Despite the fact that diabetes mellitus is one of the most common chronic diseases on the planet, medical science still does not have clear data on the causes of the development of this disease. Moreover, in each specific case of diagnosing diabetes, doctors never say exactly what caused it. Your doctor will never tell you what exactly caused your diabetes; he can only guess. Let's look at the main causes of diabetes mellitus known to modern medicine.
What is type 1 diabetes?
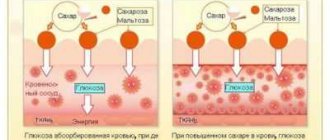
Type 1 diabetes (insulin-dependent diabetes, juvenile diabetes, T1DM) is a lifelong autoimmune disease that affects how the body processes food and turns it into energy. When we eat, food is digested and broken down into a simple sugar called glucose. Glucose is essential for all body functions, including thinking. But when a person has type 1 diabetes, the pancreas stops producing insulin, the hormone that allows the body's cells to take in glucose and convert it into energy.
In most people with T1D, the body's immune system, which normally fights infection, attacks and destroys the cells in the pancreas that produce insulin. Without insulin, glucose cannot enter cells and blood glucose levels rise. People with the disease must take insulin daily to stay alive.
Although anyone can get T1D, children and teenagers are most often diagnosed with this type of diabetes. It is estimated that out of 100 thousand, about 200 people in Russia are diagnosed with T1DM every year.
Types of analyzes and tests
I. Methods for studying metabolic processes (for metabolic disorders)
This group includes all types of tests and analyzes for glucose tolerance and determination of the level of glycosylated hemoglobin. They seem to confront a person with a fact, therefore, for the most part, they cannot be the only correct way of diagnosing. It is important to apply the second type of technique to them - screening for genetic predisposition (plus the presence of markers of autoimmune disorders that provoke type 1 diabetes)
Glycosylated or glycated hemoglobin (HbA1c)
Analysis of glycated hemoglobin is a very important component in making a diagnosis. It doesn’t really matter how you take it, on an empty stomach or not. It does not depend on the time of day and how the blood was taken: from a finger or from a vein (it all depends on the hemoglobin analyzers used).
Moreover, due to the fact that it shows the average percentage of glucose and iron-containing protein in the blood plasma (this protein is glycolyzed, i.e., has come into contact with excess glycemia, i.e., sugar) for approximately 60 - 90 days , then even colds, stress, poor nutrition will not be able to influence the final result. Even if the patient deliberately wants to tone down the final result and start eating right in a few days or weeks (without abusing carbohydrate-containing foods), this will have little effect on the accuracy of the result.
Normal glycated hemoglobin content (HbA1c)
| The norm for a healthy person | <5.7% |
| Satisfactory (can prescribe preventive methods to reduce HbA1c levels) | 5.7 — 6.0% |
| Increased risk (prevention required) | 6.1 — 6.4% |
| Diabetes | >6.5% |
Diabetics should strive to lower the HbA1c level below 7.0%, this is a specific prevention of the development of complications in diabetes.
The ideal value is the interval between 4.2 - 4.6% of the content of glycosylated hemoglobin in the blood plasma, which corresponds to an average glucose level of 4.0 - 4.8 mmol / liter.
Typically, people with these values have normal weight, a thin, lean build and lead an active lifestyle (for example, they go to the gym 2 - 3 times a week and spend at least 1.5 - 2 hours a day training).
However, this type of test is completely unsuitable for pregnant women, because in their special situation, predicting the results will only be shown at 7 or 8 months of pregnancy, i.e. actually before giving birth. This happens due to the fact that the test reflects the hemoglobin level over the 3 months preceding the analysis, and blood sampling must be done at the 4th or 5th month of actual pregnancy. Predicting future processes or changes in both the mother and the fetus and their further prevention or relief will be impossible, because they may already have started. Once the results are received, it will be too late to change anything. If blood is taken early (before or in the first months of pregnancy), the results will be unreliable, because in the process of bearing a child, a lot of qualitative changes occur in the mother’s body aimed at depleting all maternal reserves (that’s why all pregnant women are prescribed a serious vitamin complex).
Simply put, a pregnant woman carrying a child is like a universe in which the process of the birth of a new universe with numerous small young galaxies is maturing and accelerating.
Therefore, to draw some parallels, patterns before the beginning of the universe, and even more so to predict something, is a completely meaningless, insignificant and empty exercise. At this stage of its inception, it is important to conduct one-time quick tests that would show an express result.
These include a two-hour glucose tolerance test.
Glucose tolerance test
This test is popularly called a “sugar load”. It is carried out in several stages and lasts for several hours, but, unfortunately, this type of analysis is very capricious. Any little thing can affect the final results.
For example, the fasting period should be from 8 to 12 hours. Before donating blood, you should not eat, drink coffee or any other drinks, including alcohol. If a person has a cold, has a runny nose, has recently been ill or is still not recovered, had surgery a few weeks ago, is taking some medications, etc., then this will also affect the result. On the eve of the test, you should not go to the gym and it is advisable not to be too nervous or worried, and not to smoke. This test should also not be taken by women during menstruation.
It is carried out in several stages:
I. Blood sampling from a vein in the morning on an empty stomach.
II. A “glucose load” is produced.
You are supposed to drink sweetened water in which 75 grams of sugar is dissolved. Pregnant women are encouraged to drink sweetened water in which 100g is dissolved. glucose, because when carrying a child, energy consumption is slightly increased. For children, a solution is prepared at the rate of 1.75 g per kg of body weight, but not exceeding the dosage intended for adults.
All people suffering from asthma, who have angina pectoris or have had a stroke or heart attack, instead of a glucose solution, are offered a different load: it is recommended to consume simple carbohydrates (dosage - 20 g).
III. Several more blood samples will be taken over the course of 60 minutes to monitor blood glucose fluctuations.
All the steps described above must be repeated, because only a comparison of the data obtained will make it possible to compose a more accurate forecast. Usually the patient is invited to retake the test a few days later. This is done in order to refute or confirm the diagnosis.
The norm for a glucose tolerance test after receiving the results
| Norm mmol/l | 1 blood draw | <5.5 |
| In 2 hours | <7.8 | |
| Prediabetes mmol/l | 1 blood draw | 5.5- 6.7 |
| In 2 hours | 11.0 | |
| Diabetes mmol/l | 1 blood draw | >6.7 |
| In 2 hours | ≥11.1 |
II. Methods for studying genetic predisposition
PCR restriction analysis
These types of tests can detect type 1 diabetes at its early stage. More precisely, it does not even identify the disease as such, but allows one to calculate the risk of developing the disease in a particular person.
As a rule, special emphasis is placed on gene typing (HLA group II typing - human leukocytes), which identifies specific “mutations” of genes on the sixth chromosome, which is responsible for the human immune system. The protein encoded by the HLA genes is responsible for one of the most important functions in type 1 diabetes - it is involved in the recognition of foreign viruses, bacteria and other “invaders”, and helps create a specific logical chain in the immune response. Any mutations lead to a failure in the body’s protective functions.
The typing process takes place in several stages, during which genetic predisposition testing is carried out, when the patient is tested for the presence or absence of genes associated with type 1 diabetes. If your parents have diabetes or their immediate family members have diabetes, the risk of diabetes is very high. The test will allow you to understand how high this risk is.
For the test, about 2-3 ml of whole blood is taken and a PCR restriction analysis is performed. As a rule, you have to wait quite a long time for results. Within a month.
Prediction by antigenic markers
Antigens that can be found in a person’s blood during testing also play an important role in predicting diabetes.
Conducted tests to search for antigens to:
- cells of the islets of Langerhans (to β-cells of the pancreas)
- tyrosine phosphatase
- insulin
- glutamic acid decorboxylase
allow you to keep marked results. If autoantibodies to pancreatic cells, to insulin and to glutamic acid decorboxylase are detected, the risk of developing diabetes increases by 50% and can develop within 5 years. With a longer-term forecast (10 years in advance), the risk increases to 80%.
Thus, diagnosing type 1 diabetes mellitus comes down to predicting the development of this type of disease in the early stages and starting preventive actions in time in order to increase life expectancy without “sugar disease,” which can manifest itself at the most unexpected moment. At the same time, the first two types of tests (from the metabolic group) are more suitable for diagnosing type 2 diabetes, and in insulin-dependent diabetes they are used only as confirmation of the presence of the disease after it has already manifested itself.
But few people pay attention to such “little things” (the symptoms are mild), and they obviously won’t take expensive tests, because the rapidity of development of type 1 diabetes is actually a far-fetched opinion. This type of diabetes can be prevented in advance, because its predisposition is imprinted at the genetic level, and the incubation period lasts for 5 - 15 years or even longer.
Symptoms of type 1 diabetes
Since glucose cannot enter the body's cells and instead accumulates in the blood, it puts the body into crisis. The most common symptoms associated with the disease are:
- extreme fatigue;
- frequent urination;
- constant thirst, despite drinking fluids;
- strong urge to hunger;
- unexplained weight loss.
Symptoms of type 1 diabetes in children
The disease was formerly called juvenile diabetes because the disease often affects children and teenagers. Symptoms of the disease in children often look like this:
- frequent bedwetting;
- weight loss;
- severe hunger;
- frequent thirst;
- fatigue or mood changes.
These signs and symptoms can be easily noticed when you realize that the body is experiencing a lack of glucose in the body. Hunger, weight loss and fatigue are symptoms of the body's inability to use glucose for energy. Frequent urination and thirst occur because the body does its best to get rid of excess glucose by dumping it into the bladder.
Differentiation
Differential diagnosis of diabetes mellitus involves laboratory tests and medical history. In addition to making the correct diagnosis, it is also necessary to determine its form. Diff. Diagnosis is carried out with the following pathological conditions described in the table.
| Disease | Definition | Clinical manifestations |
| Diabetes insipidus | Pathology of the hypothalamic-pituitary system, characterized by insufficiency of the hormone vasopressin | Excessive urination, thirst, nausea, vomiting, dry skin, dehydration |
| Steroid diabetes | The disease occurs as a result of pathology of the adrenal glands or after long-term use of hormonal drugs | Copious urination, moderate thirst, weakness, fatigue. Symptoms are mild |
| Renal glycosuria | The presence of glucose in the urine when its levels are normal in the blood. Occurs against the background of chronic kidney disease | Weakness, constant fatigue, the skin becomes dry and acquires a yellow tint. Constant itching of the skin |
| Nutritional glycosuria | The presence of sugar in the urine after significant consumption of carbohydrates in foods and drinks | Frequent urination, feeling thirsty, weakness, decreased performance, drowsiness |
Important! The diagnosis is substantiated by an endocrinologist after receiving the examination results. Laboratory doctors do not interpret test results.
Type 1 and type 2 diabetes: what's the difference?
The biggest difference between these two types of diabetes (and there are more) is found in the production of insulin. In type 1, insulin production decreases and may stop altogether. In type 2 diabetes, the pancreas continues to produce insulin, but not enough to maintain glucose balance. It is also possible that the pancreas produces enough insulin but the body does not use it well (called insulin resistance), most often because the person is overweight (or obese). The vast majority of those diagnosed with diabetes have type 2 (accounting for 95% of diabetes cases in adults).
Clinical picture of type 2 diabetes
Type 2 diabetes usually develops in people over 40 years of age who are overweight, and its symptoms increase gradually. The patient may not feel or pay attention to the deterioration of his health for a long time, up to 10 years. If diabetes is not diagnosed and treated all this time, vascular complications develop. Patients predominantly complain of weakness, decreased short-term memory, and fatigue. All these symptoms are usually attributed to age-related problems, and the detection of high blood sugar occurs by chance. Regular scheduled dispensary examinations of employees of enterprises and government agencies help to diagnose type 2 diabetes in a timely manner.
Almost all patients diagnosed with type 2 diabetes have risk factors:
- the presence of this disease in close relatives;
- family tendency to obesity;
- in women - the birth of a child weighing more than 4 kg, there was increased sugar during pregnancy.
Specific symptoms associated with type 2 diabetes are thirst up to 3-5 liters per day, frequent urge to urinate at night, and wounds that do not heal well. Also skin problems - itching, fungal infections. Typically, patients pay attention to these problems only when they have already lost 50% of the functional mass of beta cells of the pancreas, i.e., diabetes is severely advanced. 20-30% of people with type 2 diabetes are diagnosed only when they are hospitalized for a heart attack, stroke or vision loss.
Causes of type 1 diabetes
Type 1 diabetes is caused by an autoimmune reaction (the body attacks itself by mistake) that destroys insulin-producing cells in the pancreas, called beta cells. This process may continue for months or years before any symptoms appear.
Some people have certain genes (traits passed from parent to child) that make them more likely to develop type 1 diabetes, although many will not have T1D even if they have the genes. Exposure to environmental triggers, such as viruses, is also thought to play a role in the development of type 1 diabetes.
Causes
Type 1 diabetes is caused by the body's immune system attacking and destroying the beta cells in the pancreas. These are special cells that produce the hormone insulin, which helps digest food and lower blood glucose levels. After 80-90% of beta cells die, insulin begins to be severely lacking, sugar levels rise significantly and symptoms of the disease appear. Why does the immune system decide to attack beta cells? Because the patient’s body is genetically predisposed to this. There must also be some events that trigger the process. Blood glucose levels often begin to rise after a viral infection, such as rubella.
Unfortunately, vaccination against viruses does not currently help reduce the risk of this disease. It is possible that the incidence of autoimmune diabetes is increased among children who received cow's milk-based formula as infants.
The website Endocrin-Patient.Com promotes the methods developed by Dr. Bernstein to control impaired glucose metabolism. These methods contradict official instructions, but really help. Watch this video as Dr. Bernstein explains when and how type 1 diabetes will be finally solved.
https://youtu.be/gxQQ2MOi4Jg
Did you like the video? You can find even more interesting things on our Youtube channel. It is also useful to subscribe to news on VKontakte and Facebook.
No environmental factors have been proven to influence the risk of type 1 diabetes. Scientists do not yet know why the incidence of this disease is much higher in some countries than in others. With age, the risk of autoimmune attacks on beta cells decreases significantly. The older a person is, the less likely he is to develop this disease and the easier it will be if it does happen.
Is bad genetics really the main cause of type 1 diabetes? Many people are carriers of unfavorable genetic mutations. However, few of them have the misfortune of falling ill during their lifetime. It appears that environmental conditions and lifestyle play a big role.
The worst thing is if a child has both parents with type 1 diabetes. If only one of the parents, the risk for the child is not very great. If the mother has autoimmune diabetes, the risk for the child is only 1-1.5%, for the father - 5-6%, for both parents - about 30%.
How quickly does type 1 diabetes develop?
In children, it takes several months from the onset of the immune system to attack the beta cells of the pancreas until the first symptoms appear. In adults, this disease takes much longer to develop. It can occur without symptoms for about 10 years. If you accidentally check your blood sugar, it will be moderately elevated. The number of beta cells in the human body is much greater than necessary. Even after 50-70% of them die, the remaining ones more or less satisfy the need for insulin. Therefore, type 1 diabetes develops slowly in all categories of patients except infants.
What is the difference between type 1 and type 2 diabetes?
In type 1 diabetes, the patient does not have enough insulin in the body. In type 2 diabetes, there may be enough or even too much insulin, but the tissues become less sensitive to it. Type 1 diabetes begins when the beta cells in the pancreas that produce insulin die due to an attack by the immune system. In patients with type 2 diabetes, these cells do not turn off immediately, but only at a late, severe stage of the disease. The main cause of their death is considered to be overload.
Although it should be noted that with type 2 diabetes, autoimmune attacks also occur. Type 1 diabetes cannot be prevented and cannot be avoided. Type 2 diabetes is not very difficult to treat and is 100% preventable through a healthy lifestyle, even if there is a genetic predisposition.
Read about the prevention and treatment of complications:
Eyes (retinopathy) Kidneys (nephropathy) Diabetic foot Pain: legs, joints, head
Complications
If a person does not control the symptoms of the disease, a number of dangerous complications can develop.
These include:
- Diabetic retinopathy : Excess glucose causes the walls of the retina, the part of the eye that detects light and color, to weaken. As retinopathy progresses, small blood vessels can form behind the eyes, which can bulge and rupture, causing vision problems. T1DM is one of the leading causes of blindness among adults of working age.
- Diabetic neuropathy : High blood sugar reduces circulation, damaging nerves in the arms and legs and leading to loss of sensation or abnormal sensations such as burning, tingling and pain. Because diabetes can also reduce the body's ability to heal, minor cuts and injuries can lead to more permanent damage, especially because a person may not notice them right away.
- Diabetic nephropathy or diabetic kidney disease: The kidneys filter glucose from the blood. Too much glucose can overwork them and gradually cause kidney failure, which can progress to the need for dialysis.
- Cardiovascular diseases . Diabetes can lead to a number of conditions that impair the functioning of the heart and arteries, including heart attack, stroke and peripheral vascular disease. As a result of poor circulation, the disease can also increase the risk of amputations.
- Gum disease : T1D can increase the risk of gum disease and tooth loss, meaning a person with this type must be very careful to maintain healthy teeth.
- Depression : Diabetes has strong links with depression.
- Diabetic ketoacidosis is an acute complication of T1DM that occurs when a person does not meet insulin needs and the body is under extreme stress. Diabetic ketoacidosis results in very high blood sugar levels. The body experiences a shift in metabolism and begins to break down fat instead of sugar, producing ketones as a waste product. Ketones can be harmful to the body and cause acidosis. Ketoacidosis is a medical emergency that requires hospitalization and treatment with intravenous insulin.
Complications and their prevention
Complications of impaired glucose metabolism are divided into acute and chronic (late). Patients with type 1 diabetes are most afraid of problems with their kidneys, eyesight and legs. This disease negatively affects almost all body systems, except, perhaps, the hair on the head. Read the detailed article “Complications of diabetes.” The threat of severe complications should give you the motivation to follow the regimen carefully and control your blood sugar.
Acute complications occur if glucose levels drop significantly or remain very high for a long time. Read the articles “Low blood sugar (hypoglycemia)” and “Diabetic ketoacidosis” for more information. Learn about prevention methods. Understand how to provide emergency care to a patient.
Achieving a consistently normal sugar level of 4.0-5.5 mmol/l, as in healthy people, helps block the development of complications of impaired carbohydrate metabolism. It even reverses some of them. Official medicine does not encourage achieving normal glucose levels. This is thought to require the use of high doses of insulin, creating a greater risk of hypoglycemia. In fact, switching to a low-carb diet reduces insulin dosages by 2-8 times, stops spikes in blood sugar and allows it to stabilize at the desired level.
https://youtu.be/u3OL01zrFrI
A method of treating type 1 diabetes based on a low-carbohydrate diet has convincingly proven its effectiveness in preventing complications. Damage to the nervous system, called diabetic neuropathy, is reversible. In diabetics who keep their sugar consistently normal, the nerve fibers gradually heal. In particular, sensitivity in the legs is restored. Moderate to moderate vision and kidney complications can also be reversed.
How can you predict the life expectancy of a patient?
The life expectancy of a person with type 1 diabetes depends most on his motivation. As they say, if the patient truly wants to live, then medicine is powerless... Dr. Bernstein fell ill at the age of 12, more than 30 years before the invention of home glucometers. He had many serious complications. Tests even showed a high content of protein in the urine, which is a harbinger of imminent death due to kidney failure. However, with the help of a low-carb diet, precise insulin dosing and other tricks, he managed to live to 83 years old, maintaining good physical shape and a sound mind.
At the time of writing this article, Dr. Bernstein is alive and well, working for many hours every day with patients, lifting weights in the gym and has no plans to stop. He even regained kidney function thanks to consistently normal blood sugar. However, it takes a lot of motivation to stick to the routine every day. Life expectancy is low for diabetics who are blind, undergo dialysis, have severe leg problems, or have had an amputation.
Diagnostics
There are three standard blood tests that are commonly used to diagnose type 1 and type 2 diabetes. A person may be diagnosed with type 1 diabetes if they meet one of the following criteria:
- Your fasting blood glucose level is greater than 126 milligrams per deciliter (mg/dL) in two separate tests.
- Random glucose test greater than 200 milligrams per deciliter (mg/dL) with symptoms of diabetes.
- Hemoglobin a1C test exceeds 6.5 percent in two separate tests.
When diagnosing T1DM, two other factors are taken into account: the presence of specific antibodies, such as antibody to glutamic acid decarboxylase 65 (Anti-GAD65) and/or others; and low levels of C-peptide, a substance produced by the pancreas along with insulin that can indicate how much insulin the body is making.
Differential diagnosis
The blood test is performed in the morning on an empty stomach. Particular attention is paid to carbohydrate load indicators. Regulating the amount of glucose is done using a glucometer or in a laboratory setting. Endocrinologists often study the composition of urine and determine the amount of sugar. Healthy people should not have glucose in their urine. For a detailed assessment, an acetone test is performed. An increase in the amount of metabolites of this substance in biological fluids indicates a complex form of the disease.
Treatment of type 1 diabetes
The goal of treating type 1 diabetes is to prolong insulin production for as long as possible before production stops completely, which is usually inevitable. It is a lifelong condition, but there are many treatments and medications that can help control it.
Initially, changes in diet and lifestyle may help with blood sugar balance, but as insulin production slows, an insulin injection may be needed. The timing of insulin therapy is different for each person.
If you have type 1 diabetes, you will eventually need to take insulin shots (or wear an insulin pump) every day to control your blood sugar and get the energy your body needs. Insulin should not be taken as a pill because the acid in the stomach will destroy it before it enters the bloodstream. Your doctor will help you determine the most effective type and dosage of insulin for you.
Some people who have difficulty achieving normal blood glucose levels with insulin alone may also need to take another type of diabetes medication that works with insulin, such as pramlintide ( Symlin ). Pramlintide, given by injection, helps normalize blood glucose levels when they rise after meals.
What is diabetes mellitus?
Diabetes is a complex group of diseases caused by various causes.
People with diabetes tend to have high blood sugar levels (hyperglycemia). In diabetes, metabolism is impaired - the body's conversion of incoming food into energy.
Food that enters the digestive tract is broken down into glucose, a form of sugar that enters the bloodstream. With the help of the hormone insulin, the body's cells are able to receive glucose and use it for energy.
Diabetes mellitus develops when:
- the body does not produce enough insulin;
- body cells are unable to effectively use insulin;
- in both of the above cases.
Insulin is produced in the pancreas, an organ located behind the stomach. The pancreas is made up of a collection of endocrine cells called islets. Beta cells in the islets produce insulin and release it into the blood.
If the beta cells do not produce enough insulin or the body does not respond to the insulin that is present in the body, glucose begins to accumulate in the body rather than being absorbed by the cells, leading to prediabetes or diabetes.
Causes of type 1 diabetes in children
Prediabetes is a condition in which the blood glucose level or glycosylated hemoglobin HB A1C level (the average blood sugar level over recent months) is higher than normal, but not yet high enough to be diagnosed with diabetes. With diabetes, the body's cells experience energy starvation, despite high blood sugar levels.
Over time, high blood glucose levels damage nerves and blood vessels, leading to complications such as heart disease, stroke, kidney disease, blindness, dental disease and lower limb amputation. Other complications of diabetes may include increased susceptibility to other diseases, loss of mobility as you age, depression, and problems with pregnancy.
No one is sure what triggers the processes that cause diabetes, but scientists believe that most diabetes is caused by an interaction of genetic and environmental factors.
There are 2 main types of diabetes – type 1 diabetes and type 2 diabetes. The third type, gestational diabetes, develops only during pregnancy. Other types of diabetes are caused by defects in specific genes, diseases of the pancreas, certain medications or chemicals, infections, and other factors. Some people show signs of both type 1 and type 2 diabetes at the same time.
Life forecast
People with type 1 diabetes usually adapt quickly to the time and attention it takes to monitor their blood sugar levels, manage the disease, and maintain a normal lifestyle.
Over time, the risk of complications increases. However, the risks can be significantly reduced if blood glucose levels are closely monitored.
The average life expectancy of patients with type 1 diabetes today is about 60 years.
Patients with type 1 diabetes mellitus (DM) require lifelong insulin therapy. Most require 2 or more insulin injections per day, with doses adjusted based on self-monitoring of blood glucose levels. Long-term management requires a multidisciplinary approach that includes physicians, nurses, nutritionists, and individual specialists.
Treatment
After confirming the diagnosis, many patients are interested in the question: can type 1 diabetes be cured? It is not completely curable, but it is possible to improve the patient’s condition for many years with the help of the following therapeutic measures:
- insulin replacement therapy - the dosage of such a substance is selected individually depending on the severity of the course and the age category of the patient;
- a gentle diet;
- a specially designed physical activity regimen - in general, patients are advised to perform light or moderate exercise for at least an hour every day.
Controlling type 1 diabetes
A diet for type 1 diabetes requires adherence to the following rules:
- complete exclusion of products such as sugar and honey, homemade jam and any confectionery, as well as carbonated drinks;
- It is recommended to enrich the menu with bread and cereals, potatoes and fresh fruits;
- frequent and fractional food consumption;
- limiting the intake of animal fats;
- control over the consumption of grain crops and dairy products;
- avoiding overeating.
A complete list of permitted and prohibited ingredients, as well as other nutritional recommendations, can only be provided by the attending physician.
In addition, treatment of diabetes mellitus in children and adults is aimed at informing the patient and his relatives about the principle of using insulin and providing first aid in the development of comatose states.
Patients need to take into account that pathology can only be treated using traditional methods, and the use of folk remedies can only worsen the condition.
Insulin administration
Insulin is injected under the skin; you need to massage the injection site well in advance. The injection sites should be changed daily. Insulin is administered using an insulin syringe or a pen. A pen syringe is the most practical option; it is equipped with a specialized needle that ensures a virtually painless injection procedure. You can carry it with you, and the insulin in the syringe pen is not destroyed by the environment or temperature changes.
You should consume food no later than 30 minutes after the injection. The most commonly used administration regimen is:
- In the morning, before breakfast, short- and long-acting insulin is administered;
- Before lunch - short exposure;
- Before dinner - short exposure;
- At night - long-lasting.
Glucose tolerance test
The technique makes it possible to accurately diagnose the form of diabetes and identify hidden metabolic disorders. Diagnosis is carried out after waking up on an empty stomach. You should not eat food 10 hours before tests.
Limitation:
- Do not subject your body to serious physical stress,
- consumption of alcohol and cigarettes is prohibited,
- You should not eat foods that increase the amount of sugar.
Physical activity
Any load is accompanied by a decrease in glycemia. This occurs due to the absorption of glucose by working muscle cells and increased sensitivity to injected insulin. It is important to accurately calculate the required dose of the drug depending on the planned activity and not to conduct long or overly intense training.
A daily 20-30 minute workout improves the course of type 1 diabetes. This is explained:
- reducing the required dose of insulin;
- normalization of the absorption of carbohydrates and fats;
- improvement of systemic circulation and microcirculation in tissues;
- activation of the fibrinolysis system - the blood becomes more liquid, fluid, the formation of blood clots that block the blood flow is inhibited;
- in response to stress factors, less adrenaline and other hormones that interfere with the action of insulin are released.
Watch the video about gymnastics for diabetes:
https://youtu.be/RGfzidGt0Bg
As a result, not only does the risk of vascular disease (diabetic angiopathy) decrease, but with regular exercise it is even possible to achieve a noticeable improvement in blood circulation and overall endurance of the body.
Complications of insulin therapy
In rare cases, the following conditions may occur:
- A hypoglycemic state is a sudden drop in blood sugar, observed with large amounts of insulin, excessive exercise, or insufficient food intake;
- Allergic reaction, itching, rashes in the area where the drug was administered - due to incorrect injection of insulin (thick, blunt syringe needle, cold insulin, incorrect injection site);
- Post-insulin lipid dystrophy (skin changes, disappearance of subcutaneous fat at the injection site) - incorrect injection placement - insufficient massaging, cold preparation, multiple injections in the same place.
New in diabetes therapy
The development of innovative methods takes place in several directions.
Methods of administering insulin
The traditional and most common method is still the injection method. It involves the use of a syringe or pen. This creates inconvenience for patients due to the need for repeated skin punctures and the mandatory maintenance of sterility during subcutaneous injection.
An alternative and more promising method is an insulin pump. It is a device that supplies insulin on command from the control system. Using the pump method, you can pre-program the administration mode, use fractional delivery and short or ultra-short insulin. The rhythm of hormone supply approaches the physiological one.
The new generation of pumps have become more compact, there are models without connecting tubes, and most importantly, they have additional functions:
- sugar measurement;
- glycemic monitoring;
- independent dose adjustment depending on changes in the amount of blood glucose.
Pump for patients with diabetes
Presumably, a portable device may appear that has all the functions of the pancreas. This means that he will not need the patient’s participation in the regulation of glycemia, which is what happens in a healthy body.
The second direction is to search for the possibility of administering insulin in inhalations or tablets. The final stage of testing ultra-short insulin using Technosphere technology for aerosol injection into the nose is underway. An insulin patch has also been invented, which consists of microreservoirs with the hormone, equipped with extremely small needles.
Insulin patch
The introduction of extended- and extra-long-acting drugs to the market continues, which will help reduce the frequency of injections.
Insulins that:
- begin to act faster than natural;
- have a low ability to cause allergies;
- do not have a long-term mitogenic effect (do not stimulate cell growth and division with long-term administration).
Watch the video about the treatment of type 1 diabetes:
https://youtu.be/7FbwUmvACqw
Pancreas transplant
In the world, only about 200 operations have been performed to transplant both the entire organ and its parts, the complex with the duodenum, kidney, and liver. Their effectiveness remains extremely low due to the poor survival rate of the pancreas and the need for intensive drug therapy that suppresses the immune system and the rejection reaction.
A new direction has emerged in this area. It is proposed to use stem cells and reprogram them to produce insulin. American scientists isolated the nucleus of a skin cell and transplanted it into a fertilized, nuclear-free egg.
As a result, a clone of pluripotent stem cells was obtained. This means that they can be developed into mature ones with any functions. For a thirty-year-old patient, islet B cells were synthesized in sufficient quantities and then injected into the pancreatic tissue.
Insulin dose calculation
The doctor selects the dose individually, focusing on the following criteria:
- Long-acting insulin. Before administration, glucose is measured; 2-3 hours after injection, sugar should remain at the same level (this indicates the correct dosage). It is important to control the dose over several days: on the first day, breakfast is postponed - sugar levels are measured every 1-2 hours, on the second day - lunch is postponed, measurements are taken with the same frequency. The third day - dinner is postponed, the fourth - measurements at night. If sugar fluctuates by 1–2 mmol/l, this is considered normal and the correct dose.
- Short-acting insulin. It is administered over 30 minutes. Before consuming food, when selecting a dose, you need to eat foods containing a low glycemic index. To calculate the dosage, measure sugar before eating, then inject insulin, consume food, then measure sugar 1.5–2 hours later and 3–4 hours after eating. Sugar 2-3 hours after consuming food should be 2-3 mmol/l higher than before eating; if it is lower than these values, there is an overdose of insulin; if higher, there is a deficiency. 3-4 hours after eating, your sugar level should be the same as before eating.
It is important to consider that insulin dosage may change up or down during illness, stress, menstruation, changes in physical activity and other changes.
Research methods
Diagnosis of the disease includes clinical and laboratory tests. In the first case, the doctor collects an anamnesis of the pathology - examines the patient, determines his height and weight, and hereditary predisposition to the problem. The study is continued if the patient has 2 or more signs of the disease.
When making a diagnosis, risk factors are taken into account:
- age over 40 years;
- excess body weight;
- lack of physical activity;
- disturbance of carbohydrate metabolism in women during pregnancy and after childbirth;
- polycystic ovary syndrome in the fair sex;
- constant increase in blood pressure.
People over 40 years of age should regularly check their sugar levels (once every 3 years). Persons at risk for diabetes are required to undergo examination once a year.
Some tests or screenings can help diagnose type 2 diabetes. Such a study makes it possible to identify pathology in the early stages of development, when the disease is not accompanied by characteristic symptoms.
A reliable way to diagnose pathology is to identify the indicator of glycosylated hemoglobin. The degree of deviation of the indicator from the norm depends on the concentration of sugar in the blood.
Basic diagnostic methods
Diagnosis of diabetes mellitus includes basic and additional methods. The first group of studies includes:
Pressure in diabetes mellitus - diagnosis, treatment
- Blood test to determine sugar levels.
- Glucose tolerance test. Before the examination, the patient drinks a cocktail and donates blood from a finger prick before and after it. The technique allows you to distinguish the disease from prediabetes.
- Urine analysis to detect sugar.
- Detection of ketones in the patient's blood or urine to determine complications of the disease or its acute development.
Additional research methods
Additionally, the following indicators are determined:
- Autoantibodies to insulin.
- Proinsulin - to study the possibility of pancreas functioning.
- Hormonal levels.
- C-peptide - to determine the rate of insulin absorption into cells.
- HLA typing – to identify possible hereditary pathologies.
Additional research methods are used to determine the most effective treatment tactics or in cases where diagnosing diabetes is difficult. The decision to prescribe additional tests is made by the doctor.
Types of insulin by degree of action
- Ultra-short insulin (fast-acting), begins to act immediately after administration, reaching maximum values after 1–1.5 hours. Effective for 3–4 hours.
- Short – begins to function after 20–30 minutes. after injection, reaches maximum values after 2–3 hours. Effective for 5–6 hours.
- Medium duration - exposure 2-3 hours after administration, maximum concentration after 6-8 hours. Effective for 12–16 hours.
- Prolonged (long-acting) - acts 4-6 hours after administration, accumulates in the body, peak action 2-3 days after injection.