 60 years of age.
- Follicular lymphoma. Most often develops slowly, but can progress to a diffuse form with rapid growth.
- Primary CNS lymphoma is an AIDS-associated disease.
- Non-Hodgkin T - cell lymphoma. It is characterized by a malignant change and uncontrolled growth of T - lymphocytes, which are formed in the thymus and are responsible for the barrier (cellular) immunity of the mucous membranes and skin.
- T - cell lymphoblastic, develops from precursor cells, young people aged 30-40 years are most often affected, in 75% of cases men. The course is favorable only if the bone marrow is not damaged.
- Extranodal NHL, formed from killer T cells, can develop at any age and can have varying degrees of aggressiveness.
- Anaplastic large cell. It often occurs at a young age, but responds well to treatment.
- Cutaneous T-cell lymphoma (Sezary syndrome), another name is mycosis fungoides. Occurs in patients 50-60 years of age; growth rate and prognosis often depend on concomitant and background pathology.
- Angioimmunoblastic. It is characterized by a very aggressive course and unfavorable prognosis.
- T-cell lymphoma with enteropathy. It is highly aggressive and has a poor prognosis. Occurs in patients with gluten intolerance.
- T - cell non-Hodgkin's lymphoma, affecting the subcutaneous fat, another name is panniculitis-like. Poor prognosis due to poor sensitivity to chemotherapy.
Classification by disease aggressiveness
Also convenient and clinically significant for both oncologists and patients is the classification according to the aggressiveness of the process, as this determines the prognosis, treatment tactics and observation. Highlight:
- Indolent lymphoma - has low aggressiveness, develops slowly, sometimes without showing itself for years, the prognosis for life is usually favorable.
- The aggressive form of NHL is characterized by a high rate of growth and spread, the prognosis depends on the stage at which it was detected and sensitivity to chemotherapy.
- Intermediate form – grows gradually, constantly increasing the negative impact.
Risk group
The risk group includes the population over 50 years old and young people 16-20 years old. Adolescents under 18 years of age - this group makes up 5% of the total number of patients. And this is 150 people per year. These data are provided by statistics from German researchers. It is believed that the risk group also includes the following categories of the population:
- women who became pregnant after 30 years of age;
- people exposed to prolonged ultraviolet radiation;
- elderly people;
- having the problem of immunodeficiency.
However, after intensive therapy, people recover completely, or remain in remission for a long time if the lymphoma is detected at a late stage. The most attentive should be those who are at risk and may receive a diagnosis of lymphogranulomatosis; symptoms, blood tests and x-rays - all this needs to be constantly checked, you need to be alert and monitor your condition.
Prices
| Disease | Approximate price, $ |
| Prices for thyroid cancer screening | 3 850 — 5 740 |
| Prices for examination and treatment for testicular cancer | 3 730 — 39 940 |
| Prices for examinations for stomach cancer | 5 730 |
| Prices for diagnosing esophageal cancer | 14 380 — 18 120 |
| Prices for diagnosis and treatment of ovarian cancer | 5 270 — 5 570 |
| Prices for diagnosing gastrointestinal cancer | 4 700 — 6 200 |
| Prices for breast cancer diagnostics | 650 — 5 820 |
| Prices for diagnosis and treatment of myeloblastic leukemia | 9 600 — 173 000 |
| Prices for treatment of Vater's nipple cancer | 81 600 — 84 620 |
| Prices for treatment of colorectal cancer | 66 990 — 75 790 |
| Prices for treatment of pancreatic cancer | 53 890 — 72 590 |
| Prices for treatment of esophageal cancer | 61 010 — 81 010 |
| Prices for liver cancer treatment | 55 960 — 114 060 |
| Prices for treatment of gallbladder cancer | 7 920 — 26 820 |
| Prices for treatment of stomach cancer | 58 820 |
| Prices for diagnosis and treatment of myelodysplastic syndrome | 9 250 — 29 450 |
| Prices for leukemia treatment | 271 400 — 324 000 |
| Prices for thymoma treatment | 34 530 |
| Prices for lung cancer treatment | 35 600 — 39 700 |
| Prices for melanoma treatment | 32 620 — 57 620 |
| Prices for treatment of basal cell carcinoma | 7 700 — 8 800 |
| Prices for the treatment of malignant skin tumors | 4 420 — 5 420 |
| Prices for treatment of eye melanoma | 8 000 |
| Prices for craniotomy | 43 490 — 44 090 |
| Prices for thyroid cancer treatment | 64 020 — 72 770 |
| Prices for treatment of bone and soft tissue cancer | 61 340 — 72 590 |
| Prices for treatment of laryngeal cancer | 6 170 — 77 000 |
| Testicular cancer treatment prices | 15 410 |
| Bladder cancer treatment prices | 21 280 — 59 930 |
| Prices for cervical cancer treatment | 12 650 — 26 610 |
| Prices for treatment of uterine cancer | 27 550 — 29 110 |
| Prices for treatment of ovarian cancer | 32 140 — 34 340 |
| Prices for treatment of colon cancer | 45 330 |
| Prices for lymphoma treatment | 11 650 — 135 860 |
| Prices for kidney cancer treatment | 28 720 — 32 720 |
| Prices for breast reconstruction after cancer treatment | 41 130 — 59 740 |
| Prices for breast cancer treatment | 26 860 — 28 900 |
| Prices for prostate cancer treatment | 23 490 — 66 010 |
| Disease | Approximate price, $ |
| Prices for diagnosis and treatment of myeloblastic leukemia | 9 600 — 173 000 |
| Prices for diagnosis and treatment of myelodysplastic syndrome | 9 250 — 29 450 |
| Prices for leukemia treatment | 271 400 — 324 000 |
What causes the pathology: reasons
The disease or Hodgkin's lymphoma manifests itself in adults and children, while the classic tumor has an aggressive course. Until now, doctors have not been able to find out the true reasons why cancer of this localization is diagnosed. It is customary to identify several factors when the likelihood of progression of Hodgkin's disease increases:
- Diseases of an infectious nature. Oncology is diagnosed in patients with recent onset of mononucleosis provoked by infections.
- Reduced protective functions of the immune system. With weakened immunity, the risk of infection with the immunodeficiency virus increases. Patients who have recently undergone organ transplantation are at risk.
- A chronic type of autoimmune disease. If rheumatoid arthritis, celiac disease, systemic lupus erythematosus and the patient progress, Hodgkin's disease may manifest.
- Genetic factor.
- Negative effects of chemicals and other harmful substances. People who are constantly in contact with dyes, pesticides, benzenes and aromatic hydrocarbons are at risk.
- Professional activity. Patients who work in agriculture, wood processing, or seamstresses are at risk of acquiring Hodgkin lymphoma.
Complications
What complications can await the patient? Lymphoma is known to spread to the lymph nodes and disrupt the functioning of many organs. The function of the liver is disrupted, the spleen and thymus are significantly enlarged.
The brain is damaged. But what other diseases can accompany lymphoma?
- nephrotic syndrome;
- neurological complications;
- mediastinal jaundice;
- lymphatic edema;
- intestinal occlusion;
- infections;
- fungal infections due to weakened immunity.
This disease is especially dangerous for pregnant women. As for men, after completing a course of treatment for the disease, they are not recommended to have children for 1 year.
Prevention and prognosis
Regular visits to the doctor will help to detect the disease early
In recent decades, the number of patients with NHL has been steadily increasing, so it is important to follow preventive measures. Although the cause of the disease has not been thoroughly identified, it is recommended to avoid any chemically harmful substances or radiation exposure. Immunity should be maintained to protect the body from pathogenic microorganisms. The best way to achieve this is to maintain a healthy lifestyle, including optimal exercise, nutritious nutrition and spending time outdoors.
The prognosis of NHL depends on the type of lymphoma, severity and stage of development. In general, NHL is treatable, and patients can get rid of the pathology forever. There are a number of factors that worsen the prognosis:
- Advanced age;
- High lactate dehydrogenase level;
- Damage to more than 1 localization;
- III - IV stages of development;
- General poor condition.
Five-year recurrence-free survival is approximately 70% for marginal zone B-cell NHL; less than 30% for T-lymphoblastic, in children with a single tumor the chances are up to 90%.
Treatment
The choice of treatment for non-Hodgkin lymphoma depends on the stage of the disease, the degree of malignancy of the tumor, the age and general condition of the patient. It is important to distinguish between the treatment of low-grade and high-grade lymphomas.
Often different treatments are combined to achieve maximum results: these combinations are different for each lymphoma, so there is no general standard. Treatments for lymphoma include radiotherapy, radioimmunotherapy, chemotherapy, cytokine therapy, and monoclonal antibodies.
Radiation therapy
In world practice, radiation therapy is indicated in more than 70% of cancer cases
High-dose X-rays or other high-energy radiation are used to kill cancer cells and shrink tumors. Indolent stage I and II lymphomas are recommended to be treated with radiation therapy alone. For other forms, it is preferable to use a combination of chemotherapy and radiation therapy.
Chemotherapy
Medicines (usually cytostatic drugs) are used to kill cancer cells and reduce the size of malignant tumors. Cytostatics can be used in the form of tablets or solutions for intravenous and intramuscular administration.
Chemotherapy is a systemic therapy: drugs travel through the bloodstream throughout the body and destroy or suppress rapidly growing cells. However, healthy fast-growing tissues such as bone marrow, mucous membrane or hair cells are also damaged by chemotherapy, leading to various side effects such as anemia, hair loss, etc.
Cytokine therapy
Cytokine therapy stimulates the body's immune system to fight cancer. Cytokines are substances that mediate between protective cells and other leukocytes. These include, for example, various interleukins and interferons, the effect of which is to increase the readiness and targeted activation of certain types of cells.
Cytokine therapy should be distinguished from so-called “alternative” therapeutic methods, since the influence of cytokines has been scientifically proven in numerous studies.
Antibody therapy
Antibodies are used by the immune system to identify and eliminate foreign agents. On the outside of cancer cells are surface structures (antigens) to which antibodies bind. Therefore, artificially created antibodies are able to direct toxins or radioisotopes into malignant cells. Some artificial antibodies also have a direct damaging effect on malignant cells.
Rituximab, an antibody directed against the CD20 antigen, has shown promising results in the treatment of lymphomas. Antibody therapy is only possible if the degenerate cells also have the corresponding antigen on their surface. Antibody therapy is often given in combination with chemotherapy.
Radioimmunotherapy
Radioimmunotherapy is currently the subject of clinical trials. The cancerous tumor is treated with an antibody that recognizes a specific antigen. The antibody attaches after injection to tumor cells that carry the corresponding antigen. The cells are then selectively irradiated with a radioactive substance and thereby destroyed.
Prevention
Patients who suffer from this disease should undergo periodic check-ups after completing treatment. Aftercare is an important part of the entire treatment plan, and people should not hesitate to discuss it with their doctor. Regular and periodic monitoring can ensure that the doctor can prevent complications of the disease in a timely manner.
During follow-up visits, people who have non-Hodgkin's lymphoma should report any health problems.
Related Articles
Hodgkin's lymphoma: why does it occur and how dangerous is the disease?
Lymphoma in children: symptoms and treatment methods
Non-Hodgkin's lymphoma - what is it and what symptoms does it cause?
Lymphatic system cancer: symptoms and prognosis for life
Burkitt's lymphoma: what it is, symptoms, diagnosis, stages, treatment features and prognosis
Mediastinal lymphoma: what it is, causes, symptoms, treatment and prognosis of the disease
Classification of non-Hodgkin's lymphomas
The diagnosis of non-Hodgkin lymphoma implies that the patient has one of the many subtypes of this pathology. They all differ in their histological picture (changes in the structure of mutated tissues and cells) and specific symptoms. In this regard, approaches to their treatment should be different.
Only a correctly performed diagnosis can most accurately determine what type of non-Hodgkin lymphoma a patient has.
The NHL is classified according to the following criteria
:
- The rate of disease development.
Here we distinguish between
indolent lymphomas
(which have a very slow course and may not manifest themselves for years) and
aggressive ones
(with accelerated development and spread. Their impact on the body is very dramatic).
There is also an intermediate form of NHL,
in which the pathological influence increases gradually; - The site of origin of the cancer
.
Their classification includes 2 types. Nodal
- those that developed directly in the lymph nodes and
extranodal
- outside them. The latter include non-Hodgkin lymphomas of the spleen, lungs, stomach, etc.
Most often, there are several classes of lymphomas, which I would like to talk about separately.
B cell lymphoma
This type of pathology appears as a result of mutation of B lymphocytes. Their main purpose in the human body is to maintain immunity. Thanks to them, a so-called “library of dangers” is formed in our bodies. When a patient is diagnosed with B-cell lymphoma, this indicates that the cells that recognize foreign bacteria and viruses have mutated. To put it simply, the development of non-Hodgkin B-cell lymphoma leads to the body losing the ability to fight even the simplest diseases.
Diffuse
This aggressive type of NHL is the most common. It can occur at any age and has various symptoms. The tumor received this name because it causes a complete disruption of the internal structure of the lymph node. This leads to the rapid spread of mutated cells to all parts of the lymphatic system, that is, their peculiar “diffusion” occurs. In diffuse non-Hodgkin lymphomas, malignant neoplasms appear either at all points where the nodes are concentrated, or in any single area. The tumor that appears there grows rapidly and in a short time leads to the appearance of painful symptoms.
Large cell
Large cell non-Hodgkin lymphoma most often appears as a painless but rapidly growing tumor in the groin area, armpits, or neck. As it grows, it begins to be accompanied by symptoms such as significant weight loss, fever and night sweats. This type of tumor grows very quickly.
Follicular
The name of this type of non-Hodgkin lymphoma comes from the place of its formation - the follicles of the epidermis (hair follicles). For the most part, the disease is characterized by nodal localization, that is, it does not extend beyond the lymph nodes and does not grow into other organs. Its flow character is indolent. The development of follicular non-Hodgkin lymphoma is very slow and secretive. This is the biggest danger of this type of cancer. For the most part, it can be identified only in the final stages, when metastasis has occurred into various internal organs.
Small cell
This type of pathology develops when small cells of the lymphatic system mutate. Small cell lymphoma is characterized by a slow progression of malignancy. It has practically no specific symptoms and is most often detected in the last stages. For this reason, its complete cure can be difficult.
Brain lymphoma
This type of non-Hodgkin's lymphoma occurs mostly as a secondary lesion. It occurs as a large tumor formation in the head and is characterized by the following accompanying symptoms:
— Impaired sensitivity and coordination of movements;
- Severe headaches;
- Loss of memory and cognitive abilities.
A characteristic feature of brain lymphoma is the difficulty of diagnosing it due to the complexity of performing a biopsy. It is not always possible to quickly obtain the tumor material necessary for research.
Lymphoma of the lung
The symptoms of this type of disease in the first stages resemble a cold, accompanied by fever, cough with slight sputum, general weakness and sweating. The development of lung lymphoma can be suspected only by the worsening condition of the lymph nodes. They noticeably increase in size and become painful upon palpation. In the last stages of pulmonary lymphoma, patients experience hemoptysis. Metastasis also occurs to neighboring organs and the spinal cord. In the case when the pathology is diagnosed at the initial stage of the formation of the tumor process, almost all patients have a good chance of a complete recovery.
Stomach
Quite a rare type of pathology. It is characterized by the tumor growth of lymph cells occurring in the stomach. Damage to the digestive organ can be not only primary, but also secondary. Gastric lymphoma is characterized by the appearance of symptoms typical of diseases of the gastrointestinal tract: decreased appetite, nausea, turning into vomiting and abdominal pain. This makes it possible to identify this type of non-Hodgkin lymphoma in the early stages and, accordingly, carry out the most successful treatment.
Mediastinum
A very rare type. A feature that characterizes primary mediastinal lymphomas is the tendency to rapid growth and spread to the affected organ, located in this area, the esophagus, trachea, large bronchi, heart, etc. In this case, they are compressed, causing shortness of breath, cough, chest pain and dysphagia ( swallowing disorders). Non-Hodgkin's lymphoma of the mediastinum occurs mostly in young women. They suffer from this type of pathology 2 times more often than men.
T cell
This type of tumor is characterized by a mutation of T lymphocytes, which are responsible for destroying foreign pathogenic cells in the body. It manifests itself in generalized (general) enlargement of lymph nodes and skin lesions. Skin eczema appears as papules and plaques. At the same time, anemia and bone marrow damage are not typical for this form of pathology.
Chronic non-Hodgkin's lymphoma
A chronic course is characteristic of indolent (sluggish) lymphomas. The course of the pathology in this case is unpredictable. The remission stage is not stable. An exacerbation can begin at any moment. The chronic form of lymphoma is characterized by a low content of tumor cells in the blood and moderate lymphocytosis. Life expectancy in the absence of adequate treatment reaches several years until the disease becomes acute.