Bronchiectasis is a pathological condition that is irreversible and is characterized by dilation of the bronchi and bronchioles. The main cause of bronchiectasis is purulent-inflammatory damage to the bronchial wall. At the same time, local expansions occur in the bronchi, and the structure of the walls changes radically.
Causes and risk factors
The etiological factors of the disease have not been fully established. The most significant causes of the development of bronchiectasis are considered to be the following:
- genetically determined structural features of the bronchial tree (inferiority of the wall, underdevelopment of smooth muscle, connective tissue component of the bronchi, failure of the bronchopulmonary protection system);
- irreversible changes in the structure of the bronchial mucosa that arose against the background of infectious respiratory diseases suffered in childhood (both bacterial and viral);
- smoking, maternal alcohol abuse during pregnancy and viral diseases during this period;
- congenital anomalies of the structure of the bronchial tree (about 6% of cases).
Measures to prevent bronchiectactic disease include timely treatment of respiratory diseases, smoking cessation, and timely vaccinations.
Risk factors:
- unfavorable climatic conditions in the area of residence;
- unfavorable environmental situation;
- occupational hazards (industrial contact with toxic and aggressive volatile substances, dust, suspended matter, mists);
- smoking, alcohol abuse;
- chronic diseases of the bronchopulmonary zone;
- hard physical work.
Structural changes in the lungs during bronchiectactic disease
As a result of exposure to causative factors (in the presence of aggravating risk factors), structural and functional changes in the bronchial tree occur. Bronchial patency is impaired, which leads to a delay in adequate evacuation of bronchial secretions; Inflammatory changes develop in the bronchi, which, as they progress, can lead to degeneration of cartilaginous plates, smooth muscle tissue, and sclerosis of the bronchial wall. Impaired coughing, stagnation and infection of secretions in the dilated bronchi lead to the appearance of characteristic signs of the disease.
Main etiological factors
The reasons for the development of this disease are numerous. They vary depending on the form of bronchiectasis. The reason for the development of congenital bronchiectasis is a disruption of the development of the bronchi during the fetal development of the baby. Inferiority of the bronchi is associated with insufficient production of a special substance (alpha-1-antitrypsin).
The genetic defect causes subsequent deformation (expansion) of the bronchi and impaired secretion (sputum) excretion. Stagnation contributes to the addition of infection. Such changes in the bronchial tree cannot be treated and are irreversible. Congenital disorders may include the following:
- decreased local immunity;
- weakness of the walls of the bronchi;
- softening of the bronchi;
- connective tissue weakness;
- increased sputum production;
- changes in the composition and viscosity of bronchial secretions.
Abnormalities in lung development are caused by the following factors:
- heredity;
- smoking and alcohol consumption by the mother during pregnancy;
- toxic effects of drugs on the fetus;
- poor environmental conditions;
- infectious diseases (rubella, toxoplasmosis, cytomegalovirus infection);
- chronic somatic diseases.
The reasons for the formation of bronchiectasis in the lungs in children and adults lie in chronic pathology of the respiratory system. Respiratory diseases most often occur in childhood. The following causes of the secondary (acquired) form of bronchiectasis are distinguished:
- long-term pneumonia;
- pneumosclerosis;
- severe chronic bronchitis;
- pulmonary sarcoidosis;
- the presence of a tumor or cyst in the lungs or mediastinal organs;
- tuberculosis;
- chronic dust diseases (silicosis, silicosis, carboconiosis, metalloconiosis);
- rheumatism;
- systemic lupus erythematosus;
- the presence of foreign objects in the lower respiratory tract.
Risk factors for bronchial deformation include hypothermia, frequent respiratory infections in childhood, contact with tuberculosis patients, smoking, alcoholism, and occupational hazards. Bronchiectasis is a favorable factor for the development of infection. Violation of the drainage function of the bronchi contributes to the activation and accumulation of bacteria (cocci, Pseudomonas aeruginosa, Klebsiella, chlamydia, E. coli, Legionella).
Forms of the disease
Classification of bronchiectasis according to the form of bronchi dilatation:
- cylindrical;
- saccular;
- fusiform;
- mixed.
Types of bronchiectasis according to the form of bronchi dilatation
Bronchiectasis is understood as an irreversible, often segmental dilatation of the bronchi, caused by a change in tone or destruction of their walls due to inflammation, local disruption of trophic processes, sclerosis or hypoplasia.
According to the clinical course (severity), bronchiectasis can be:
- light form;
- moderate severity;
- severe form;
- complicated form.
Depending on the prevalence of the process:
- one-sided;
- double sided
Bronchiectasis occurs with alternating phases of exacerbation and remission.
Is it possible to cure the disease?
Bronchiectasis is a chronic progressive disease in which the quality of life of patients depends on the extent of lung damage, the degree of impairment of pulmonary function, the severity and frequency of exacerbations. This disease cannot be cured. But we are able to influence the rate at which the disease worsens. The rate of progression is largely determined by the nature of the chronic bronchial infection.
Thus, it is possible to slow down the progression of the disease and improve the patient’s quality of life with early diagnosis, identification and treatment of their cause, adequate treatment of chronic bronchial infections, prevention of exacerbations and regular medical supervision of the patient.
Are there surveillance programs for patients with bronchiectasis? Yes, they exist. Follow-up examinations with a doctor should be scheduled every 1 to 6 months, depending on the severity of the disease. Even if the patient’s condition is stable (in the remission phase), a general sputum analysis and bacteriological examination of sputum should be performed to assess the activity of inflammation in the bronchi. During the examination, the doctor should assess the severity of shortness of breath, the presence or absence of hemoptysis, general symptoms of inflammation (weakness, sweating, weight loss, temperature), listen to the lungs and, in case of severe impairment of pulmonary function, conduct a stress test (6-minute walk test).
Annual examination of a patient with bronchiectasis should include spirometry with a bronchodilator to assess the rate of decline in pulmonary function, a complete blood count with C-reactive protein (CRP) and immunoglobulin (Ig) A to assess the overall inflammatory response of the body.
At each visit to the doctor, it is advisable to measure saturation (oxygen saturation in the blood) using a pulse oximeter. If saturation decreases below 93%, it is recommended to perform a complete study of the gas composition of arterial blood to decide on the prescription of oxygen therapy.
For patients at high risk of disease progression, it is recommended to repeat CT scans of the lungs routinely once every 2 years. In addition, an X-ray of the lungs is performed annually, as well as if severe or life-threatening complications (pneumonia, pneumothorax) are suspected.
Symptoms
The main signs of bronchiectasis:
- cough with purulent, foul-smelling sputum;
- hemoptysis (approximately 1/3 of patients);
- shortness of breath (mainly during physical activity, worsens as the disease progresses);
- chest pain;
- increased body temperature, weakness, sweating, apathy, headache during an exacerbation.
Main symptoms of bronchiectactic disease
Sputum in patients with bronchiectasis has a putrid odor, comes out “full of mouth” (from 50 to 500 ml per day), and is released in greatest quantities in the morning after getting up or when taking a certain body position (hanging or with the head of the bed lowered). During the period of remission, the amount of sputum produced decreases significantly; In some patients, sputum is completely absent outside of exacerbations.
Hemoptysis more often bothers a person during an exacerbation of the disease or during intense physical activity. In rare cases, it may be the only manifestation of the disease (with so-called dry bronchiectasis).
Objective examination of patients:
- children's retardation in physical development, low body weight, muscle wasting;
- characteristic changes in fingers and nails (symptoms of drumsticks and watch glasses);
- cyanotic staining of the skin and visible mucous membranes;
- uneven participation of the chest in the act of breathing (lagging half on the affected side).
The onset of bronchiectasis in most cases occurs between the ages of 5 and 25 years; In women, the disease is registered less frequently than in men.
Treatment of bronchiectasis of the lungs: how will we treat it?
Let's start right away with treatment. So where does it always start? That's right, let's go to the doctor. And then there is the following:
- Treatment with antibiotics. The primary task is to stop the spread of infection. The medication regimen is always prescribed for each case separately. I'll explain why. If the lesion is severe, then antibiotics must be taken daily, even during periods of remission. If bronchiectasis is developed quite easily, it’s easier.
In this case, the method of administration can be different: in tablets, inhalers, aerosols, through intramuscular and intravenous injections. But the most effective way is to administer the antibiotic using bronchoscopy. More on this a little further.
- Complex medication use. In addition to antibiotics, anti-inflammatory drugs, bronchodilators, expectorants, immunostimulants, vitamin-mineral complexes, and herbs are prescribed (more about them below). If tests show the presence of an additional pathogen, for example a fungus, take antifungal drugs.
- Instrumental treatment. First, there is bronchoscopic drainage. A bronchoscope is inserted, with its help the sputum is removed, the bronchi are washed and irrigated with antibiotics. Secondly, this is electrophoresis. Further, during periods of remission, you need to undergo physiotherapy courses. Sometimes magnetic field treatment and microwave irradiation are prescribed.
- Surgery. In some cases, an operation is performed - a lobectomy (a part of the lung with bronchiectasis is removed). There are also contraindications, for example, damage to the bronchi on both sides, kidney failure, heart disease.
- Nutrition. Here we need a lot of calories (up to 3000 Kcal per day), protein and vitamins, and we reduce the content of fat, salt, and seasonings. And a lot of water, if everything is in order with the heart and kidneys. The diet for bronchiectasis is the same as for infectious diseases - table No. 13.
- Sanatorium treatment. Nothing heals the respiratory system better than sea, forest and mountain air. Most often, of course, salty, sea. Sanatoriums with mineral waters are very useful. For example, in the famous health resorts of the Caucasus, Abkhazia, Kislovodsk. Fortunately, now the sanatorium-resort network is well developed, and you can choose a place for any age, taste and budget.
- Exercise therapy. For bronchiectasis, breathing exercises and exercises in a lying position are necessary. I think this deserves a separate chapter.
Diagnostics
Diagnosis of bronchiectasis includes:
- taking anamnesis (prolonged cough with purulent sputum);
- objective research data;
- auscultation (during an exacerbation, hard breathing and various moist rales are heard over the lesion, decreasing or disappearing after vigorous coughing and expectoration of sputum);
- complete blood count (leukocytosis with a neutrophilic shift to the left, an increase in ESR);
- biochemical blood test [an increase in the content of sialic acids, fibrin, seromucoid, acute-phase proteins (nonspecific signs of the inflammatory process) is established];
- radiography of the lungs [reveals deformation and strengthening of the pulmonary pattern, a cellular pulmonary pattern in the area of the lower segments, thin-walled cyst-like clearings (cavities), sometimes with fluid, a decrease in volume (wrinkling) of the affected segments, increased transparency of healthy segments of the lung, “amputation” of the lung root, the presence indirect signs of bronchiectasis];
- bronchography with a contrast agent (the dilation of the bronchi of various shapes, their approach and the absence of filling of the branches located distal to bronchiectasis with a contrast agent are determined);
- bronchoscopy (the phenomena of purulent endobronchitis are established);
- serial angiopulmonography (anatomical changes in the vessels of the lungs and hemodynamic disorders in the pulmonary circulation are revealed);
- bronchial arteriography (for the presence of anastomoses between bronchial and pulmonary vessels);
- spirography (impaired external respiration is determined).
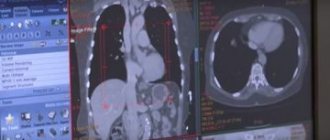
Visualization of bronchiectasis on CT
Treatment of bronchiectasis of the lungs: folk advice
Do not forget that folk remedies cannot be used instead of medicines. Only as an addition. Everyone knows chest infusions made from medicinal herbs. Probably everyone was given this when they coughed. But with purulent sputum, some herbs cannot be used, so we consult a doctor about everything.
Which recipes are considered the most effective:
- Garlic. The head of garlic should be chopped and mixed with a glass of milk. Boil the resulting mixture over low heat for 5 minutes, then filter and take a tablespoon three times a day before meals.
- Carrot. Namely its juice. Whether you make it yourself or buy it doesn’t matter. Mix a glass of juice with a glass of milk and add 2 tbsp. l. linden honey, set aside in a dark corner for 6 hours. Sometimes we come to interfere. When it brews, take 1 tbsp throughout the day. l. up to 6 times, preheated.
- Wine infusion. Take large aloe leaves, 4-5 pieces, scald with boiling water and knead. We try not to squeeze out the juice. Then pour the leaves with wine and let it brew for 4 days. After this, you can take the infusion according to Art. l. three times a day.
- Herbs. We need expectorant herbs that are taken for wet coughs. And this is licorice root, calendula, wild rosemary, marshmallow, coltsfoot, anise, sage.
Treatment
Complex therapy for bronchiectasis:
- passive and active sanitation of the bronchial tree, restoration of drainage of bronchial secretions;
- pharmacotherapy (antibacterial, mucolytic drugs, expectorants, bronchodilators, immunostimulants, immunomodulators);
- aerobic physical training, breathing exercises;
- Spa treatment.
Breathing exercises are indicated as part of the complex treatment of bronchiectactic disease.
If there is no effect from conservative therapy, surgical intervention is recommended.
With the development of complications of bronchiectactic disease (in particular, involvement of the cardiovascular system in the pathological process), the treatment prognosis significantly worsens.
Treatment of bronchiectasis
There are two types of treatment for bronchiectasis:
- Medication;
- Surgical.
The goal of drug treatment of bronchiectasis is to relieve exacerbations of pathological processes, prevent the development of complications and new formations. In this case, the patient is prescribed:
- High calorie diet;
- Mucolytic drugs, anabolic steroids, vitamins A and B, stimulants-modulators of the immune system, biogenic stimulants;
- Antibiotics that correspond to the sensitivity level of the detected flora;
- Physiotherapeutic procedures (including kinesitherapy and postural drainage).
Surgical intervention makes sense if conservative therapy does not produce positive results and the patient's condition worsens.
With the development of bronchiectasis of the lung, when the pathological process affects one or two of its lobes, resection of the lung is performed (it can be performed open or thoracoscopically). If bronchiectasis of the lung progresses and affects both lobes of the organ, lung transplantation is possible.
Prevention
In order to reduce the risk of developing bronchiectasis, it is necessary to:
- promptly treat respiratory diseases in children;
- carry out seasonal influenza vaccination;
- vaccinate against pneumococcal infection if the disease is present (to prevent exacerbation);
- avoid exposure to risk factors;
- stop smoking and alcohol abuse (they contribute to a significant deterioration of bronchopulmonary protection).
Video from YouTube on the topic of the article:
Why is bronchiectasis dangerous?
Complications from bronchiectasis are common. All of them are divided into pulmonary and extrapulmonary. Pulmonary complications include the following:
- lung abscess;
- bleeding;
- perifocal pneumonia;
- gangrene of the lung;
- broncho-obstructive syndrome;
- accumulation of air in the pleural cavity.
Extrapulmonary complications include brain abscess, anemia, sepsis, kidney damage (development of amyloidosis), liver and spleen damage, metabolic disorders, and cachexia. Dilatation of the bronchi in the absence of timely treatment leads to the following consequences:
- chronic respiratory failure;
- pneumosclerosis;
- damage to the kidneys and heart;
- septicemia;
- developmental delay of the child;
- exhaustion;
- formation of the pulmonary heart.
The most common complication is the development of respiratory failure. The reason is a violation of air movement and gas exchange in the alveoli. This leads to depletion of oxygen in the blood and disruption of the function of other organs. The presence of chronic respiratory failure is confirmed by a decrease in the partial pressure of oxygen in the blood.
Chronic respiratory failure is manifested by acrocyanosis, poor cold tolerance, periodic dizziness, weakness, shortness of breath on exertion or at rest. Long-term consequences of bronchiectasis include the development of pneumosclerosis. This is a condition in which connective tissue grows in the lungs. At the same time, the airiness of the organ decreases.
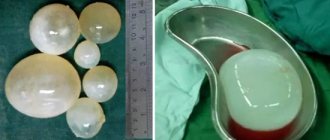
Treatment of saccular form
The course of the disease with the formation of saccular bronchiectasis is severe; in addition to drug treatment, additional methods of therapy are used.
Instrumental treatment methods are used.
These manipulations are used as maintenance therapy and are combined with taking the necessary medications.
Instrumental techniques include physiotherapeutic measures, for example, irradiation with microwave radiation, electrophoresis using calcium chloride, exposure to a high-frequency magnetic field.
Physiotherapeutic manipulations are carried out during the remission stage to prevent exacerbation of the pathology. Instrumental methods of therapy include endobronchial administration of drugs.
Using a bronchoscope, the specialist enters the bronchial tree and moves towards the expanded area. An antibacterial drug or medication is sprayed in the immediate vicinity of it to remove sputum and dilute it.
Stages of the disease
There are three degrees of development of bronchial expansion. The first stage has a benign course and is characterized by damage to the mucous membranes of the bronchi. The second degree is classified as a destructive process and represents damage to the entire thickness of the bronchial walls together with the peribronchial tissue. This stage of bronchiectasis is characterized by the following clinical situation: chronic, often exacerbating pneumonia, in which large volumes of purulent-sputum masses are released. In the third stage of lung damage, the clinical picture looks even more depressing: abscess pneumonia, accompanied by the constant release of foul-smelling purulent-sputum masses and periodic hemoptysis.
Consequences of the disease
Bronchiectasis with an unfavorable course can lead to a number of pathological conditions.
Complications of bronchiectasis include:
- Respiratory failure is a pathology that occurs in most patients with bronchiectasis, manifested by shortness of breath, cyanosis of the skin, decreased tolerance to physical activity, and changes in blood gas composition;
- Cor pulmonale is a complication of any bronchopulmonary pathology that has lasted for decades, resulting in right ventricular heart failure, congestion in the systemic circulation, edema, and liver enlargement;
- Kidney amyloidosis is also a complication of many chronic processes in the lungs; it occurs due to an imbalance of proteins in the body, manifested by the deposition of protein masses in the kidneys and the gradual development of chronic renal failure;
- Pulmonary hemorrhage - can occur in severe cases of even a short-term bronchiectasis; this complication appears due to persistent cough, as a result of which small vessels of the lungs rupture;
- Pneumosclerosis is a complication characterized by the formation of foci of connective tissue proliferation in the lung tissue, which aggravates respiratory failure.
All of these pathological conditions are potentially life-threatening for the patient.
What is this
Bronchiectasis is a rare phenomenon, but cases of the formation of the disease are recorded, and it has a severe course. This pathology occurs as a consequence of bronchial deformation - a certain area of the bronchus undergoes thickening, which is formed as a result of damage to the bronchial wall.
This process leads to the fact that the structure and function of the bronchi becomes different. In this thickened and modified zone of the bronchus, purulent deposits are observed.
Bronchiectasis is localized mainly in the lower region of the lungs. There are 2 positions explaining the nature of the pathology.
The first position is based on the idea that this is a primary lesion. Bronchiectasis occurs without a previous disease, and bronchiectasis is called an independent nosological form.
The hypothesis is not yet considered as real; such a mechanism for the development of the disease has been little studied.
The second statement describes the fundamental principle of the occurrence of bronchiectasis. Bronchiectasis is considered as a secondary substrate that occurs along with another disease or is a complication of some disease.
Secondary bronchiectasis is a companion to diseases - tuberculosis, lung abscess and chronic pneumonia.
Classification and symptoms of the disease in a child
Depending on the causes of occurrence, course and severity of bronchiectasis, doctors distinguish several of its classifications. Their determination is important when diagnosing a patient and selecting methods of treatment.
If we consider bronchiectasis through the prism of their root causes, then they are:
- conditionally primary (arise as a result of a genetic predisposition of the respiratory organs to defective functioning);
- conditionally secondary (pathology develops as a result of complications of continuous respiratory diseases).
Did you know? In healthy people, there is always more air in the right lung than in the left.
According to the shape of the modifications of the bronchi, saccular, fusiform, cylindrical, and mixed bronchiectasis are distinguished. And depending on the course, there are several forms of bronchiectasis:
- light . It is characterized by a one-time exacerbation per year and excellent health of the patient during the absence of manifestations of the disease;
- medium- heavy There can be up to 5 exacerbations per year, with moderate dysfunction of the respiratory organs and decreased performance;
- heavy . It is expressed by fairly frequent periodic exacerbations and short-term relief, as well as lack of performance and very poor functioning of the respiratory system;
- complicated _ This form of the disease is characterized by all the severe symptoms combined with associated complications.
Find out how to treat in children: cystitis, dysarthria, enterovirus infection, intestinal infection, mononucleosis, stomatitis, scoliosis, hip dysplasia, atopic dermatitis, streptoderma, obstructive bronchitis, adenoids, colic and whooping cough.
Bronchiectasis can be unmistakably recognized by a cough accompanied by purulent sputum with an unpleasant odor. During the remission period their number is minimal, and during an exacerbation - abundantly. A characteristic feature of the discharge is that it leaves to a greater extent in the morning and only when the body is located on the side opposite to the deformed areas of the bronchi.
This may include general weakness, malaise, shortness of breath, loss of appetite, poor performance, fever, headache, bleeding when coughing and pain in the sternum.
If the disease torments a child for a long time, his fingers may become very wide and his nails may become convex. This occurs as a result of bone growth and oxygen starvation of the body. But another danger of the disease is that in the initial stages of development it can be asymptomatic.
Did you know? Every day, about 10 thousand liters of air pass through the lungs of a healthy person, and the total weight of the blood driven is 8 tons.
Sputum examination.
- general analysis of sputum: purulent sputum, 2 or 3 layers when settling, multineutrophils, elastic fibers, red blood cells may be present
— culture of sputum or BALF for flora and sensitivity to antibiotics
Read also: How much alcohol is in pina colada
4. X-ray examination of the chest in two projections.
Characterized by a decrease in the volume of the affected part of the lung, a shift of the mediastinum towards the affected side, a high position of the diaphragm, strengthening, deformation, cellularity of the pulmonary pattern, and sometimes intense darkening of a sharply reduced lobe.
5.
X-ray tomography
,
computed tomography
- more informative compared to radiography
6. Bronchography –
cylindrical or saccular expansions of the bronchi of the IV-VI order, their approach, deformation, lack of contrast distal to the branches located.
7. Fiberoptic bronchoscopy
(possibly with a biopsy) - signs of purulent bronchitis, clarification of the source of bleeding
Complications
Bronchiectasis develops in the lungs, but there are complications:
- pulmonary;
- extrapulmonary.
The first group of complications include:
- bleeding in the lungs;
- abscess pneumonia (lungs filled with pus);
- organ gangrene;
- disruption of the passage of air through the bronchi. There is constant shortness of breath, a feeling of lack of air;
- pneumothorax.
The second category of complications included:
- entry of toxic bacteria into the blood (sepsis);
- amyloidosis, in which protein accumulates in internal organs, leading to disruption of their functioning.
Bronchiectasis - treatment
Bronchiectasis can be treated with medications, surgery, or endoscopic techniques.
For reference. As a rule, all of the above methods are used in combination with each other. In addition, during the remission stage, physiotherapeutic treatment can be used to prevent subsequent exacerbation.
Conservative therapy
Conservative methods of treatment are called medicinal methods. They are aimed at relieving the main symptoms of the disease and eliminating the causative agent of the exacerbation. They start with etiotropic therapy. A broad-spectrum antibiotic is prescribed.
Additionally, mucolytics are prescribed that allow better removal of sputum, for example, ambroxol or acetylcysteine.
High fever can be treated with non-steroidal anti-inflammatory drugs, such as ibuprofen. In case of severe cough with streaks of blood in the sputum, antitussives, for example, Ascoril, are recommended. To combat shortness of breath, inhaled beta-agonists are prescribed.
Surgery
For reference. It is advisable to resort to surgical intervention in cases where bronchiectasis is isolated and can be removed without consequences for the body. In this case, the main indication for surgery is frequent exacerbations of the disease.
Removal of single enlarged areas can lead to complete cure if no new bronchiectasis appears in the future. However, the operation is quite difficult and traumatic, so this type of treatment is rarely used.
Endoscopic treatment
Endoscopic therapy is a therapy that is performed during bronchoscopy. In this case, using special devices, you can aspirate pus from the bronchiectasis cavity, treat it with an antiseptic, or administer other medications.
This method is also limited in application because it causes pain in the patient.
Characteristic symptom
Such a symptom as “Hippocrates’ fingers” appears mainly in people over 40 years of age. As respiratory failure progresses, the fingers begin to expand from the base to the top of the phalanges. They may take on the appearance of drumsticks. This hand deformation is irreversible.
The nature of the disease and the symptoms that appear in the overall picture can help in suggesting the presence of bronchiectasis, but there is still a need for diagnostics to establish an accurate diagnosis.
What about prevention?
Here's what you need to do:
- eliminate smoking;
- do not inhale dust, either at home or at work;
- treat upper respiratory tract infections in a timely manner;
- Healthy food;
- harden the body.
Stop! Hardening does not mean hypothermia.
Pouring with ice water is not for you, it is better to choose gentle methods, move more and walk. It is necessary to observe a sleep and rest schedule, and be sure to do gymnastics, both breathing and general strengthening, in the fresh air.
I’ll say a few words about nutrition
To recover, you will need a lot of protein and vitamins, iron and other microelements. There is no need to eat whole mountains of meat, fish and cottage cheese. You need to consume food correctly and in the right quantities, in small portions and at least five times a day, for better digestibility.
Food should be light and tasty, because the psychological factor is no less important than any other.
Forecast
Competent, timely treatment helps to achieve stable remission and stop the progression of the disease. In some cases, complete recovery is achieved. In the absence of treatment in moderate, severe and complicated forms of pathology, the prognosis is unfavorable. About a quarter of patients die within 5-10 years. In half of the patients who did not undergo surgery, the disease progresses.
Mortality after surgery is low. But an absolutely positive result is rare. Slightly more than half of patients forget about the disease for a long time. 12% fail to improve. The rest periodically face relapses.
Antibiotics
Antibiotics are prescribed according to the microflora that is sensitive to them. Sensitivity is determined using microbiological studies of sputum.
Because an exacerbation can be triggered not by one microorganism, but by a whole association of microbes that are resistant to most antibacterial drugs, therefore broad-spectrum antibiotics are prescribed: penicillins, cephalosporins, fluoroquinolones and nitrofurans.
There are 4 groups of people according to Wilson. Using this classification, you can determine the amount of necessary therapy and the choice of antibiotic:
- Previously healthy individuals with post-viral bronchitis. They are characterized by the production of viscous sputum, which leads to poor penetration of antibacterial drugs into the bronchial mucosa. Such patients need plenty of fluids, expectorants, and herbal infusions that have a bactericidal effect. If the amount of therapy does not help, amoxicillin, erythromycin, and tetracycline are recommended.
- Patients with obstructive and non-obstructive chronic bronchitis. It is necessary to follow the same instructions as for the first group.
- Patients with chronic bronchitis and the addition of severe somatic pathologies and a high risk of developing a secondary infection. This group requires treatment with the following groups of antibiotics: cephalosporins, fluoroquinolones and combination antibiotics.
- Patients with chronic bronchitis and associated bronchiectasis, secreting purulent-hemorrhagic exudate (sputum). It is necessary to follow the therapy recommended to the third group, and also include macrolides in the treatment.
Important! When prescribing antibacterial therapy, it is necessary to take into account individual drug tolerance. Many people are allergic to the penicillin group.
Antibiotics can be prescribed orally, intravenously or intramuscularly. This depends on the severity of the disease and the general condition of the patient.
Important! In case of severe and long-term COPD (chronic obstructive pulmonary disease), antibacterial drugs that have chemotherapeutic activity against the causative agents of chronic bronchitis may be prescribed.
Penicillins
- The group of penicillins includes benzylpenicillin sodium and potassium salts. Available in powder form. Prescribe from 250 thousand to 1 million action units, dissolving the powder in lidocaine or sodium chloride NaCl 0.9%. Administer intramuscularly 1-2 times a day. Penicillins can provoke skin itching, rashes of various types and angioedema of angioedema in case of hypersensitivity to the drug. Cost – from 6 rubles for 1 bottle.
- Combined drug Augmentin , consisting of amoxicillin and clavulonic acid. Available in tablets, powder form and suspension. Prescribe 1000 mg (1 tablet) 2-3 times a day. Cost – from 400 rubles.
Benzylpenicillin sodium salt
Augmentin
Cephalosporins
From this group, Ceftriaxone is used. Available in the form of powders for intravenous and intramuscular administration. Contraindicated during pregnancy, bleeding, and pathology of the large intestine. Price – from 35 rubles for 1 bottle.
Ceftriaxone
Fluoroquinolones
Ciprofloxacin is active against common pathogens in bronchitis (mycoplasma, staphylococci and streptococci). Prescribe 1 tablet 2 times a day.
Side effects may develop in the form of abdominal pain, seizures, decreased hearing and vision. It is not recommended to use drugs for fungal infections and dysfunctions of the urinary system and liver.
Cost – from 300 rubles.
Ciprofloxacin
Nitrofurans
They have bactericidal and antiseptic effects. Representative – Furazolidone. Take 1 tablet 0.1 g every 6 hours. Cost – from 20 rubles.
Furazolidone
Drugs for dilation of bronchi
M-anticholinergics
M-anticholinergics
– drugs that block M-receptors, resulting in dilation of the bronchi. These drugs are contraindicated during pregnancy, rhythm and conduction disorders, and glaucoma.
This group includes Atrovent. Available in the form of an aerosol, you need to take 1-2 breaths 3 times a day. Price – from 223 rubles.
Atrovent
B2-adrenergic receptor stimulants
B2-adrenergic receptor stimulants
– drugs that enhance the functioning of B2 adrenergic receptors in the smooth muscles of the bronchi and lead to the expansion of their lumen.
These include:
- Short-acting drug – Salbutamol. It is recommended to take 1-2 puffs 4 times a day. Price – from 60 rubles.
- Long-acting drug – Formoterol. Prescribe 1-2 breaths 2 times a day, morning and evening. Price – from 880 rubles.
Formoterol
Salbutamol
Methylxanthines
Methylxanthines also have a bronchodilator effect, but they are prescribed only for severe cases due to the large number of side effects. They quickly eliminate bronchial obstruction, restoring respiratory function.
There are:
- Short-acting methylxanthines include Euphyllin. Prescribe 10 ml intravenously, diluting it with 300 ml saline. solution (NaCl). Cost – from 12 rubles.
- Long-acting methylxanthines include Theotard. They are prescribed 0.3 g 1 time per day. The cost of extended-release theophyllines is from 200 rubles.
Eufilin
Theotard
The following side effects may occur when taking methylxanthines:
- hypotension,
- allergic itching,
- diarrhea,
- irritability,
- tremor.
Anti-wet cough medications (expectorants)
Restoring and improving the functioning of mucociliary transport (ciliated epithelium) is very important, because this leads to the subsidence of the exacerbation.
Expectorants are divided into several groups:
- Medicines that stimulate expectoration : Mucaltin. Available in tablet form, it consists of herbal mixture and polysaccharides. Prescribed 3 tablets 3-6 times a day. The drug must be stored in the refrigerator. Cost – from 15 rubles.
- Eucalyptus tincture – 15 drops 2-5 times a day.
Eucalyptus tincture
Mukaltin
- Mucolytic drugs - thin (reduce viscosity) sputum: Acetylcysteine (ACC). It is used in tablet form orally, 200 mg 3 times a day. Can also be used for inhalation, because Available in solution. Contraindicated for gastric ulcers in the acute phase. Cost – from 116 rubles.
ACC
- Mucoregulators - reduce the viscosity of sputum, increase its excretion, improve the regeneration (restoration) of ciliated epithelial cells and the synthesis of surfactant: Bromhexine. Available in tablet form, injection solutions and syrup. Used orally, 1-2 tablets 3 times a day, or intravenously, 2 ampoules 2-3 times a day. Price – from 17 rubles.
- Ambroxol. Available in tablets and solutions. In the first 5 days you need to take 30 mg (1 tablet) three times a day. Then the dose is reduced by 2 times. 2-3 ampoules are administered intravenously or subcutaneously twice a day. Price – from 14 rubles .
Ambroxol
Bromhexine
Antiviral drugs for bronchitis
Antiviral drugs are rarely used when bronchitis is caused by viruses. Most often, Anaferon and Arbidol are used to treat such bronchitis. The cost of drugs varies from 250 to 1000 rubles.
Anaferon
Arbidol
Cause of congenital and acquired bronchiectasis
The main cause of acquired bronchiectasis is complicated diseases, such as tuberculosis or pneumonia.
Along with the described mechanism of formation of acquired bronchiectasis, there are factors that also help the development of this type of pathology:
- Panbronchiolitis of diffuse type;
- Inhalation injuries;
- Immunodeficiency;
- Congenital disorders of the respiratory system;
- Genetically transmitted diseases.
Congenital bronchiectasis occurs as a result of damage to the respiratory system during the period of intrauterine fetal formation.
Such underdevelopment of the respiratory system usually leads to the fact that the child has no alveoli on the outer bronchial branches.
As a result, the air tubes in the affected area thicken. The presented defect may affect only a certain part, a lobe of the lung, or the entire lung. If such a picture covers both lungs at once, the fetus is not viable.
The reasons why this pathology may develop in a pregnant child is the mother’s improper behavior during and before pregnancy. Aspects like smoking, consumption of drugs, large amounts of alcoholic beverages in significant cases lead to bronchiectasis.
Treatment options
Treatment of bronchiectasis is complex and complex. The methods used depend on the severity of the bronchial lesion.
Conservative treatment
The main method in the treatment of patients with minor manifestations of the disease. It is also used in the treatment of patients with widespread foci of inflammation in the presence of contraindications to surgery. A mandatory step in preparation for bronchoscopy and surgery.
Medicines, medical procedures and physical therapy help maintain stable remission. In children, complete recovery is possible. In complex cases, conservative treatment helps prevent complications and stop the progression of the pathology.
Clinical recommendations include taking antibiotics. Their choice depends on the pathogen and its sensitivity to drugs. Bronchodilators have a dilating effect and promote mucus discharge. Mucoregulators thin mucus and facilitate its drainage. The drugs are used in the form of tablets and injections. The use of an inhalation nebulizer helps the drugs penetrate as close as possible to the source of infection.
Additionally, xenobiotics are prescribed to restore intestinal microflora. Antifungal drugs are used for preventive purposes. Immunity is increased with the help of immunomodulators and vitamins. If it is proven that the cause of the pathology is a congenital deficiency of alpha-1-antitrypsin, replacement therapy is carried out
In addition to drug treatment, sanitation measures are necessary. Using a bronchoscope, antibiotics, antiseptics and drugs to improve sputum discharge are injected into the bronchi. Procedures are carried out every 2-3 days until suppuration decreases. If this method is poorly tolerated, endotracheal administration of drugs is used.
Lavage is used for washing. The procedure allows you to cleanse the lungs and remove mucus. Sanitation of the upper respiratory tract is necessary mainly for children. It is performed by an otolaryngologist. Infusion drip solutions have a diuretic effect and improve microcirculation. They are necessary to reduce intoxication.
Physiotherapy plays an important role in treatment. Postural drainage and vibration massage of the chest help get rid of stagnation of pus and mucus in the bronchial tree. Oxygen therapy is indicated for respiratory disorders. Medicinal electrophoresis, therapeutic exercises and breathing exercises are also useful. All these procedures restore the natural drainage function and normalize blood circulation in the lungs.
Surgical intervention
The optimal age for surgery is 7-14 years. In an earlier period, it is difficult to identify the affected area. In older patients, the result may not be effective. In mild forms, the decision to perform an intervention is made with caution based on an assessment of the dynamics of the condition after conservative treatment. In difficult cases, surgery is prescribed provided that after the manipulations the respiratory function is not impaired.
With unilateral ectasis, it is possible to remove all affected tissue while preserving healthy tissue. In advanced cases, the lung is completely removed. Bilateral asymmetrical lesions provide the opportunity for partial tissue removal on the more affected parts. This can significantly improve the patient’s condition and stop the progression of the disease. For symmetrical changes, resection on both sides is indicated. But only if there is enough healthy tissue in the bronchial tree. The operation is carried out in two stages with a break of six months or a year.
For patients with complications that have spread to the heart, obstructive bronchitis and severe respiratory failure, surgery is contraindicated. Changes in the kidneys and liver are most often reversible even at the stage of conservative treatment, so they do not interfere with resection. The older the patient, the greater the likelihood of extensive changes and the less chance of surgical removal of bronchiectasis.
Contraindications also include suspicion of congenital weakness of the bronchial wall. This is indicated by an inflammatory lung disease suffered in early childhood. During surgery, the risk of developing new bronchiectasis and reducing respiratory function increases due to a decrease in the area of healthy tissue.
Regardless of contraindications, surgery is performed for life-threatening conditions. These include pulmonary hemorrhage, gangrene and pneumothorax.
A story about a tree that grows upside down
We have such a phenomenon in our bodies.
The trunk of our tree is the trachea. Two massive branches depart from it - the main bronchi, which are then divided into many small branches. At their ends alveoli grow - small bubbles through which oxygen enters the blood. Bronchiectasis is a deformation of the bronchi.
They stretch, their walls become thinner, and cannot work normally. They develop a chronic inflammatory process, which results in the accumulation of pus. Since the organ is sick, various pulmonary infections are added to the main ailment.
You should be alarmed if you have the following symptoms:
- persistent cough;
- separation of a fair amount of purulent sputum, especially in the morning;
- hemoptysis, and in the worst case, pulmonary hemorrhage.
What causes bronchiectasis?
There are two types of causes of bronchiectasis:
- Primary bronchiectasis. They arise as a result of congenital pathologies. Due to genetic inferiority, the bronchial tree is not formed correctly, and the bronchial tissues become deformed and expand. Such cavities subsequently become infected, which causes chronic inflammation and suppuration.
- Secondary bronchiectasis. The appearance of this type of bronchiectasis is promoted by various infectious diseases of the respiratory system, such as bronchitis and pneumonia. Due to the disease, the walls of the bronchi lose their elasticity and atrophy. Frequent coughing in chronic bronchitis also contributes to this process.
Diagnosis of the disease
Bronchiectasis does not have pathognomonic symptoms that could be used to identify this particular disease. To make a diagnosis, a number of additional studies are necessary.
These include:
- Physical examination. It is carried out by percussion, palpation and auscultation. As a rule, palpation and percussion do not give any results. Exceptions are secondary bronchiectasis, in which the underlying disease is detected. On auscultation, moist rales are heard in the lungs, the localization of which corresponds to the localization of bronchiectasis.
- X-ray of the chest organs. It is also not the most reliable way to make a diagnosis. Bronchiectasis itself is not visible on x-rays. However, it is possible to identify the cause of the pathology if it is another lung disease. Complications of bronchiectasis may also be visible on x-rays.
- Bronchography. This is the main method of diagnosis. Bronchography is an X-ray examination with the introduction of contrast into the bronchi. At the same time, the structure of the bronchi, areas of bronchiectasis and their shapes are clearly visible.
- Bronchoscopy. This method allows you to see the bronchi from the inside. In this case, you can evaluate changes in the mucous membrane and look at the contents of the bronchi. Sometimes this method is used not only for diagnostic purposes, but also for therapeutic purposes.
- Spirometry. This test cannot make a diagnosis, but it can reveal the degree of respiratory failure. This is important for determining patient treatment tactics.
Causes that contribute to the development of bronchiectasis and its types
The impetus for the development of bronchiectasis is many factors; it is difficult to single out the main one. But there are still three groups of reasons:
1. Genetic factor.
Genetic factors in the development of bronchiectasis include various defects that exist from birth and contribute to the formation of bronchiectasis in the lungs.
2. Abnormal development of the lungs.
Abnormal lung development can occur when the lungs are not formed correctly in the womb. Due to the poor lifestyle of a pregnant woman, as well as as a result of infectious diseases she has suffered, a child may be born with bronchiectasis in the lungs.
3. Past respiratory tract infections.
Since children are very prone to diseases of the respiratory system, we can assume the development of bronchiectasis due to infection. This outcome is likely if there is a genetic factor or abnormal lung development in the child.
IMPORTANT! Bronchiectasis can occur in different forms. Having determined the nature, symptoms and features of this disease, the doctor will be able to make an accurate diagnosis and prescribe adequate and effective treatment.
The type and degree of bronchiectasis of the lungs can be classified according to the following indicators:
- bronchial deformation;
- phase of bronchiectasis;
- areas that are affected by inflammation;
- severity of bronchiectasis;
- the cause of bronchiectasis in the lungs.
The main criterion is the nature of the deformation of the bronchi, because it is used to describe the pathological process. The type of deformation is determined using bronchography, the results show the following forms of expansion:
- cylindrical: the expansion of the lumen of the bronchi is uniform and located over a long section;
- clearly shaped: such bonchiectasis look like beads or rosaries, located sequentially along one bronchus;
- saccular: expansion of the bronchus is observed on one side in the form of a ball or oval;
- fusiform: bronchiectasis has the appearance of a gradually narrowing expansion;
- mixed: one patient has several of the above forms.
Diagnosis of bronchiectasis
Laboratory diagnostics
A general blood test reveals leukocytosis, increased ESR, and sometimes anemia.
The sputum has a three-layer character, and its bacteriological examination reveals symptoms such as various microflora (Haemophilus influenzae, Streptococcus pneumoniae, Staphylococcus aureus, anaerobes, Mycobacterium tuberculosis, fungi). When examining blood serum globulins, a significant decrease in the sc-fraction is detected, which allows one to suspect alpha-antitrypsin deficiency, especially in patients with emphysema. It is advisable to determine the content of electrolytes in sweat fluid, since chloride concentrations of more than 60 mEq/L in children and more than 80 mEq/L in adults are pathognomonic for cystic fibrosis. In order to identify primary ciliary dyskinesia, a biopsy of the nasal mucosa is performed for ultrastructural studies of the cilia apparatus. Differential diagnosis
Differential diagnosis of symptoms of bronchiectasis in most cases is not difficult. Sometimes the problem arises in cases of severe deformation of the bronchi in COPD. However, the introduction of RCT and, if necessary, carefully performed bronchograms make it possible to confirm or exclude the presence of bronchiectasis. Atelectasis racemes differ from small bronchial cysts by good contrast.
www.medmoon.ru
Bronchiectasis is an irreversible dilation of a section of the bronchus caused by damage to the bronchial wall.
Bronchiectasis can develop as a result of conditions that indirectly or directly lead to damage to the bronchial wall, impairing its stability. Bronchiectasis can occur either in any particular area or throughout the bronchi.
As a rule, their development is observed in bronchi that are of medium size, however, quite often, damage to small bronchi located below is observed.
There are several types of bronchiectasis that affect large bronchi. Their occurrence is observed in allergic bronchopulmonary aspergillosis, the occurrence of which is associated with the body’s immune response to a fungal infection.
The bronchial wall has several layers, which in different parts of the respiratory tract have different thickness and structure. The bronchial mucosa and the submucosa that follows it have cells that help protect the respiratory tract and lungs from harmful substances. Protective cells also include cells that produce mucus, cells that have cilia (they help remove particulate matter and mucus from the respiratory tract), ciliary cells, as well as many other types of cells that play an important role in the formation of immunity, protecting the human body from pathogens organisms and harmful substances. The cartilage layer, muscle and elastic fibers take part in the formation of the structure of the respiratory tract. Blood vessels, as well as lymphoid tissue, play an important role in the nutrition and protection of the bronchial walls. During contraction of muscle fibers, a change in the diameter of the airways occurs.
With the development of bronchiectasis, partial destruction or inflammation of the bronchial wall may be observed, ciliary cells may be damaged or partially destroyed, and mucus production may be increased. In addition, there may be a loss of normal tone of the bronchial walls, while the affected area becomes wider and flabby, protrusions, “bags”, which in appearance resemble small balloons, can form in it. Increased mucus production leads to an increase in the number of pathogenic microorganisms in the bronchi. An increase in the amount of infected mucus contributes to a decrease in bronchial patency and leads to further progression of damage to the bronchial wall. Inflammatory damage to the bronchi can involve quite large areas of the bronchi, up to the alveoli. In especially severe cases, vascular tissue is replaced with fibrous tissue, and destruction of the vascular wall of lung tissue can create additional stress on the heart. In addition, inflammation and an increase in the number of blood vessels in the bronchial walls can cause blood in the sputum, and mucus blockage in damaged airways can reduce the oxygen content in the blood.