What are esophageal diseases
Pathologies of the esophageal tube include conditions accompanied by damage to the walls of this organ, disturbances in peristalsis, the process of moving food from the mouth to the stomach, and the appearance of malignant and benign neoplasms. The proximity of this section of the gastrointestinal tract to the heart causes difficulties in diagnosing diseases; with chest pain, people rush to see a cardiologist instead of a gastroenterologist.
Diseases from which the esophagus suffers can be different, and these ailments will cause pain, very often accompanied by symptoms in the form of frequent belching, unpleasant odor and heartburn.
So, if a person is affected by this organ, then he may suffer from achalasia cardia, peptic esophagitis, diaphragmatic hernia or esophageal spasm of the esophagus. Generally speaking, the above diseases, which are also the most common, usually occur when the motility of the esophagus is impaired. Otherwise, this is facilitated by neoplasms in the form of cysts (benign tumors) and cancer.
Looking more specifically at diseases of the esophagus, it should be noted that cardiospasm (achalasia cardia) belongs to the category of neuromuscular ailments. As for the reasons, they have not yet been determined, but it is known: this disease manifests itself in people from 20 to 40 years old. Most often women suffer from it.
If a child has been diagnosed with such a disease, then it may be accompanied by certain symptoms: bronchopneumonia or some other disease that affects the respiratory tract, and this is facilitated by the food that has entered them.
Symptoms that are specific to achalasia itself can be of a different nature. In this case, swallowing is primarily impaired or so-called dysphagia occurs, which occurs both suddenly and gradually. If a person is nervous, this symptom intensifies. Sometimes dysphagia is observed, which has a paradoxical specificity. When it occurs, hard and dense products pass through normally, but liquid ones do not. Swallowing may be impaired depending on the temperature of the food.
The next stage, which is characterized by the manifestation of achalasia, is regurgitation. This sign makes itself felt when there is overflow of the esophagus, and the muscles contract. The last symptom of this disease includes pain, which is observed due to muscle spasms formed due to overfilling of the esophagus. In this case, some patients experience nausea, burning, belching, and increased salivation.
In medical practice, diseases of this organ are recognized as the most common. There are congenital and acquired types of diseases that affect the esophageal canal. Congenital malformations include malformations of this organ, which can manifest themselves even during the first months of a child’s birth.
The most common acquired disease is called diverculum of the esophagus, in which protrusion of the organ wall occurs in the form of a pocket. With this pathology, there is a violation of the swallowing reflex, a burning sensation in the chest, and vomiting.
Cardiospasm of the organ represents a chronic spasm of the lower sphincter. With this disease, there is a violation of muscle tone and motility of the entire organ. Food is retained in the enlarged part of the organ and causes spasm. The disease is characterized by difficulty swallowing solid food and regurgitation while eating.
Esophageal candidiasis is provoked by a large number of yeast fungi that affect the esophageal mucosa. This disease affects people who have undergone chemotherapy and AIDS patients. The symptoms of the disease are similar to other diseases of the esophagus.
A chemical burn of an organ occurs as a result of contact with caustic liquids. The disease is fraught with cicatricial narrowing or complete obstruction of the organ.
It is no less difficult and has dangerous consequences of blocking foreign bodies in the narrow passage of the digestive canal. This can cause a rupture of the organ wall. When scarring occurs, this human organ shortens in some part of it, which contributes to the formation of a diaphragmatic hernia. When the contents flow back, bile enters the organ, creating conditions for the appearance of ulcers and erosions.
Here is a list of the most common signs, the presence of which indicates that the esophagus is currently in serious trouble.
- Problems swallowing, pain - similar difficulties are secondarily called dysphagia.
- Sore throat, similar to that that occurs with a sore throat or cold.
- Unexpected pain in the chest, for no apparent reason. Moreover, the intensity of such pain can be extremely strong, so it is sometimes confused with an attack of angina.
The listed symptoms can be considered fundamental for diseases of the esophagus, but usually, heartburn, accompanied by severe belching, is its integral companion. An unpleasant sensation of “metallic” taste constantly persists in the oral cavity, and copious salivation is noted.
Of course, the final verdict (diagnosis) is the prerogative exclusively of a specialized medical specialist. However, if such problems occur in the esophagus, you should be especially wary and visit the necessary doctor. Close attention should be paid to the issue of nutrition.
Now we’ll talk in more detail about the main diseases that can bring massive troubles to this organ.
The first in line is esophagitis, which is characterized by inflammatory damage to the mucous membrane of the esophagus.
Violations in the functioning of organs
When comparing the incidence of diseases of the esophagus and stomach, doctors note higher statistics for the latter organ, since the passage of food does not cause such frequent development of pathologies as the direct process of digestion of incoming substances.
The advantage of the esophagus in the development of various diseases is that it has a simple structure and does not carry out long-term vital processes. The stomach performs a considerable number of functions for the body and is the center of normal absorption and digestion of food, therefore it is more susceptible to the influence of negative factors.
Disruption of the activity of one of these organs implies the appearance of various diseases that can introduce pathological changes in the functioning of the body. Therefore, the main preventive method is to ensure the normal functioning of all vital systems.
Developmental defects
Even in the womb, the fetus develops this organ in the third week. At first it is the primary swallowing gut, which is later divided by a parallel membrane into the anterior respiratory and posterior esophageal. From the foregut the stomach, liver, pancreas, primitive pharynx and esophagus are formed.
Later, on the surface, as a result of splitting into two parts, the first signs of an organ and trachea are formed. During the same period, cases of the development of certain defects may be observed - artesia, tracheoesophageal fistula and esophageal stenosis. If development occurs in a normal course, then by the age of two the beginning of the organ in a child is located at the level of the fourth cervical vertebra, by the age of twelve - from the fifth, in an adult - from the sixth, in an elderly person - from the seventh.
The structure and function of the human esophagus can be disrupted as a result of abnormal development. This is often facilitated by the negative impact of a polluted environment, ionizing radiation, and harmful working conditions that involve prolonged contact with toxic compounds (heavy metal salts, mercury vapor, arsenic). The most common types of pathologies are:
- Atresia. This type of pathology is characterized by complete occlusion of the lumen of the esophagus. It is noticed immediately after birth, since after feeding the child regurgitates food, foam and mucus are released from the nasal passages and mouth. The danger of this condition is that aspiration pneumonia may develop. In this case, the baby can only be helped through surgical therapy.
- Stenosis. Typically, hypertrophy of the muscular tissue of the lining of the esophagus also leads to pathology. In this case, dysphagia leads to a pathological expansion of the food canal, where the accumulation of food masses stagnates, which causes the process of putrefactive fermentation.
- Tracheoesophageal fistula. A congenital pathology that results in abnormal communication between the trachea and esophagus. Because of this, there is no possibility of feeding the newborn through the mouth. Any intake of food causes a paroxysmal cough with severe cyanosis of the skin. Treatment is possible only surgically.
- Short esophagus. A disease in which dysphagia in a child causes a gag reflex with the presence of blood streaks. To eliminate this pathology, not only surgical intervention is used. Sometimes providing an elevated position of the body after eating, or during a night's rest helps relieve negative symptoms.
Bends of the esophageal tube
If you carefully examine the esophagus, the structure and functions of the organ are varied. The size of the tube may depend not only on age, but also on individual characteristics. With the development of pathologies, the esophagus can begin in the neck, but end at the location of the 8-10 vertebrae. This indicates an abnormal structure, its shortening and elevation of the remaining digestive organs into the sternum.
It is worth mentioning the bends of the tube. There are areas that change their position. Initially, the esophagus lies in the middle. But at the level of the 6th cervical vertebra it forms a slight bend. That is, the tube begins to go to the front.
After passing the second and third spine, the esophagus goes to the right. This area is usually called anteroposterior. It completely follows the physiological curve of the spinal canal. After the 2nd vertebra, a bend forms again. Then it passes forward due to the proximity of the aorta. After it has passed the diaphragmatic ring, an anterior displacement is observed.
The esophagus is considered a mobile part of the digestive tract, making it easy for doctors to perform surgery on this area.
Classification of esophageal diseases
Diseases of the esophagus can have different origins, course patterns, severity, and symptoms. For ease of diagnosis, they are divided into the following groups:
- Congenital anomalies detected at an early age:
- Extensions of different parts of the organ.
- A cyst located inside a cavity or attached to the outer wall.
- Tracheoesophageal fistula is an opening connecting the trachea and esophagus.
- A diverticulum is a protrusion of the wall of an organ in the form of a sac into the surrounding cavity.
- Stenosis is a narrowing of the tube lumen.
- Absence of an organ or its shortening.
- Partial or complete doubling.
- Specific and nonspecific acquired diseases:
- Diverticula.
- Acute, chronic and infectious inflammation (esophagitis, stenosis, peptic ulcer).
- Vascular diseases (varicose veins of the esophagus, hemorrhagic angiomatosis, angioma).
- Diseases that impair the functioning of the organ - neuromuscular dysfunction:
- Esophagospasm is a sharp short-term spasm, contraction of the muscular wall of the esophagus.
- Atony, paralysis - decrease or complete loss of muscle tone of the tube walls, impaired peristalsis.
- Achalasia is a neuromuscular disease that prevents the passage of food due to decreased peristalsis of the organ and the lower sphincter (cardia), which connects to the stomach, being constantly closed.
- Benign tumors (lipoma, rhabdomyoma, leiomyoma, angioma, myxoma, neuroma, fibroma).
- Malignant tumors (cancer - sarcoma, epithelioma).
- Mechanical injuries leading to the appearance of perforations (holes) in the walls of the tube.
- Chemical burns that cause scarring and adhesions.
- Foreign bodies entering the cavity and getting stuck.
External structure
The structure of the human esophagus is divided into three sections, which total 25 cm. Each part has its own boundaries. When considering the generally accepted classification, the following departments are distinguished:
- Cervical. The upper part is located at the level of the 6th segment of the cervical spine, and the lower border ends at the level of the 1st or 2nd thoracic vertebra. It originates at the end of the oral cavity, and is adjacent to the trachea (its upper part) and the larynx. On the sides of it are the lobes of the thyroid gland. The total length does not exceed 7 cm.
- Chest. The total length is 17 cm. The complexity of this topographical area is explained by the location of the aortic arches and the nerve plexus. Also at this level, the trachea is divided into bronchi.
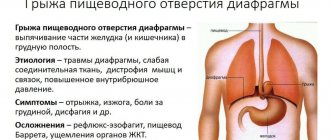
- Distal (the second name is cardiac). Despite the fact that this area is the shortest (no more than 4 cm), it is most often susceptible to the formation of hernial protrusions. The appearance of this pathology is explained by the weakness of the ligaments through which the esophagus is connected to the diaphragm (cordia).
In addition, this organ has two sphincters. In the upper section, it prevents food from flowing back into the pharynx. The lower sphincter prevents stomach contents from refluxing into the esophagus. The structural features include five natural constrictions. Obstruction most often occurs in these places, and food is retained in the event of dysphagia (impaired passage of the food bolus). There are three types of anatomical narrowings, which are:
- at the pharyngeal edge of the cervical spine;
- in the place of projection of the left bronchial tree of the thoracic segment of the spine;
- in the distal region (diaphragmatic region).
Nearby organs create physiological bends along the food canal. So in the area of the 6th cervical vertebra it deviates in front. Bypassing the area of the heart (in the area of the 3rd thoracic vertebra), it deviates to the right side. The position of the aorta causes a forward bend. The repeated forward bending is explained by its passage through the diaphragmatic ring. This body provides the following functions:
- motor, occurs due to the contraction of muscle fibers, which causes the passage of food to the stomach;
- special glands produce a special secretion, due to which a food lump is formed;
- acts as a barrier, due to which food passes in one direction;
- the synthesis of immunoglobulin occurring in the mucosal epithelium neutralizes the effect of viral and bacterial pathogens ingested.
In the internal structure of the human esophagus, there are four cellular layers, each of which provides a specific function. The muscle layer has a different type of structure. The movement of food in the upper section is facilitated by striated muscles, closer to the bottom it is formed by smooth muscle fibers.
The concentration of a large number of cardiac and esophageal glands ensures the production of internal secretions in the submucosa. The outer part (adventitia) is covered with pleural layers. It is especially pronounced in the diaphragm area. The inner epithelial layer differs in structure from the gastric layer.
If we consider the structure of the organ, then it is worth paying attention to the fact that in an adult the average length of the esophagus is about 25 cm, while it has a thickness with a diameter of 4 – 6 mm. The main parts of the organ are:
- cervical esophagus;
- thoracic esophagus;
- abdominal part of the esophagus.
The skeletotopy of this organ shows that, according to the location of the esophagus from the spinal column, it is located from the level of the VI-VII vertebrae and reaches the X-XI thoracic vertebrae. The anatomical diagram indicates the most basic parts of the esophagus, which play important functions in the functioning of the digestive system as a whole. These include the esophagus, lower food sphincter and stomach.
According to what the topography of the organ demonstrates, you can see that its upper part is located between the spine and the windpipe. The thoracic part of this organ also passes between the spinal column and the trachea, slightly lower between the aorta and the heart. The abdominal part fills the space between the cardiac part of the stomach and the diaphragm.
The structure of the esophagus includes a flattened tube, which has a thick layer consisting of the mucous membrane, the muscular layer, the lower part of the muscular layer, and the outer layer. The mucous membrane is covered by multi-tiered and flat epithelium of the esophagus. The muscular layer is divided into two layers, which perform the functions of narrowing and dilating the esophagus.
The lower part of the muscularis mucosa is responsible for the formation of its dense formation, which separates the esophagus and stomach. These are the sphincters of the esophagus. The outer surface of this system is lined with a layer that helps the esophagus connect to the surrounding organs. Due to its peculiarity, this organ can vary its thickness and length.
The anatomy of the esophagus, along with its structure and functional development, has a number of features that affect its proper functioning. We will talk about the blood supply to the esophagus, which is carried out in the cervical region from the lower thyroid arteries, in the thoracic region - through its own arteries.
The lymphatic system of the esophagus is a network of capillaries and vessels that dot all layers of the wall of the esophagus. A feature of the blood supply system is the collector vessels located along the entire path of the esophagus. They connect all lymphatic networks in all layers. An important aspect is the lymphatic topography of the esophagus, which demonstrates the direction of vessels from the cervical region to the deep cervical lower lymph nodes. Bypassing nearby nodes, it flows into the thoracic lymphatic duct.
Anatomy
The wall of the esophagus consists of a mucous membrane (covered with stratified epithelium), a submucosa (in which mucus-producing glands are scattered), a muscular layer (consists of an inner and outer layer) and a connective tissue membrane.
On the one hand, the structure of this organ is not so complex, but it is not so much the structure that is important as the functions that the esophagus performs.
Causes of inflammation of the esophagus
Diseases of the esophageal tube can be caused by a variety of reasons. The walls of this section of the gastrointestinal tract are sensitive to physical, chemical and other influences, infections, and food components. The following groups of factors contributing to the development of pathology are distinguished:
- Genetic, chromosomal - contribute to the occurrence of congenital diseases. They act on the fetus during intrauterine development.
- Mechanical – cause damage. This group includes poorly chewed food, hard foreign objects that have entered the digestive tract, and bones from meat and fish.
- Chemical - components of food, medicine, household or industrial reagents. This includes excessively salty, sour or spicy foods, alcohol, tobacco smoke inhaled into the esophagus, coffee, chocolate.
- Infectious – pathogenic microorganisms. The described section of the gastrointestinal tract can be affected in the presence of bacterial diseases of neighboring organs (inflammation of the tonsils). Observed in chronic or untreated diseases.
- Thermal - exposure of epithelial cells to too high or low temperatures when consuming hot or cold food or drinks.
How to resist the onslaught of diseases?
The best countermeasure is prevention. Vary your diet with foods that are high in fiber, low in fat and rich in quality protein. Stop smoking, do not drink alcohol, especially strong drinks, and food and drink should not be too hot. Don't eat late. So, the last meal is allowed at least three hours before bedtime. The fight against excess weight is not the least important in the prevention of esophageal diseases.
https://youtu.be/LkYteXUaYhQ
Introduction to the esophagus
According to what the topographic anatomy of the organ demonstrates, the following can be described: in the upper location, the thoracic esophagus is adjacent to all segments of the thoracic vertebrae - from the second to the eleventh. The bends of the esophagus on the frontal and sagittal planes are small.
At the top of the space, the esophagus is located at the back of the trachea. At the level of the division of the trachea, the esophagus on the left side is adjacent to the right posterior part of the aortic arch. In this condition, it borders the left carotid and left subclavian arteries. The thoracic duct passes between them.
The aortic arch forms a small depression on the wall of the organ, which contributes to the occurrence of a second narrowing of the organ. The left laryngeal nerve runs along the left side.
Along the walls of the organ, the arteries passing through it diverge at the base. Along these walls in the fiber there is a nerve plexus, which is formed by the branches of the vagus nerves, spinal nerves and lymph nodes.
Syntopy of the esophagus indicates a convenient location of nearby organs. In front is the trachea, which slightly covers the right side of the organ. It contains the left nerve, which is directed towards the larynx. The anterior wall of this organ borders the thyroid artery, which is on the lower left. The right recurrent nerve abuts its lateral part.
Arteries nourish the organ from several sources, creating an abundant communication of blood vessels.
Where is the esophagus located?
The esophagus is the connecting chain between the oropharynx and the body of the stomach. The anatomy of the organ is quite complex. It has its own innervation and a network of feeding vessels; glands that produce secretions open into the cavity. The wall is multi-layered, with natural bends and narrowings throughout.
The topography places it between the 6th cervical and 11th thoracic vertebrae, behind the trachea. The upper segment is adjacent to the lobes of the thyroid gland, the lower, passing through an opening in the diaphragm, connects to the stomach in its proximal part. The posterior part of the esophagus is adjacent to the spinal column, the anterior part is adjacent to the aorta and the vagus nerve.
You can see where the human esophagus is located; the photo gives a schematic idea.
Treatment of esophageal diseases
https://youtu.be/963o3iIGjtw
Various diseases of the esophageal tube are characterized by general and specific symptoms. A number of signs accompany any pathology of this part of the gastrointestinal tract. These include the following diseases of the esophagus and their symptoms:
- Heartburn is a burning sensation in the neck and behind the sternum. The acidic contents of the stomach are released into the esophagus. It intensifies after eating, when the patient takes a horizontal position, during physical activity, and bending. Suppressed after drinking water and antacids. It happens with esophagitis, a violation of the walls of the organ.
- Odynophagia – pain in the chest when eating food. Occurs when the mucous membrane is damaged. It is observed with esophagitis, tumors, ulcers, and chemical injuries.
- Atypical pain in the chest area - occurs spontaneously or during meals, their nature changes throughout the day. They may be accompanied by depression, anxiety, depression, panic attacks, and sudden mood swings. Present in esophagospasm, reflux esophagitis, and impaired peristalsis.
- Regurgitation (belching) is the movement of food in the opposite direction, from the esophagus to the oral cavity. Often accompanied by heartburn. In this case, food particles may enter the respiratory tract. Observed with diverticula, gastro-food reflux.
- Dysphagia is difficulty in moving solid and liquid food through the gastrointestinal tract when swallowed. Caused by the consumption of certain foods (for example, rich in fiber), damage to the parts of the nervous system responsible for swallowing.
As for a disease such as esophagospasm, during its development symptoms are observed that are characteristic of any disorders of the digestive tract. This pathology is more often found in men (middle-aged or elderly). Most often, patients suffer from pain that appears in the sternum, for this reason some people mistake this ailment for angina.
If we talk about peptic esophagitis (reflux esophagitis), then when it develops, the contents of the stomach are thrown back into the esophagus. These manifestations are also observed with achalasia cardia, but here there is a suspicion of a hernia of the esophageal diaphragm. In this case, the esophageal mucosa suffers from the above symptom, and the appearance of inflammation and ulcers cannot be ruled out, which leads to scarring of the esophagus and its narrowing. This disease progresses quite slowly. It can often be observed in infants.
It should be noted that the symptoms are no different from those inherent in the above diseases. So, this is belching, acute or dull pain and heartburn. Sometimes these signs can intensify if the person bends over or takes a lying position.
In some cases, exacerbations are observed during smoking and abuse of alcoholic beverages. At the same time, it is also necessary to take into account that belching can lead to aspiration pneumonia, since gastric contents sometimes enter the respiratory tract. Most often this happens if regurgitation catches a person at night.
But as for a diaphragmatic hernia, it can be either congenital or acquired, as well as caused by injury. In most cases, the symptoms are quite sparse. In many cases, it manifests itself as anemia or hidden bleeding.
The thing is that neoplasms (benign in nature) that arise in the esophagus develop very slowly and do not manifest any symptoms. Therefore, timely diagnosis plays an important role here, and the disease itself can only be determined with regular preventive examinations.
Blood supply in the esophageal tube, segments and proximity
The anatomy of the organ has its own characteristics.
It all depends on which parts of the digestive tract the esophageal tube is adjacent to. In medicine, there are 8 types of segments:
- supra-aortic and aortic area - adjacent to the aorta;
- bronchial and subbronchial. Adjacent to the bronchi;
- interaortobronchial. Located next to the aorta by the bronchi;
- retropericardial. Passes by the pericardium;
- supradiaphragmatic, intradiaphragmatic and subdiaphragmatic. Adjacent to the diaphragm.
The esophagus passes through several sections at once. Next to it there are several important parts of the body: trachea, aorta and left bronchus, pericardium. If any pathological processes occur, pain can occur both when swallowing and in the heart area, which makes diagnosis difficult.
If the pleura is adjacent to the esophagus, this leads to difficulties when performing surgical interventions. Then the inflammatory process from the esophageal tube moves to the pleura, heart and nerve endings.
Moving into the abdominal cavity, it interacts with the diaphragm. On the other sides is the liver and part of the gallbladder.
It is important to know not only about the structure of the esophageal tube, but also how it is supplied with blood. This process is carried out thanks to the arteries. They pass through the thyroid artery, the thoracic region of the aorta and the gastric branch. The outflow of venous blood is observed in the thyroid, gastric, paired and semi-gyzygos veins.
The lymphatic system gradually drains through the vessels into the lymph nodes. The second part bypasses them and enters the thoracic duct.
The organ is supplied with blood through the vagus, glossopharyngeal and sympathetic trunk. When they are squeezed, the pupil dilates.
Main functions
During the passage, food that passes through this organ is generously lubricated. The secretory glands of the esophagus are involved in this, which line the cavity of the organ, thereby helping the food bolus easily pass to its destination.
The protective functions of the organ help prevent food from entering from the stomach in the opposite direction, avoiding reflux, giving it only one direction. The speed of peristalsis in the organ is about five centimeters per second. Coordination of organ function is caused by voluntary and involuntary mechanisms.
When motor function is impaired, esophageal dyskinesia occurs, associated with impaired thoracic peristalsis and disorders of the esophageal sphincter. This may be preceded by increased and decreased contractions of the esophageal muscles.
Mechanism of food swallowing
Swallowing is a complex process in which food enters the pharynx from the mouth and moves further through the esophagus into the stomach. Initially, this function is carried out consciously, and then automation is developed, requiring precise coordination of other body systems:
- The tongue pushes the bolus of food directly to the pharynx;
- The palatal membrane automatically lifts to prevent bolus food from entering the sinuses;
- The epiglottis obstructs the larynx to prevent food from entering the respiratory system;
- Opening of the upper esophageal sphincter to further move food into the stomach;
- Alternate contraction of the esophagus to ensure the necessary pushing of food into the stomach;
- The upper gastric sphincter opens and the bolus enters directly into the stomach.
Diagnostics
If a doctor has identified a particular disease in the early stages, then esophagotonocymography is used. In some cases, X-ray diagnostics are used, which can detect the deformations that have occurred in the specified organ.
Sometimes it is necessary to bougienage the esophagus, that is, insert a specific probe. It is capable of expanding the organ, and the bougie itself can have a flexible or rigid structure. This remedy is also used during other diseases.
Before using any diagnostic method, an experienced doctor interviews the patient about symptoms that are characteristic of diseases of the esophagus.
Diseases of the stomach and esophagus are diagnosed using various methods using high-tech equipment. The necessary information about the course and causes of the disease is obtained by applying the following procedures and techniques:
- X-ray examination - contrast fluoroscopy. X-rays are taken before and after the administration of a contrast agent (barium sulfate). Using this method, it is possible to characterize the position of the esophageal tube in the chest, its size, the diameter of the internal canal, the general condition of the walls, and the filling of the organ. The images reveal the reasons for the difficulty in passing food particles and deformation. Provocative tests are carried out - fluoroscopy is done in standing, lying and bending positions. Using this method, you can diagnose gastroesophageal reflux, paraesophageal hernia, polyps, diverticula, and ulcers.
- Esophagoscopy. An endoscopic procedure is performed on an empty stomach using a fibroesophagoscope in a specially equipped room. A targeted biopsy is performed and foreign objects are removed. Anesthesia is first used, and the patient is placed on a special table. Using the device, the mucous membrane is examined for inflammation and erosion. The size and position of the affected area are noted, and a piece of tissue is cut off from it (a biopsy is performed). Next, the resulting material is examined using a microscope, describing individual cells. This method allows you to establish obstruction of the esophagus in any area or non-opening of the sphincters. If there are scars on the walls of the organ, the lumen of the esophageal tube must be expanded using rigid or flexible rods. Esophagoscopy helps to establish the causes of dysphagia, diagnose tumors, and detect foreign bodies in the cavity.
- Esophageal pH-metry. A pH probe is used to record the acid-base balance at the bottom of the tube. Since values can fluctuate during the day, the study is carried out throughout the day. The results are processed using a computer. The nature of gastroesophageal reflux is revealed. It can be acidic (gastric), alkaline (pancreatic) or bile. The duration of this phenomenon is recorded.
- Computed tomography. Used to diagnose tumor diseases. At the same time, the condition of nearby organs, blood and lymphatic vessels is noted.
- Functional X-ray diagnostics. It is used for negative changes in the motility of the muscles of the esophageal tube, increased or decreased tone of the sphincters.
- Esophagotonocymography, esophagomanometry. Complex research methods using probes. By measuring the pressure in its different parts and in the area of the sphincters, areas with impaired tone are found. Indicators at rest and during swallowing are recorded.
- Functional testing for the diagnosis of gastroesophageal reflux. Includes Stepenko test, Baker and Bernstein acid test, reflux acid test. The stomach is probed using methylene blue dye.
- Radioisotope research. The 32P isotope helps to diagnose malignant tumors of the esophagus.
Anatomical and physiological narrowings of the esophagus
https://www.youtube.com/watch?v=https:accounts.google.comServiceLogin
Constrictions are areas of the smallest diameter; they differ in anatomical and physiological. There are 5 natural constrictions in total. These are high-risk areas, since this is where obstruction occurs when a foreign object enters or food accumulation occurs during dysphagia (a functional disorder of the passage of food).
Anatomical narrowings are determined both in the body of a living person and during a pathological examination. There are 3 such areas:
- cervical region at the lower edge of the pharynx;
- in the thoracic segment – the place of contact with the left bronchial tree;
- transition to the distal section when crossing the diaphragmatic window.
Physiological narrowing of the esophagus is caused by the spastic action of muscle fibers. These areas can only be detected during a person’s lifetime; these are the aortic and cardiac segments
Nervous system
The innervation of the esophagus occurs due to the vagus nerves and the trunks of the sympathetic nerves bordering them. The neurons of these nerves are located in the motor nuclei of the brain stem. Efferent fibers transmitting nerve impulses form plexuses that penetrate the wall of the organ. The straight and circular muscle layers form a plexus with neurons that have a specific autonomous function; a short neural arc can close at their level.
The cervical and thoracic sections of the organ supply branches with nerves that ensure their connection with the central nervous system, which form strong plexuses, which in turn stimulate the heart and trachea. In the thoracic section of the organ, in its middle part, in the nerve plexuses there are incoming branches of the sympathetic trunk and splanchnic nerves. In the lower part of the thoracic region, the plexuses again form trunks.
In the part of the esophagus above the diaphragm, the vagal trunks are closely adjacent to the walls of the esophagus and branch in a spiral state. The left trunk goes to the anterior surface of the stomach, the right – to the back. Centripetal nerve fibers from the esophagus enter the spinal cord.
Part of the organ’s autonomic nervous system, which is connected to the sympathetic system, but is functionally opposed to it, helps reflexively regulate the motor function of the esophagus. The mucous membrane of the organ is sensitive to heat, light, pain and tactile effects. The areas of the pharyngeal-esophageal and esophageal-gastric boundaries are particularly sensitive.
Anatomical feature
The anatomy of the esophagus, along with its structure and functional development, has a number of features that affect its proper functioning. We will talk about the blood supply to the esophagus, which is carried out in the cervical region from the lower thyroid arteries, in the thoracic region - through its own arteries.
The lymphatic system of the esophagus is a network of capillaries and vessels that dot all layers of the wall of the esophagus. A feature of the blood supply system is the collector vessels located along the entire path of the esophagus. They connect all lymphatic networks in all layers. An important aspect is the lymphatic topography of the esophagus, which demonstrates the direction of vessels from the cervical region to the deep cervical lower lymph nodes. Bypassing nearby nodes, it flows into the thoracic lymphatic duct.