The gastrointestinal tract consists of many sections, each of which performs its own function. When diagnosing diseases of the digestive system, it is not enough to focus on the nature of the symptoms; you also need to know where each department is located. Taking into account such knowledge, it is possible to quickly identify possible disturbances in the body’s functioning and predict successful and appropriate treatment for a particular patient.
Where is the colon located?
Colon and its parts
The colon is the main section of the large intestine. It begins in the area of the cecum and is divided into its parts. The cecum and colon are connected by the Busi sphincter, which ensures the movement of products from one part to another part of the gastrointestinal tract.
Structure of the large intestine
On average, the described section of the intestine has a length of one and a half meters, and the diameter of the intestines can vary depending on the characteristics of the patient and is 5-8 cm. Since the colon is one of the largest parts of the large intestine, it has a large number of sections - ascending, transverse, descending and sigmoid.
The first part is not involved in the process of digestion and breakdown of food, but it is in the ascending intestine that the main absorption of water and other liquids occurs. Liquid stool also passes through it, which gradually turns into solid feces. The section itself is located on the back wall of the abdomen on the right side. The length of the ascending part varies between patients and can be 12-20 cm.
What is the colon
Attention! Connects the colon to the transverse colon by several bands of the colon. In the anterior part of the abdomen there is a free band, the omental band has moved slightly backward, and the mesenteric band is closer to the posterior wall of the peritoneum. The latter forms a bend and in the area of the right rib passes into the transverse colon.
The length of the transverse intestine is half a meter. For this section of character there is a separate mesentery, which connects to the mesenteric band. Gradually, this part passes into the descending colon, which is why a sharp angular transition is formed. This part is fixed using the diaphragmatic-colic intestinal ligament. The descending section has a length of 20-22 cm, the diameter is noticeably smaller than that of the previous two intestines.
Parts of the human colon
The sigmoid colon is located on the left side in the ileal fossa. It gradually moves towards the pelvis and goes into the rectum in the sacrum area. The average size of the sigmoid colon is 55 cm, but there have been cases when this section significantly exceeded or did not reach the average normal values.
Attention! This section is the last in the colon. Additionally, it has two more loops that are located directly on the iliacus and psoas muscles. This will ensure more coordinated operation of the entire system and reduce the likelihood of problems with bowel cleansing.
Ascending colon
Transverse colon
Descending colon
Sigmoid colon
Diagnostics
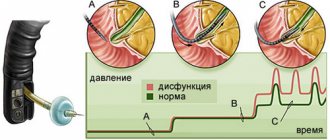
Diagnosis of the disease begins in the doctor’s office, who collects all the information from the patient, asks in detail about the condition, what symptoms are troubling and for how long. It is important to name all the symptoms of the disease, so the doctor can first assess the situation and decide what to do next. Next, the patient’s abdomen is examined, palpated and tapped. If suspicions are confirmed, the doctor examines the anus using a rectal speculum. To get more accurate results, the following diagnostic methods are used:
- Fibercolonoscopy, in which a thin tube equipped with a microvideo camera is inserted into the rectum. Before the procedure, it is important to cleanse the intestines of feces the day before.
- X-ray using contrast agent. Helps to see intestinal diseases, the presence of tumors, excess fluid or air.
- Angiography, in which contrast is administered intravenously, followed by X-rays taken one after the other.
- An ultrasound of the colon will help the doctor examine changes in the rectum, whether there is inflammation, ulcers, or neoplasms there.
- MRI or CT diagnostics is the most highly informative method that allows us to examine intestinal pathologies in the early stages and determine the nature of the disease.
Causes of development of colon diseases
In order to prevent pathologies of this part of the gastrointestinal tract, you should know what they may be associated with:
- an insufficiently active lifestyle, and this condition is especially dangerous when it is associated with poor nutrition;
- frequent consumption of fatty foods;
- frequent constipation or diarrhea, which can be caused by infection, viruses and other pathogens;
- atonic constipation in patients over 65 years of age;
- accumulation of a large number of toxic substances, most often due to the consumption of low-quality products and frequent constipation;
- the need to constantly take various medications;
- frequent use of unjustified biological additives and laxatives.
Attention! These reasons can cause many different pathologies of the colon, from inflammation to severe oncological processes. Each of the disorders has its own symptoms and can lead to similar problems in other parts of the gastrointestinal tract.
Video - Anatomy of the colon
Symptoms of inflammation
Naturally, the first manifestations of an unhealthy process are disturbances in peristalsis, and, accordingly, in the evacuation of feces. The movement of masses through the intestines slows down, resulting in prolonged constipation. Or vice versa, persistent diarrhea may appear. In any case, intestinal atony develops, which leads to obstruction or other equally serious conditions, often requiring surgical intervention.
Other manifestations of dysfunction depend on the type of pathological process. Experts identify several of the most common diseases.
Hirschsprung's disease and its manifestations
Pathology refers to hereditary pathologies. The main manifestations of this problem in the colon are constant constipation, increased gas formation and bloating. Constipation can last from several days to several months and begins to manifest itself from the first days of a child’s life, sometimes from 3-5 years. It is often not possible to get rid of constipation even with the help of an enema. This condition may also be followed by severe diarrhea, which will lead to severe dehydration and exhaustion.
Hirschsprung's disease in children
To completely get rid of this problem, mandatory surgical intervention is required. It consists of completely removing the aganglionic section and increasing the length of parts of the intestine.
Attention! Such surgical interventions are recommended to be carried out at the earliest opportunity. If the operation is delayed, the child will constantly suffer due to a lack of vitamins and poisoning of the body.
Surgery for Hirschsprung's disease
Survival prognosis
The prognosis of colon cancer in the absence of treatment is unambiguous - death occurs in one hundred percent. After radical operations, people live five or more years in 50-60%, with superficial cancer (not reaching the submucosa) - in 100%. If there is no metastasis in the lymph nodes yet, the five-year survival rate is 80%.
Naturally, the more advanced and higher the stage, the more difficult it is to recover from cancer, and the chances of a long life drop. That is why it is important to be attentive to your health and seek medical help on time.
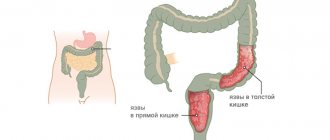
Nonspecific ulcerative colitis
It is one of the most frequently reported diseases. Refers to chronic processes. The disease manifests itself as a large number of ulcers on the mucous membrane. Infections and immune processes in the body can provoke such a disorder. The disease manifests itself as constant diarrhea, while blood, purulent masses, and mucus can be released with feces. Severe pain must be recorded. The patient also has a decrease in hemoglobin levels, severe weakness and disturbances in liver function.
Not everyone has heard about the colon, but this does not diminish its important role in the digestive system. It consists of transverse, ascending, descending and sigmoid parts. In general, its length can reach one and a half meters, and is curved in the abdominal cavity. How to recognize that it is she who is hurting? What disease can discomfort be a symptom of? The answers to these questions are in this article.
- Ascending, the length of which is 10-25 cm. This is the beginning of the colon, located on the right of the abdominal cavity, and is a continuation of the blind part of the intestine. May vary depending on the position of the person's body. When in a vertical position, its base is directed downward. It becomes transverse, forming the hepatic flexure.
- Transverse - length is 45-60 cm. In its location it comes into contact with the stomach, liver, gall bladder, and resembles a loop in shape. The transverse part forms the splenic flexure. Stretches to the right from the costal cartilage to the left hypochondrium.
- Descending - length varies from 10 to 25 cm. The descending colon is located on the left side of the abdominal cavity. Its continuation is the sigmoid part of the digestive system.
- Sigmoid - length ranges from 20 to 50 cm. The origin is the iliac edge of the posterior crest from above. It forms two loops, one with the convex part down. The second loop is distal, located upward on the psoas muscle. The final part of the colon passes into the rectum.
Causes of colon pain
You can understand that problems have begun in the colon of the intestine by the following signs: discomfort near the anus, pain in the lower abdomen, constipation, flatulence, the presence of blood discharge and pus in the stool. All these symptoms can be the beginning of serious diseases, for which only a doctor can identify and prescribe treatment.
Diseases
- Polyposis. Polyps or lipomas form on the mucous membrane of the colon. Their sizes range from a few millimeters to several centimeters. The first symptom of the disease is problems with stool, as growths interfere with the passage of stool. Large polyps can cause hemorrhage in the intestinal area. Treatment is carried out surgically or with the help of cytostatic drugs.
- Hirschsprung's disease. This is a hereditary disease that develops in early childhood. The parts of the intestine located above the colon hypertrophy, preventing it from emptying itself. The disease develops as a result of the formation of ganglion cells. The patient is scheduled for surgery to remove the inflamed hypertrophied section.
- Diverticulosis. The disease can be congenital or acquired. It occurs as a result of protrusion of the mucous membrane through the muscle mass of the intestine. Feces get stuck in them, forming inflammation of the organ mucosa. Sometimes a symptom of a disease does not appear for a long time, but sooner or later it makes itself felt. The patient experiences vomiting, diarrhea, and severe pain in the lower abdomen. In the early stages of inflammation, the temperature rises. Treatment is carried out with medication, and if complications develop, in a hospital hospital.
- Crohn's disease. It occurs as a result of immune inflammation on the walls of the gastrointestinal tract, forming fistulas, ulcers and abscesses in the mucous membrane. Crohn's disease is a hereditary and chronic disease, and it can also be triggered by smoking. Antibodies are formed in the mucous membrane, they can ascend and spread throughout the digestive system, as well as in the stomach and esophagus. The patient immediately loses weight, suffers from sharp pain, inflammation in the anus, nausea and bouts of diarrhea. Treatment consists of medication and supportive therapy. During the period of acute development, surgery is prescribed to remove the inflamed area.
Oncological diseases
A tumor in the colon appears as a result of an advanced form of the disease and inflammation. Hereditary predisposition plays a major role. Obesity, a sedentary lifestyle, an unbalanced diet, frequent constipation - all this can be the beginning of the acute development of oncology. The symptoms are quite similar to other ailments: colic in the lower abdomen, diarrhea, mucus and blood in the stool. As cancer develops, complications worsen. Treatment depends on the forms and stage of the disease. An operation is performed to remove inflammation. If metastases are detected, chemoradiotherapy is prescribed.
- Adenocarcinoma. A common form of cancer. Neoplasms affect the mucous area and organ cells, quickly spreading metastases.
- Signet ring cell carcinoma. The disease is formed as a result of the accumulation of signet ring cells filled with mucus, unconnected to each other.
- Squamous cell carcinoma. The tumor is formed from squamous epithelial cells. Dangerous oncology, high risk of death. This diagnosis is extremely rare.
- Undifferentiated cancer. Oncological formation consists of cells that do not secrete mucus and are not components of the glands. They are separated by connective tissue stroma, forming cords.
- Unclassified cancer. Malignant tumors that do not fit any description of other forms of cancer. Rarely seen.
Treatment of the sigmoid colon
Inflammatory processes can be suppressed with medication, while structural changes in the department require surgical intervention. Before treating the sigmoid colon, it is necessary to identify the etiology of the pathological process and promptly eliminate the main provoking factor from the patient’s life. Then remove the pain with painkillers, proceed to intensive therapy, supplemented by a therapeutic diet and physiotherapeutic procedures for medical reasons.
Conservative therapy
Drug treatment is aimed at removing the cause and consequences of inflammation, and is additionally monitored by clinical methods. The intensive therapy regimen involves a combination of representatives of several pharmacological groups to enhance the overall therapeutic effect. This:
- antispasmodics to relax smooth muscles: Spazmalgon, No-shpa;
- enzyme-containing preparations: Mezim, Creon, Festal;
- antibiotics to kill bacteria: representatives of the fluoroquinolone group;
- antihistamines against allergic reactions: Fenistil, Suprastin, Tavegil;
- immunosuppressants: Daclimusa, Cyclosporine, Azathioprine;
- anti-inflammatory drugs: Prednisolone and its analogues;
- adsorbents to prevent stomach ulcers: Smecta;
- probiotics to normalize intestinal microflora (Enterol, Linex);
- enemas, rectal suppositories with a favorable prognosis for the disease.
- multivitamin complexes to restore the immune system after long-term treatment of the sigmoid colon with medications.
Surgical methods of treatment
If conservative methods are ineffective, doctors recommend a radical approach to the problem. The patient requires surgery on the sigmoid colon with preliminary radiation therapy. Such surgical intervention is appropriate for oncology of the sigmoid colon. First, its size is reduced by an acceptable dose of radiation, and then completely removed. An additional course of chemotherapy and radiotherapy is necessary to prevent the spread of metastases to healthy parts of the digestive system. For polyps, resection of the pathological focus is recommended.
The meaning and work of the organ
The colon encloses the small intestine. The ascending part occupies the right corner, the transverse part is located at the top of the abdominal cavity, the descending part is on the left, and the sigmoid part is located at the bottom left. Does not participate in the digestion process. Digested food comes from the small intestine. In the ascending part, the absorption of liquid, vitamins, and microelements begins, gradually forcing it to descend through the remaining parts. A substance, chyme, is released from the thin section, under the influence of which solid feces are formed.
Functions
- Absorption of water and salts. Every day, up to 2 kg of food mass (chyme), which is largely represented by water, enters the large intestine. The intestines absorb from 1.4 to 1.9 liters of water per day, mainly in the ascending colon. Salts of sodium, potassium, chlorine, and calcium are also absorbed in the colon. After absorption of all the necessary electrolytes and water, 200-300 g of intestinal contents remain, which is formed into feces.
- Formation of feces. With the help of peristaltic movements, the intestinal contents are mixed and gradually moved towards the rectum. The descending colon and sigmoid colon accumulate feces, which, at a certain mass, create pressure on the sphincter in the rectum and cause the urge to defecate. This accumulation allows you to avoid the constant release of feces from the intestines in an unregulated manner.
- Synthesis of vitamins (group B and vitamin K). The main source of B vitamins and vitamin K are intestinal bacteria.
- Mucus formation. The secretion of mucus by goblet cells in the large intestine allows stool to move better through the intestines. There are practically no enzymes in mucus.
- Digestion. Compared to the small intestine, the colon is practically not involved in digestion. Absorption of small amounts of glucose and some amino acids synthesized by intestinal microorganisms may occur.
Read on: Where does the digestion process begin?
Examination methods
Constant sharp pain in the lower abdomen and digestive system problems may be a sign of the disease. It is necessary to consult a gastroenterologist who will prescribe examinations. The earlier the disease is detected, the more favorable the outcome of the disease.
- Irrigoscopy. X-ray, in which the desired section is filled with a suspension. With this study you can detect: fistulas, tumors, ulcers and polyps.
- Colonoscopy. It is carried out using a special apparatus that allows you to examine the intestine from the inside. This is the most accurate research method. During the colonoscopy procedure, you can remove a benign tumor, take a biopsy, remove a foreign object, and stop bleeding.
- Examination with a rectal speculum. The examination is carried out using a rectal speculum, inserting it 10-15 cm into the anus. The examination is not carried out in case of severe pain, inflammation or sphincter spasms.
Disease Prevention
Prevention of diseases of the colon, as well as the gastrointestinal tract, consists primarily of normalizing nutrition. It is recommended to consume more fiber, plant foods, protein, and enough water. Minimize the consumption of trans fats, quickly digestible carbohydrates, fast food and other heavy, fatty foods. Obesity also has a negative impact on the digestive tract.
Smoking and alcohol have a negative impact on all systems of the body, including the digestive processes, creating disturbances. There is also a genetic predisposition to diseases; such people need to be examined twice as often. Older people are also at increased risk. At the first sign of pain symptoms, visit a gastroenterologist or therapist. He will prescribe the necessary examinations to make a diagnosis and prescribe the correct treatment.
The colon is a section of the large intestine that immediately follows the cecum. The main function of the colon is the absorption of fluid and electrolytes and the formation of feces. Chyme, passing through the colon, becomes more formed.
The average length of the colon is 1.5 meters.
The colon consists of several sections:
24 cm. Transverse,
56 cm Descending,
The normal diameter of the colon is 5-8 cm.
The colon begins with the ascending section, which extends from the ileocecal angle to the hepatic flexure. The ascending section of the intestine is fixed to the posterior abdominal wall and is covered with peritoneum. Sometimes there is a mobile ascending colon, which occurs due to incomplete fixation by the mesentery or with a defective mesentery, which can cause volvulus.
The transverse colon starts from the hepatic flexure (right flexure of the colon) and extends to the splenic flexure. Outwardly it resembles a small loop, above or below the navel in the projection onto the anterior abdominal wall. Sometimes its location changes, and it can descend lower - into the pelvic cavity. The lower edge of this section of the intestine is connected to the greater curvature of the stomach by the gastrocolic ligament, called the greater omentum. The transverse colon is completely covered by the peritoneum, i.e. it has a mesacolon (its own mesentery).
In the place where the omentum is attached to the intestinal wall, there are no blood vessels, so in this place its intersection during surgery will be almost bloodless and effective.
The descending section of the intestine begins from the splenic flexure and continues to the entrance to the pelvic cavity. Fixed with the help of the peritoneum to the posterior abdominal wall. The next section, the sigmoid colon, starts from the entrance to the pelvic cavity and ends at the level of the ΙΙΙ sacral vertebra, i.e. beginning of the rectum. This section of the intestine is also completely covered by the peritoneum and has its own mesentery.
The sigmoid intestine has the most variable length: from 12 to 75 cm.
Throughout the colon there are fat pads filled with adipose tissue. The vessels carrying blood to these fatty pendants pass through the muscular layer of the intestine, so intestinal diverticula often occur in these places in old age.
There are three main functions of this section of the intestine: motor (motor), absorption, excretory.
In the colon, the liquid part of the chyme is absorbed, food components are recirculated, solid feces are formed and excreted. During the day, up to 1.5 liters of liquid chyme enters the colon, while almost 10 times less is excreted in the form of feces. The contents of the intestine become more dense, because water and electrolytes (calcium, magnesium, potassium, sodium) are absorbed.
In addition, the colon ensures the absorption of amino acids, vitamins (mainly fat-soluble), fatty acids and glucose. The digestive glands secrete enzymes, heavy metal salts, cholesterol into the intestinal cavity, and fiber is also broken down in this part of the intestine. Pectin fibers are completely broken down, cellulose is partially broken down, and lignin is not fermented at all.
An important role in digestion is played by the intestinal microflora, which consists of 400 or more species of aerobic and anaerobic bacteria. The predominance of anaerobic flora is considered normal. These are lactobacilli and bacteroides.
There are 1000 times more anaerobes than aerobic bacteria. About one third of the dry stool residue consists of bacteria. This must be remembered during operations on the gastrointestinal tract or intestinal obstruction (paralytic). During these periods, the intestinal protective barrier is weakened, microorganisms and toxins can easily penetrate the bloodstream and abdominal cavity, so the intestines in this case are a source of serious infection.
Normally, intestinal flora ensures the synthesis of vitamins (K, C, B), promotes the physiological fermentation of food and determines the protective function of the intestines.
How to check the sigmoid colon
The basis of the clinical examination is ultrasound and radiography. It is obvious on the monitor screen that this section is pathologically enlarged, displaced, and exerts negative pressure on other structures of the digestive system (this is in advanced cases). Diagnosis of the sigmoid colon starts with the collection of medical history and patient complaints, and necessarily includes a study of the composition of stool and a biochemical blood test in the laboratory. Additionally, the doctor prescribes sigmoidoscopy, colonoscopy, followed by an intensive therapy regimen.
Palpation
During the first examination of the patient, the doctor tries to palpate the suspected focus of pathology. Pain on palpation of the sigmoid colon is sharp, disrupts breathing, and only increases with prolonged exposure. It is correct to palpate the problem area only through the anus, while checking the elasticity of the walls and their structural integrity. A rectal examination of the Rossi-Muthier sphincter is performed by a highly specialized specialist - a proctologist.
Frequent illnesses
The number of people with inflammatory and tumor diseases of the colon is growing. This can be explained by the following factors:
- improper diet, eating large amounts of fatty foods and processed foods.
- restriction of physical activity, many people now lead a sedentary lifestyle, almost all people in this category can show symptoms of damage to the large intestine.
- If a person suffers from chronic constipation, intestinal atony or hypotension, especially in old age, this can lead to severe intestinal diseases.
- entry of carcinogens into the intestines in large quantities.
- the use of a large number of drugs and biological additives.
Diseases such as colonic dyskinesia, colon cancer and diverticulosis are common. Many symptoms of colon diseases disrupt metabolic processes in the body; clinically they look like this:
- Pain syndrome (in the abdomen and anus).
- Mucus and pus from the anus.
- There is bloody impurities in the stool or severe intestinal bleeding.
- The patient is concerned about constipation.
- Anemia.
- Flatulence (bloating) of the intestines.
- Obstruction at the level of the large intestine.
- Tenesmus - the urge to have a bowel movement (painful).
- Liquefaction of stool.
- The patient sometimes cannot hold in gases and feces.
As you can see, the symptoms are predominantly general, but specific to colon disease.
It is dangerous if a patient fails to consult a specialist in a timely manner for such serious diseases as colon cancer, which can lead to severe complications and death. The symptoms of this disease are as follows: disruption of the normal bowel movement due to a malfunction of the motor function of the intestine, diarrhea and constipation, abdominal pain, disturbance of the general condition and well-being of the patient, the appearance of pathological impurities in the stool (blood, mucus), a tumor felt during palpation examination in the abdominal cavity.
Colon cancer often simulates other diseases depending on the location: appendicitis, gastric and duodenal ulcers, cholecystitis, adnexitis. These diseases are characterized by similar symptoms.
Any symptoms characteristic of colon cancer may accompany other diseases. Such patients are hospitalized in a general surgery hospital with a diagnosis of intestinal obstruction. In 35% of cases, the patient is admitted to the infectious diseases or therapeutic department with a diagnosis of anemia of unknown origin or dysentery. This increases the percentage of diagnostic errors when detecting colon cancer. X-ray and endoscopic examination of the intestine will help to make a correct diagnosis. It is also important for the doctor to perform a palpation examination of the patient; this will help to find out the location, size of the tumor, and its consistency. It is believed that intestinal cancer is palpable in more than half of cases.
The most common pathology of the colon is dyskinesia, or irritable bowel syndrome.
Intestinal dyskinesia is a violation of its motor function, without changes in organic properties. Such disorders are caused by improper diet, hereditary factors, constipation, and diseases of the endocrine system. In children, symptoms of dyskinesia occur with early transfer to artificial feeding, with a tendency to food allergies, or acute intestinal infections in infancy.
Dyskinesia develops in people prone to psycho-emotional stress, with spinal disorders, damage to the central nervous system, and the use of certain medications.
The symptoms of this disease vary depending on the type of dyskinesia: hyper- or hypotonic. The patient may be bothered by constipation and diarrhea; sometimes feces irritate the intestines if their quantity is excessive. Weakness of the muscle sphincters occurs, and stool may appear. Due to dysfunction, the bowel movement pattern, its diameter gradually expands. Pain appears with prolonged retention of stool and disappears after bowel movement. Dyskinesia can be treated with diet, physiotherapeutic methods and medication.
The colon is the longest section of the large intestine, which includes several parts.
Stages
Like all cancer diseases, this type of cancer has several stages of development.
- Stage zero, characterized by the development of carcinoma from the epithelium without affecting the lymph nodes. Metastases do not spread.
- The first stage of colon cancer is caused by tumor growth under the epithelial layer, and then into the muscle layer. Metastasis does not occur.
- The second stage is A, in which the neoplasm affects the tissue adjacent to the colon. Metastases do not spread throughout the body.
- The second stage B, in which the cancer affects other organs and grows into the visceral pleura. There are no metastases.
- The third degree A is characterized by the growth of the tumor into the muscle layer, the appearance of metastases in three regional lymph nodes.
- Third degree B, when cancer grows into tissues located near the organ, as well as other organs, lymph nodes.
- The third stage C is caused by the spread of the tumor to all layers of the organ, damage to other organs and lymph nodes.
- The fourth degree, in which large areas are affected, lymph nodes, and metastases spread throughout the body.
Sections of the colon
Features of the anatomical location of the intestine in the abdominal cavity made it possible to divide it into 4 sections:
- Ascending colon.
- Transverse colon.
- Descending colon.
- Sigmoid colon.
The total length of the four parts reaches 1.5 -2 meters.
Ascending colon
The intestine is located to the right of the midline of the abdomen (right flank) in the abdominal cavity. Being a continuation of the cecum, it rises up to the lower edge of the liver. At this level, it forms the right flexure of the colon (hepatic flexure) and passes into the transverse part of the large intestine. The length of the ascending part is about 15-20 cm. The ascending part is topographically limited from behind by the quadratus dorsi muscle and the right kidney, above by the right lobe of the liver and gall bladder, in front by the anterior abdominal wall, and inwardly by loops of the small intestine. In a small number of people, the intestine has its own mesentery, which ensures its mobility and the development of volvulus of the cecum and colon (in rare cases).
Transverse colon
The ascending and descending sections of the large intestine are connected to each other by the transverse colon. The intestine is located in a horizontal plane, slightly sagging downwards. It originates from the hepatic flexure and reaches the left hypochondrium, forming the splenic flexure (left flexure of the colon). The left flexure is located above the right flexure of the colon. When palpating the abdomen, it can be detected above the navel in the form of a horizontal elastic cord.
The length of the transverse colon varies from 25 cm to 65 cm in an adult. The transverse colon is bounded on the right by the liver, on the left by the stomach and spleen. The duodenum and pancreas are located behind the intestine, and the loops of the small intestine are adjacent below. The anterior part is covered by the anterior abdominal wall. In the abdominal cavity, it is attached to the walls using the mesentery.
Descending colon
It starts from the left flexure of the colon and descends to the left iliac fossa, passing into the sigmoid colon. Posterior to the intestine lies the left kidney and the quadratus dorsi muscle. Covered in front and left by the abdominal wall. The right side of the descending colon is adjacent to the loops of the small intestine. The length of an adult varies from 10 to 30 cm.
Sigmoid colon
It is located in the left iliac region and forms 2 loops: proximal and distal, which lie on different muscles. The proximal part is supported by the iliacus muscle, and the distal part by the psoas major muscle. The length of the sigmoid colon can be from 15 cm to 50 cm in an adult. Near the intestine there is the left ovary, uterus, and bladder.
Complications
Colon cancer in the absence of timely treatment is characterized by the presence of a number of complications.
- Obstructive intestinal obstruction. It occurs as a result of blockage of the lumen by pathological tissues. It is considered a defining sign when the descending section (left side) of the colon is affected. Detected in 15% of patients.
- Perifocal inflammatory and purulent processes. The formation of abscesses and phlegmons in the tissue is typical for pathologies in the ascending section (right side) of the affected organ. It is observed in 10% of patients.
- Perforation of the intestinal wall. It is observed in 2% of patients, since this complication most often leads to mortality. This is due to ulceration and decay of tumor tissue, which causes rupture of the organ, inevitable penetration of fecal contents into the abdominal cavity and the development of peritonitis.
- Tumor invasion of neighboring organs and development of interorgan fistulas (intestinal-vaginal or vesical). Characteristic of the later stages of the malignant process. In this case, the prognosis for 5-year survival is disappointing.
Wall structure
Located in the abdominal cavity, throughout the entire length of the wall of the colon are formed by the following layers (membranes):
The mucous membrane lines the inner surface of the intestine. It contains epithelial cells, between which there are a large number of endocrine glands. The glands bend to form crypts. Each crypt contains goblet cells that produce mucus to facilitate the passage of feces. The surface of the crypts is dotted with cells with a set of villi and enzymes for breaking down substances that enter the intestines. The mucous layer also contains blood vessels, clusters of lymphatic plaques (follicles), nerve endings and single muscle fibers. Lymphatic follicles are of great importance in the development of immunity in childhood. Protrusions of the mucous wall increase the absorption surface of the intestine several times.
The submucosa is a connective tissue with a high content of nerve fibers, lymphatic follicles, and blood vessels.
The muscular coat is formed by thick layers of internal muscle fibers (circular layer) and external fibers (longitudinal layer). Nerve plexuses are located between the layers. The longitudinal layer consists of three ribbon strands throughout the entire colon. Between the muscle fibers, the intestinal walls protrude, forming haustra. The haustrae are separated by circular muscle fibers. Contraction of haustra ensures better movement of feces.
The serosa is the outer lining of the colon. There are fatty growths on its surface. The role of the processes is not fully understood.