Category: Neurology
Encephalitis is a terrible diagnosis associated with disability and a high risk to life. Most people have heard about tick-borne encephalitis, but the cause of the disease can be meningococcus, viruses, even syphilis and numerous vaccinations.
The severe course of general cerebral and focal symptoms, indicating the localization of the inflammatory process in the brain, often leaves incurable neurological consequences.
Classification
Since the formation of viral encephalitis is based on the entry of neurotropic pathogens into the brain tissue, experts adhere to the following classification of the disease:
By type of viral agent:
- Economo's encephalitis – infection by droplet-airborne means;
- tick-borne – occurs after the bite of an infected tick, as the primary carrier of the virus;
- Japanese – the source of danger will be birds, insects, as well as people themselves;
- influenza encephalitis of the brain - occurs against the background of an existing influenza infection;
- herpetic - the causative agent is the herpes virus.
Depending on the seasonality factor, encephalitis can be:
- seasonal - for example, tick-borne or Australian;
- multiseasonal – enterovirus, influenza;
- caused by an unknown type of virus - leukoencephalitis, a lethargic variant of encephalitis.
According to the localization of the pathological focus:
- in the white matter of the brain;
- with inflammation of the gray structures of the brain;
- panecephalitis - with diffuse involvement of cerebral elements.
By age criterion:
- encephalitis in children;
- brain damage in adults.
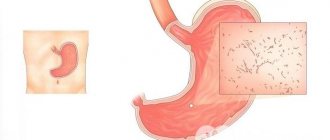
In order for encephalitis to form, the virus must penetrate directly into the membranes of the brain. It is after their inflammation that the characteristic symptoms of the disease appear. However, only a study of spinal cerebrospinal fluid can confirm the appearance of tick-borne encephalitis or its other form.
Encephalitis - what is it?
Encephalitis is an inflammation that develops directly in the brain. The disease is epidemic (seasonal outbreaks or epidemics in a limited area).
In addition to the acute form, encephalitis can be asymptomatic or flu-like. However, the absence of severe symptoms does not reduce the risk of developing severe complications. The disease occurs focally (inflammation of a limited part of the brain) or diffusely (spread).
Often, both encephalitis and meningitis (inflammatory damage to the meninges) are simultaneously diagnosed, which aggravates the course of the disease and worsens the prognosis even with timely therapy.
Causes of encephalitis:
- bacteria - meningococcus, Treponema pallidum, which causes syphilis;
- viruses - specific tick-borne encephalitis virus, herpes, measles, chickenpox and rubella viruses, the causative agent of Economo's disease - lethargic encephalitis;
- pathogenic microorganisms from different groups - toxoplasma, the causative agent of malaria, typhus and rabies;
- vaccination - DPT, anti-smallpox serum (especially if the vaccination regimen and rules for administering vaccines are not followed);
- autoimmune disorders - leukoencephalitis, rheumatic form of the disease;
- severe intoxication with chemicals, carbon monoxide.
Tick-borne encephalitis
Tick-borne viral encephalitis is especially common - infection occurs through the bite of an ixodid tick, which parasitizes birds and rodents.
Infection cannot be ruled out by consuming milk from livestock (cow, goat) infected with the virus. The infection enters the bloodstream already on day 2, but symptoms of the disease appear 2-3 weeks after the bite; when infected through food, the incubation period is reduced to 4-7 days.
Outbreaks of tick-borne encephalitis are recorded during the periods May–June and August–September. At the same time, the local population suffers encephalitis in an asymptomatic form in 90% of cases. In epidemically disadvantaged areas, the population is recommended to be vaccinated against tick-borne encephalitis.
Symptoms
The clinical picture of encephalitis in humans largely depends on the type of infectious agent and the characteristics of the course of the pathology. At the very beginning of inflammation of the brain substance, general infectious signs will be present - for example, severe malaise and weakness, as well as fever and disturbances in appetite and stool.
And only then do the symptoms of encephalitis appear directly, the main of which, of course, is intense pain in the head - diffuse in nature, difficult to respond to standard analgesics. Against the background of brain inflammation, people may experience varying degrees of consciousness disorders - from euphoria to lethargy and coma. In addition, nausea, convulsions, increased sensitivity to light, and uncontrollable vomiting are added.
A viral infection of the brain tissue cannot but affect the cranial nerves. Patients experience a sharp decrease in auditory and visual activity. In addition, neurological deficit certainly affects sensitive, olfactory perception - paresthesia, hallucinations, changes in appetite.
While impaired motor function is more often expressed by cerebellar syndrome - a swaying gait, sweeping movements, or severe muscle weakness and tremors in the fingers. For each form of encephalitis, the symptoms will have their own nuances of the course, so it seems difficult for specialists to identify any specific syndromes.
Symptoms
Encephalitis is a disease that is accompanied by a whole group of symptoms. They can be divided into:
- general inflammatory reactions of the body;
- cerebral symptoms;
- focal symptoms (indicating which part of the brain is affected).
Depending on the cause of encephalitis (infection, allergy or toxic effects), one or another group of symptoms may be more severe. For example, with encephalitis with a bacterial and viral onset, the general inflammatory reactions of the body will be more pronounced than with the allergic nature of the process, but the diagnosis of encephalitis is valid only if all three groups of symptoms are present.
General inflammatory reactions of the body
After the incubation period (the time from the moment the pathogen enters the body until the first symptoms appear), general weakness, malaise, a feeling of weakness and fatigue occur. Sleep and appetite are disturbed. Aches appear in the body and muscles, and there is a feeling of “twisting” in the joints. Body temperature rises to 38°C - 40°C. Manifestations of catarrh of the upper respiratory tract (mucous discharge from the nose, sore throat, coughing, etc.) or gastrointestinal disorders may occur, and a rash may appear on the body. All these symptoms are nonspecific (occur in other diseases) and depend on the type of pathogen. Not every encephalitis is accompanied by all of the listed symptoms.
General cerebral symptoms
This subgroup of symptoms includes:
- disturbance of consciousness;
- headache;
- dizziness;
- nausea and vomiting;
- increased sensitivity of the senses;
- generalized convulsive seizures;
- mental disorders.
Impaired consciousness can range from minor confusion (the patient is slightly inhibited and does not immediately answer questions) to coma. Moreover, a comatose state can develop almost at lightning speed.
Headache is an almost obligatory sign of encephalitis. It can be very diverse in nature (dull, sharp, aching, pulsating, shooting, drilling, and so on) and intensity, and tends to increase. Headache may be associated with intoxication of the body, or may be the result of impaired blood circulation and circulation of cerebrospinal fluid.
Dizziness also tends to get worse and may be accompanied by nausea and vomiting, the latter not always bringing relief and may recur several times.
The so-called hyperesthesia (increased sensitivity) of the sense organs is characteristic: fear of light and noise, perception of tactile touches as painful.
Generalized epileptic seizures may be one of the first signs of encephalitis. They appear as a result of irritation of brain tissue.
Mental disorders in encephalitis are acutely occurring and emotionally excessive manifestations. Usually these are delusions, hallucinations and even psychosis. The patient may suddenly develop psychomotor agitation, during which he has absolutely no control over his actions and behaves inappropriately. Just like other general cerebral symptoms, mental disorders can increase. A situation is possible when, after an attack of hallucinations or psychomotor agitation, the patient falls into a coma.
CM. SEE ALSO: Herpetic encephalitis: symptoms and treatment
Focal symptoms
Patients with encephalitis develop weakness in the limbs and sensory disturbances.
The inflammatory process can affect absolutely any part of the brain tissue, although some pathogens are characterized by “favorite” places of damage, but, in most cases, these places cannot be predicted. Depending on which part of the brain is involved, such symptoms will arise. It can be:
- paresis and paralysis: decreased muscle strength. Moreover, this may be a barely noticeable weakness during active movements (akin to fatigue), or maybe a complete lack of even the ability to move a limb. Weakness may increase gradually, or may immediately be quite pronounced;
- violation of muscle tone (both increasing and decreasing);
- Sensory impairment: loss of the sensation of touch or the difference between cold and hot, sharp and dull touch. This group also includes a kind of sensitivity disorder, when the patient cannot understand which part of the body the doctor is holding him by and in which direction he is making a passive movement (for example, with the patient’s eyes closed, the doctor touches the index finger of one of the hands and bends it in the direction of the palm , and the patient does not feel the touch or direction of movement at all or cannot correctly name the serial number of the finger and where it is bent);
- speech disorders: loss of the ability to understand or reproduce speech. However, it is not at all necessary that the loss of speech will be complete. Options are possible when the patient cannot pronounce individual words or sounds, confuses similar words and letters, does not understand the meaning of complex verbal constructions (for example, cannot correctly answer the question: “Glory is higher than Nikita. Who is the tallest?”);
- loss of ability to read, write and count;
- loss of the ability to recognize a familiar object by touch: astereognosis (for example, if you put a pen or a matchbox in your hand, then with your eyes closed the patient will not be able to determine what kind of object it is);
- imbalance and coordination disorders: unsteadiness when walking and standing, inability to hit a stationary object with a finger, missing when trying to pick up a spoon or glass;
- hearing loss, tinnitus;
- memory loss;
- loss of visual fields, sensation of looking “down the tube”;
- incorrect visual perception (for example, large objects appear small, loss of distinction between left and right sides, etc.);
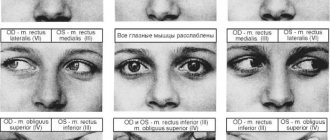
- violation of combined movements of the eyeballs (turns to the sides, up and down);
- the appearance of involuntary movements in the limbs and torso: twitching, shuddering, waving the arms, turning the body, nodding the head, grimacing, trembling of the arms and legs and similar movements;
- symptoms of parkinsonism;
- loss of control over urination and bowel movements;
- damage to the cranial nerves (the face looks distorted, strabismus, drooping eyelids, blurred vision, loss of taste, trigeminal neuralgia, impaired speech intelligibility, difficulty swallowing, nasal voice, choking and other symptoms occur);
- mental disorders: inappropriate behavior, foolishness, unmotivated aggression and others.
It should be understood that in each specific case, only one of the above listed symptoms, or maybe several, may be present. It all depends on the extent of the lesion.
Encephalitis of the brain may be accompanied by the development of meningeal syndrome.
CSF changes
Encephalitis is characterized by the appearance of inflammatory changes in the cerebrospinal fluid (CSF). It is obtained by performing a spinal tap. With encephalitis, the pressure of the cerebrospinal fluid increases, the content of cells (lymphocytes and/or neutrophils) increases, the protein content increases, in some cases an admixture of red blood cells may be detected (for example, with chickenpox encephalitis, influenza encephalitis), and a slight increase in sugar content is possible. Also, antibodies to the causative agent of encephalitis can be detected in the cerebrospinal fluid and the disease can be identified from them.
Encephalitis is a serious disease of the nervous system. In addition to general infectious, cerebral and focal symptoms, encephalitis is almost always accompanied by changes in blood pressure, disturbances in cardiac activity and breathing. A serious complication of encephalitis can be the development of cerebral edema with displacement of some of its parts, which can cause compression of the vital centers of breathing and heartbeat, and the latter can be fatal.
CM. SEE ALSO: Herpetic encephalitis: symptoms and treatment
Each type of encephalitis is characterized by certain features of its course (for example, measles encephalitis develops against the background of a specific rash). Knowledge of these features helps the doctor in diagnosis.
Diagnostics
The lack of a specific clinical picture of viral brain damage makes it difficult for specialists to differentiate it from bacterial encephalitis at the pre-laboratory stage.
As a rule, diagnosis in neurology of this pathology is based on anamnestic and epidemiological information - an outbreak of viral diseases, a person’s travel to countries where encephalitis is common. Additionally, diagnostic procedures are required:
- echo-encephalography – reveals hypertension of cerebrospinal fluid etiology;
- electroencephalography – shows diffuse changes in the electrical activity of the brain;
- ophthalmoscopy - the specialist observes significant deviations in the optic nerve head;
- lumbar puncture – lymphocytic pleocytosis;
- computed tomography/magnetic resonance imaging – the prevalence of inflammation in the brain, its localization.
However, as the practice of specialists proves, only PCR diagnostics of cerebrospinal fluid allows one to clarify the type of pathogen of the disease. Unfortunately, this method is not always informative - in some cases, virus verification remains an impossible task.
Diagnosis and treatment methods for encephalitis
To establish an accurate diagnosis, a blood test (general and biochemical) and a lumbar puncture are taken from the patient. Hardware studies are also carried out - computer () or magnetic resonance imaging (MRI), electroencephalograms (EEG) of the brain.
Serological reactions can also be carried out, the purpose of which is to detect specific antibodies in the blood. In order to properly treat a patient, it is extremely important to correctly determine the cause of the disease. After all, the type of medicine depends on the nature of encephalitis: some medicines “work” against viruses, and completely different ones against bacteria.
Treatment of encephalitis is carried out comprehensively. First of all, it is necessary to provide the patient with rest and bed or semi-bed rest. The best way to create such conditions is in a hospital, so the patient is usually treated in a hospital. Medical supervision is necessary, because in severe cases it is necessary to resort to emergency measures to support life functions, for example, connecting the patient to a ventilator.
Drugs used:
- Glucocorticosteroids (hormones) – Prednisolone, Hydrocortisone.
- Decongestants (diuretics) – Glycerol, Mannitol and others.
- Antihypoxants (to combat the lack of oxygen) - Actovegin, vitamin E, Mexidol.
- Antihistamines (antiallergic) - Suprastin, Tavegil, Loratadine.
- Antiviral (Ribavirin, Acyclovir, etc.) - if the disease is viral in nature - a mosquito or tick bite, a secondary disease against the background of another virus.
- Antibacterial (antibiotics) – for encephalitis caused by bacteria: Streptomycin, Cefixime, etc.
- Human immunoglobulin is prescribed for severe encephalitis.
- Intravenous infusion drugs to remove toxins from the body;
- Vitamins.
Depending on the symptoms of the disease, the following may also be prescribed:
- Non-steroidal anti-inflammatory drugs (Paracetamol, Ibuprofen and others).
- Neuroleptics (Sonapax, Ridazine);
- Anticonvulsants (Difenin, Sibazon, Seduxen, Phenobarbital);
- Stimulators of neuromuscular transmission (Prozerin, etc.);
- Medicines that correct the mental state, prevent the symptoms of Parkinson's disease, metabolic drugs.
After discharge from the hospital, the patient will need rehabilitation therapy. As a rule, it consists of taking nootropic drugs to improve metabolism in brain tissue. It is very useful to take vitamin, vitamin and mineral complexes, attend exercise classes, massage sessions, and physiotherapy procedures. Spa treatment is also indicated.
Treatment tactics
Viral infections of the brain - encephalitis - are characterized by a fulminant course. Therefore, therapy for such diseases must be comprehensive and, if possible, early. As a rule, it includes several areas:
Etiotropic effect – massive antiviral therapy:
- Ganciclovir;
- Acyclovir;
- Ribavirin;
- less often - the introduction of specific immunoglobulins.
Pathogenetic treatment – correction of vital activities:
- cardiac glycosides;
- vasoactive drugs;
- oxygen therapy;
- mechanical ventilation;
- decongestants;
- antihypoxants;
- neuroprotectors;
- glucocorticoids.
Symptomatic therapy consists of relieving secondary clinical signs:
- antipyretics;
- antiemetics;
- psychotropics;
- anticonvulsants.
During the recovery period, treatment of viral encephalitis involves vascular as well as neuroprotective therapy - in order to accelerate the regeneration of cerebral structures and brain functions.
If paresis and paralysis have formed, the doctor will prescribe complexes of physical therapy, physiotherapy, as well as various options for massage or acupuncture. In case of severe mental disorders, consultation with a psychiatrist and psychotherapist will be required to carry out appropriate corrective action, as well as social adaptation.
How to treat osteomyelitis
The disease can be treated conservatively or surgically. Most patients manage without surgery. Treatment lasts from six months to two years (mostly). In the acute phase of the disease, bed rest is indicated.
There is a risk of chest deformation, therefore, in order to stabilize the spine and reduce pain, the patient should be immobilized. The patient will lie on a special bed for about three months.
The medications used are antibiotics, immunostimulants, and tonic drugs. After the acute symptoms subside, the patient can get up; doctors will fix the spinal column with a corset. Therapy is monitored by laboratory tests. During the rehabilitation period, exercise therapy is needed (to stimulate muscles).
In general, we can say that the success of treatment is early diagnosis, adequate therapy, the degree of damage and, of course, the desire of the patient himself to be cured.
The desire of the sick person to be cured
Prevention
To protect their own health, every person needs knowledge of how viral encephalitis is transmitted and what needs to be done to avoid such a pathology. For this purpose, specialists have developed a special set of preventive measures.
So, prevention of viral encephalitis is, first of all, strong immunity. Therefore, doctors recommend that all people be vaccinated in a timely manner, both against seasonal viral infections, for example, influenza, and against other diseases that can become a platform for inflammation of brain structures - measles, mumps.
A prerequisite for increasing your own immune barriers is proper nutrition. The diet must include fresh vegetables and fruits, more greens and fiber, seafood and grains. They contain those vitamins and microelements that are necessary for the smooth functioning of the brain.
Secondary prevention measures include hardening and giving up bad personal habits - consuming tobacco and alcohol products. Timely elimination of various infectious foci in the internal organs - caries, chronic tonsillitis, pharyngitis, sinusitis, pyelonephritis, gastritis, also helps the body itself to cope with the onset of encephalitis.
In general, no specific prevention - for example, the introduction of a vaccine - has not been developed to date. After all, the number of viruses that can provoke brain inflammation is enormous. Therefore, it is simply impossible to create such a medicine. Experts urge people to exercise caution during the flu and acute respiratory infections season, dress appropriately for the weather, and avoid places where already infected people gather.
Symptoms of inflammation of the brain
In brain inflammation, the symptoms are not so vivid and specific that the patient himself would initially assume that he has such a serious disease. The manifestations of symptoms depend on the source of inflammation, the age of the patient, and the true cause of this pathology.
Signs of brain inflammation:
- General lethargy, malaise, which is not replaced by activity and relief after the person has slept and rested;
- Regular, long attacks of headaches;
- Vomit;
- Hyperthermia;
- The appearance of hallucinations;
- Joint and muscle pain, cramps.
Neurological symptoms are also quite eloquent. The patient experiences joint stiffness, his consciousness and emotional background change, problems arise with pronouncing words, and the motor activity of the eyeballs is disrupted.
The person becomes very anxious, he cannot sleep normally, his mood is bad. Mental disorders can appear suddenly.
There are often cases when, against the background of an illness, a patient experiences psychomotor agitation, when, as people say, he “does not know what he is doing.” In such cases, his behavior is inappropriate, but he is unable to control himself.
Consequences
All infectious diseases of the brain carry the threat of intellectual and physical impairment. However, the consequences of encephalitis, which occurs in a mild form, are completely reversible - the person recovers completely and can return to professional duties almost immediately after recovery.
Whereas with moderate severity, the pathology leads to decreased hearing and vision, strangulation of speech and motor activity. The rehabilitation period can last up to six months and it is not always possible to fully restore health - the person remains with memory defects and decreased intelligence.
Severe encephalitis has a particularly severe effect - with the development of cardiac or respiratory failure, as well as coma. Death occurs in 2/3 of cases. Otherwise, when a person returns to consciousness, he remains deeply disabled and requires constant outside care. He shows a significant personality change.
Less commonly, the transition from an acute form of viral brain damage to a chronic type of disease occurs - exacerbation occurs with a decrease in immunity, overwork, or due to a person’s alcoholism. Symptoms will be less pronounced, however, complications occur more often. Timely seeking medical help and following all doctor’s prescriptions helps to exclude such an outcome. Encephalitis can be defeated and prevented if every effort is made.
Prevention of encephalitis
You can be vaccinated against encephalitis. Vaccination of the population is necessary in areas of distribution of insect species that transmit this disease. There are 3 vaccinations against ticks, which provide protection to the body for 3 years.
For influenza and measles, against which encephalitis can develop as a complication, the patient is administered special immunoglobulins for prophylactic purposes.
Non-pharmacological types of prevention concern behavior when visiting forest areas. When going outdoors, it is wise to dress in closed clothing that prevents insects from penetrating the skin, and also treat things with repellents. They can be purchased at hardware stores or pharmacies. Compliance with personal hygiene rules plays an important role. During tick season, every time you change clothes, you need to carefully inspect your armpits and other places where the insect could go unnoticed.
Special preventive measures should be taken by forestry and horticultural workers. It is best for them to work in special clothing impregnated with a compound that has a paralyzing effect on ticks (acaricide). At the same time, measures must be taken to reduce the number of ticks in forests and parks.
If a tick bite occurs or you find it attached to your body, you need to urgently seek medical help. To prevent encephalitis, the victim of the bite is given an injection of immunoglobulin. There is no need to crush the tick with your hands, because... With the slightest crack or scratch on the skin, pathogens can enter the body. If you feel unwell after coming into contact with a tick or simply visiting an area with dense vegetation, you should consult a doctor. In addition, if there is a risk of contracting encephalitis, you should not drink unboiled fresh milk from cows and goats.
Pathogenesis
How can you get infected?
Natural reservoirs for the virus are wild animals and birds - in particular, ungulates, small rodents, etc. Ixodid ticks are one of the main parasites of these warm-blooded animals, since they need blood for growth and development. Insects become infected with the virus after biting a host, after which it remains dormant in their saliva, and thus they themselves become carriers of the infection and can transmit it to their offspring.
Infection most often occurs through transmission, that is, after direct contact with an infected tick - not only through a bite, but also when trying to crush the insect. Less commonly, pathogenic microorganisms are transmitted through the nutritional route - they enter the gastrointestinal tract along with contaminated milk, dairy products or poorly cooked meat.
An insect bite does not necessarily lead to infection, since only 6 out of 100 individuals are carriers of the virus (all other parasites are sterile), but you should not rely on statistics. Ixodid ticks carry not only encephalitis, but also other dangerous diseases (such as borreliosis, relapsing fever, spotted fever, tularemia, ehrlichiosis), so if the parasite is attached, you need to consult a doctor and get diagnosed.
REFERENCE! It is quite difficult to accurately determine the most dangerous areas in terms of infection with tick-borne encephalitis, since outbreaks of the disease are observed in different regions. A list of places with an increased risk of infection is published annually by state authorities monitoring the epidemiological situation.
Risk group
Brain inflammation can happen to anyone, but most often the disease occurs due to the following risk factors:
- Season. This factor refers to diseases transmitted through insect bites (ticks, mosquitoes). This type of infection mainly occurs in summer and autumn;
- Age. Most types of encephalitis occur in children and older adults, except for infections caused by the herpes virus. Her age category is from 18 to 45 years;
- Weak immunity. This group includes people with the immunodeficiency virus (HIV) and patients who suffer from cancer. After all, they are forced to undergo chemotherapy and radiation, which kill their immunity. This group also includes people taking pills to suppress the immune system and hormonal drugs, which have a similar effect with long-term use;
- Localization area. This factor relates to the habitat of mosquitoes and ticks capable of infecting encephalitis, since they are mainly concentrated in certain areas;
- Camping. They are especially often bitten in forest areas. According to statistics, 1 insect per 1,500 individuals is infected, but with a large cluster, the chances of contracting the infection increase.
Classification of inflammatory changes in the brain
According to statistics, about 80% of the population are carriers of the herpes simplex virus. The main clinical manifestations of the infection are characteristic rashes on the lips, less often on the genitals. For unknown reasons, the virus affects the brain in some people. The mechanism of development of the disease is explained by two theories:
- The virus penetrates the mucous membranes and reaches the vegetative nodes along the nerve processes. There the pathogen replicates, and it enters the brain along nerve fibers.
- The virus also reaches the nerve nodes and enters a latent state. The inactive infectious agent is transferred to the brain tissue, where it is activated and starts the entire pathological process.
The development of herpetic meningoencephalitis in a third of all patients occurs after the first contact with the virus. In 2/3 of patients, encephalitis develops as a reactivation of a latent infection.
In a dormant state, the viral agent is located in the bulb of the olfactory trigeminal nerve. Along it, it spreads to the temporal and frontal lobes of the brain. This explains the main symptoms of the disease and the formation of foci of necrosis only in these areas.
But meningoencephalitis caused by herpes does not develop in all infected people. It has been established that there is a predisposing factor in the form of innate characteristics of the immune system. The reason lies in a mutation or deficiency of certain genes. Acquired immunodeficiency or decreased immunity as a result of taking medications rarely leads to encephalitis herpes.
A person with encephalitis does not necessarily have to have all of the following symptoms. Their number and severity depend on the location of the source of inflammation, as well as on its intensity.
Most typical symptoms
- headache (this symptom is constant);
- temperature increase;
- impaired consciousness (from confusion to coma);
- hallucinations (auditory, visual, tactile, gustatory, olfactory);
- dizziness, loss of balance, coordination;
- weakness in the limbs;
- numbness in the arms or legs;
- speech impairment (difficulty pronouncing words or understanding speech);
- involuntary movements in the muscles of the limbs or face;
- oculomotor disorders (drooping of the upper eyelid, double vision, strabismus).
Epidemic encephalitis is now rare, but there was an epidemic of the disease in the early twentieth century. The incubation period is 12–20 days. In the acute stage, the patient has severe drowsiness. After 3–4 months, the chronic stage develops: trembling of the hands and head and involuntary movements in the limbs appear. Children are characterized by changes in personality, character, and intelligence.
Tick-borne encephalitis occurs in a more severe form in the eastern regions of Russia than in the western regions. The incubation period after a tick bite is 14–20 days.
Ixodid tick is a carrier of tick-borne encephalitis
If infected through goat's milk - 3-7 days. Most of the sick are children and teenagers.
Despite the fact that tick-borne encephalitis is a severe disease, asymptomatic cases sometimes occur. This type of trend is typical for children whose ancestors lived in taiga regions for several generations. In these cases, innate immunity is probably formed.
Herpetic makes up 80% of primary encephalitis. Newborns become infected in utero if the mother has genital herpes. Areas of brain necrosis, cysts and foci of calcification develop.
A child under one year old is not yet able to complain of a headache. Therefore, parents should pay attention to the following alarming symptoms:
- baby rubs his head on the pillow;
- cries;
- refuses food;
- does not take the breast.
Enteroviral encephalitis is relatively benign if the child is hospitalized in a timely manner. The incubation period is one week. Vomiting and diarrhea are often associated.
The disease is more severe in children under one year of age. Since intracranial pressure is increased with this pathology, attention is paid to the swelling of the fontanel. Spinal puncture quickly improves the patient's condition.
Secondary encephalitis: rheumatic, post-vaccination
Secondary encephalitis due to infectious diseases (measles, chickenpox, rubella) develops 3–7 days after the appearance of the rash.
https://www.youtube.com/watch?v=aMJvUQ9-MJI
Rheumatic encephalitis affects the subcortical nodes of the brain. As a consequence of this, involuntary movements appear in the limbs (large chorea) or facial muscles (minor chorea). The child begins to grimace, grimace, and wink. Such symptoms are characteristic of adolescence.
A child who has suffered rheumatic encephalitis may grimace, grimace, wink
Post-vaccination encephalitis develops after vaccinations; neurological symptoms appear on days 10–14. It is important to associate these symptoms with vaccination and exclude other pathogens of encephalitis.
Tick-borne encephalitis
This disease is exclusively seasonal, occurring in spring and summer. The main source of infection are ixodid ticks that live in wooded areas. Tick-borne encephalitis occurs after the virus enters the body due to the bite of an infected tick. In more rare cases, infection occurs through nutritional means, for example, after consuming milk from infected animals. The incubation period of the disease can last from 8 to 20 days; if the bite occurs on the head, the incubation period is shortened and lasts from 4 to 7 days. The disease begins with an acute course: a person suffers from vomiting, severe headache, and photophobia. Body temperature rises sharply, reaching 39-40°C. Sometimes with tick-borne encephalitis repeated hyperthermia occurs. In this case, the symptoms of encephalitis are even more pronounced. The patient exhibits hyperemia of the sclera, pharynx, skin, and various dyspeptic disorders. A blood test reveals an increase in ESR , leukocytosis , and lymphopenia . In particularly severe cases, the respiratory muscles may be affected and bulbar disorders may occur.
Tick-borne encephalitis has several clinical forms: poliomyelitis , meningeal , polioencephalomyelitis , cerebral and effaced .
With the meningeal form of tick-borne encephalitis, pronounced meningeal symptoms appear. Due to inflammation of the brain and its membranes, a person experiences disorders of consciousness, epileptic seizures, delirium, and paralysis . Manifestations of convulsions are possible with the likelihood of their transition to a general convulsive attack.
With encephalitis of the polioencephalomyelitis form, the patient exhibits flaccid paralysis of the muscles of the shoulder girdle and neck. Bulbar and meningeal disorders may occur.
In patients with the plenomyelitic form of encephalitis, the symptoms include paresis and paralysis of the neck, arms, and the patient’s head hangs unnaturally on the chest. A person’s sensitivity is not impaired, but motor functions are impaired. In the erased a fever for two to four days , neurological symptoms do not appear, but there is tachycardia and periodic attacks of arterial hypertension. There is also a progressive form of the disease, in which periodic twitching of certain muscle groups is noted. These are mainly the muscles of the arms and neck.
Toxoplasmic encephalitis
Toxoplasmic encephalitis. The causative agent of the disease is Toxoplasma gondii. Acute toxoplasmosis encephalitis is rare. Most often, the disease develops gradually.
In the acute form of the disease, increased body temperature, generalized lymphadenopathy, hepatosplenomegaly, pneumonia, myocarditis, conjunctivitis, pharyngitis, skin exanthema, and monocytosis are noted. The latter is often mistaken for infectious mononucleosis. The cerebrospinal fluid is xanthochromic, its protein content is moderately increased, and lymphocytic pleocytosis is determined.
In the acute stage, Toxoplasma is sometimes isolated from blood, urine, cerebrospinal fluid and lymph nodes.
Rubella encephalitis - symptoms and treatment
Encephalitis in exanthemal infections in children is one of the specific complications of acquired rubella. In recent years, the frequency of this type of encephalitis reaches 1:4000 - 1:13,000 of the population, mainly between the ages of 5 and 14 years. In recent decades, it has been proven that the rubella virus is the cause of the development of subacute sclerosing panencephalitis and multiple sclerosis.
Causes of encephalitis due to rubella
The rubella virus has both a direct pathogenic effect on the nervous system and plays the role of a specific allergen that causes the formation of delayed-type immunopathological reactions. This produces autoantibodies against brain tissue that interact with myelin basic protein and microglia. This variant of the reactivity of the macroorganism contributes to the formation of persistent forms of infection and the development of symptoms of panencephalitis.
During pathomorphological studies in the brain, and in cases of encephalomyelitis and the spinal cord, foci of inflammatory-infiltrative nature and demyelination are determined, as well as the reaction of micro- and macroglia.
Symptoms of encephalitis with rubella
The development of encephalitis does not depend on the severity of rubella. Neurological symptoms usually appear on days 3-5 of the disease (at the end of the rash period), less often on days 9-15. In 8 - 10% of cases, encephalitis develops before the rash appears (1-2 days).
The onset is acute, with headache, vomiting, and a repeated rise in body temperature to febrile levels. Most patients experience a rapidly progressing disorder of consciousness up to deep coma, and generalized tonic-clonic convulsions.
From the first days of the disease, focal neurological symptoms appear: motor disorders in the form of hyperkinesis (myoclonus, choreoathetosis, opisthotonus). The following symptoms develop less frequently: central paresis and cerebellar disorders (diffuse muscle hypotonia, scanned speech, intention tremor, dynamic and static ataxia).
The condition of patients is usually severe or extremely severe; Brain edema and bulbar disorders pose a threat to life. In most cases, rubella encephalitis is acute, with a critical drop in body temperature and rapid reversal of symptoms. However, in some cases, convulsions can last up to 5-6 days, impaired consciousness - up to 1 week. Mortality is 10-20%, death usually occurs in the first three days due to intractable cerebral edema.
Diagnosis of encephalitis with rubella
Supportive diagnostic signs of rubella encephalitis:
- connection of the disease with rubella or contact with a person with rubella;
- repeated rise in body temperature to high numbers;
- Strong headache;
- sudden loss of consciousness;
- generalized clonicotonic seizures;
- focal symptoms.
Laboratory diagnosis of encephalitis due to rubella
https://www.youtube.com/watch?v=u1ZEplNWjRk
Changes in the cerebrospinal fluid may appear a few days after the clinical manifestations of encephalitis, and only with a repeated lumbar puncture on the 4th - 5th day of illness, a slight lymphocytic pleocytosis and an increase in protein (up to 2.0 g/l) are revealed.
A virological study is carried out to isolate the virus from the blood (in the first 3 days) and cerebrospinal fluid (in the first 7 days of illness).
In order to determine specific antibodies in the blood and cerebrospinal fluid, serological methods are used in the dynamics of the disease (RN, RSK, RTGA).
Treatment of encephalitis due to rubella
Observance of strict bed rest, organization of care and balanced nutrition are important. The use of immunoglobulin for intravenous administration (endoglobulin, pentaglobin, sandoglobulin), recombinant interferons (viferon), inducers of endogenous interferon (amixin, larifan, etc.) is indicated.
Now you know the main causes and symptoms of encephalitis in children, as well as how encephalitis in a child is treated. Health to your children!
Treatment
Treatment of patients infected with tick-borne encephalitis is carried out in a hospital setting, and includes several areas - the fight against the virus itself and the consequences of its impact.
The scheme is developed individually and depends on the time that has passed since the first signs of the disease appeared. In the first few days, the introduction of immunoglobulin is effective, as is the use of antiviral drugs, including interferon.
If the central nervous system is damaged, such treatment does not have an effect, so the therapeutic regimen is aimed at stopping pathological processes that can cause serious disorders in the body.
To reduce intracranial pressure and oxygen starvation, artificial ventilation, diuretics, and drugs to improve blood circulation and increase tissue resistance to oxygen starvation are used. In order to improve the condition of the nervous system and increase immunity, antipsychotics, vitamin therapy, and immunomodulators are used.
REFERENCE! A person infected with encephalitis is not able to transmit the virus and therefore does not pose a threat to others.
Course of therapy
If the course of the disease is mild and the pathological process does not develop much, then encephalitis can be treated using the following methods:
- Drinking large amounts of water (more than 2 liters per day);
- Strict adherence to bed rest;
- Taking anti-inflammatory medications, such as Ibuprofen and Naproxen. They not only reduce inflammation, but also normalize body temperature and relieve headaches.
Acyclovir is usually prescribed immediately, since determining the nature of the virus is quite difficult and time-consuming, and treatment must be started immediately. This drug works well on herpes and does not allow serious complications associated with it. There is no point in treating an infection received from an insect with this medication, since the reaction will be virtually zero.
That is why it is important to know how to treat tick-borne encephalitis. The best remedy is considered to be an injection of anti-tick immunoglobulin. This medication is an antibody that can begin to act immediately after it is introduced into the body. The medicine consists of the blood of people who have been vaccinated against encephalitis.
Among the side effects after taking medications with an antiviral effect are:
- Abnormal stool (diarrhea, constipation);
- Weak appetite;
- Vomit;
- Pain in muscles and joints;
- Malfunctions of the kidneys and liver;
- Myelosuppression (decreased bone marrow activity).
The course of therapy must include supportive treatment. It consists of the following points:
- Taking medications to prevent seizures like Dilantin;
- Observations of the respiratory and cardiovascular systems;
- Administration of drugs to compensate for fluid and nutrients;
- The use of corticosteroids to reduce inflammation, as well as eliminate swelling and reduce pressure in the skull.
After a course of therapy, a long recovery period will be required. It will depend on the resulting consequences of encephalitis, but mainly consists of the following stages:
- Physiotherapeutic procedures;
- Treatment with a speech therapist (if necessary);
- Psychotherapy course;
- Long rest, preferably in the fresh air.
Despite the fact that there are currently many different pathogens, there are three main methods of treating the acute form of viral encephalitis:
- etiotropic therapy;
- maintaining all body functions;
- eliminating all possible complications.
Very often, doctors prescribe treatment with glucocorticoids, which relieve inflammation, help avoid allergic reactions and help strengthen the immune system of a sick person.
At the acute stage of the disease, patients take Prednisolone in tablets or injections. In addition, Dexamethasone may be prescribed.
Glucocorticoids are taken in large dosages for no more than 10 days, after which the dose should be quickly reduced, as there is a risk of side effects.
Along with the main treatment, doctors practice the use of potassium and calcium, always monitoring electrolytes.
In order to relieve cerebral edema, it is worth taking diuretics in combination with diuretics, which prevent an increase in edema. During this process, it is imperative to control your fluid intake.
If the swelling is not removed, stem syndrome and problems with breathing and the cardiac system may develop. Such a phenomenon should be an impetus to transfer the patient to intensive care and carry out measures to save him.
When epileptic seizures occur, it is appropriate to take sodium oxybutyrate, Clonazepam, Finlepsin, and enemas with Chloral hydrate. Along with drugs to relieve seizures, a tranquilizer and an antipsychotic are prescribed. This treatment is carried out for a couple of months after the first attack to exclude subsequent attacks.
It is very important to properly care for the patient:
- in this case, the respiratory tract should be cleaned;
- turn the person in bed more often;
- ensure that there are no folds in the bed;
- constantly wipe the body with alcohol or disinfectants;
- perform gymnastics and various massages;
- feed the patient through a tube if there are problems with swallowing food;
- inject antibiotics and allergy medications;
- prescribe anticoagulants that prevent the formation of blood clots in the veins.
Japanese encephalitis
Japanese encephalitis (another name is encephalitis B ) is caused by a virus that is stored and transmitted by mosquitoes. Birds and people can sometimes be carriers of viruses. In this case, the incubation period lasts from three to twenty-seven days. The disease begins to manifest itself acutely: body temperature rises sharply to 40 °C and above, without dropping for about 10 days. The patient is plagued by general malaise, chills, weakness, severe headaches, vomiting, and muscle pain. There is hyperthermia of the facial skin, dry tongue, and the abdomen is strongly retracted. Disturbances in cardiac activity and consciousness of the patient are also possible. There is an increase in the tone of the flexors of the upper limbs and at the same time the extensors of the lower limbs. Sometimes twitching of some muscles and periodic convulsions occur. In severe cases of the disease, bulbar palsy may occur. With this disease, death occurs in approximately 50% of cases.
Complications
The prognosis of measles encephalitis depends on the period of measles during which they occur.
- The worst prognosis is for encephalitis that occurs in the prodromal period: gross organic disorders of the central nervous system remain.
- A severe complication of measles encephalitis, often leading to death, is cerebral vein thrombosis and especially sinus thrombosis.
- With complete recovery after measles encephalitis, asthenic syndrome persists for a long time.
- Many patients remain with residual neurological symptoms: paresis, seizures, decreased memory and level of mental development.
Etiology
The causative agent of viral tick-borne encephalitis is an RNA-containing arbovirus of the genus Flaviviridae, family of togaviruses. It was isolated and studied by USSR scientists in the late 40s of the 20th century; before that, the disease was considered a type of influenza with a neurotoxic type of course.
The basis of this virus is a nucleocapsid with a cubic type of symmetry, consisting of single-stranded RNA and structural protein C. It is packaged in a spherical supercapsid, which is formed by a combination of lipids and 2 glycoproteins: membrane (type M) and envelope (type E).
The causative agent of tick-borne encephalitis dies within 2-3 minutes during boiling and pasteurization, and is quickly destroyed by the action of solvents and basic disinfectants. At the same time, it is very resistant to low temperatures, which gives it the opportunity to successfully survive in the bodies of ticks even during severe frosts in Far Siberia. In addition, it is almost insensitive to the action of low concentrations of hydrochloric acid and digestive enzymes, therefore it is able to survive and exhibit virulence when it enters the gastrointestinal tract of warm-blooded animals.
Although the pathogen is sensitive to many environmental factors, it persists for a long time in a dried state and in living cells, even outside the phase of its reproduction. Therefore, in nature it is found mainly in the bodies of ticks and a number of warm-blooded animals, which are natural reservoirs for it. In addition, some dairy products (milk, butter) are a source of infection.
In laboratory conditions, the virus is well cultivated on chicken embryos and in various tissues, although with prolonged passage under such conditions, the pathogenicity decreases somewhat. Of the laboratory animals, the most sensitive to it are white mice, hamsters, young rat pups, and monkeys.
Classification of inflammatory changes in the brain
The incidence of nervous system lesions in chickenpox is 0.1-0.7%, of which encephalitis is up to 90%. Encephalitis is most often observed in children with primary immunodeficiencies, iatrogenic immunosuppression, and after organ transplantation.
Causes of encephalitis in chickenpox
In conditions of reduced immunoreactivity of a child with chickenpox, dissemination of the virus with the development of encephalitis and encephalomyelitis is possible. The nature of brain damage in chickenpox is due to both the direct effect of the virus and the infectious-allergic process that determines the genesis of damage to the central nervous system.
In chickenpox encephalitis, the pathomorphological picture is represented by perivenous inflammatory-infiltrative changes, micro- and macroglial infiltration, and demyelination. Mainly the cerebellum is affected, less commonly the brainstem and spinal cord.
Symptoms of encephalitis with chickenpox
In patients with chickenpox, neurological disorders often appear on the 3rd to 8th day of the rash period. In some cases, symptoms of encephalitis precede the appearance of a rash.
This type of encephalitis occurs acutely, against the background of severe fever, sometimes low-grade body temperature. The most typical for chickenpox encephalitis are cerebellar disorders (cerebellitis), which are manifested by an unsteady gait (ataxia), diffuse muscle hypotonia, nystagmus, scanned speech, intention tremor, difficulty performing coordination tests, static ataxia (the patient cannot sit or stand).
Damage to the cerebellum may be the only manifestation of chickenpox encephalitis or be combined with other focal symptoms: pyramidal signs, hemiparesis, damage to the cranial nerve nuclei, aphasia, agnosia, hyperkinesis. Possible disturbances of consciousness and convulsions. In some cases, children develop meningoencephalitis.
Treatment prognosis: encephalitis that occurs at the end of the rash period ends favorably in most cases. Residual effects in the form of paresis, hyperkinesis, and epilepsy are observed in 15%. Mortality averages 10%.
Diagnosis of encephalitis in chickenpox
Supportive diagnostic signs of encephalitis in chickenpox:
- connection of the disease with chickenpox or contact with a patient with chickenpox;
- repeated rise in body temperature;
- disturbance of consciousness;
- cerebellar disorders.
During lumbar puncture, cerebrospinal fluid flows out under pressure, is transparent, the number of cells remains within normal limits, and a moderate increase in protein is determined. The presence of pleocytosis indicates meningoencephalitis.
Identification of the pathogen in the cerebrospinal fluid is carried out using the virological method (isolation of the virus on embryonic cultures of human cells); with electron microscopy. Detection of virus antigens is carried out using the immunofluorescent method. The serological method (RSM) allows you to detect specific antibodies in the blood and cerebrospinal fluid.
Treatment of encephalitis due to chickenpox in children
Patients are subject to mandatory hospitalization with strict bed rest during the entire acute period. The use of antiviral drugs (acyclovir, valacyclovir), recombinant forms of interferon (viferon) is indicated.
Treatments for chickenpox encephalitis
Intensive therapy for cerebral edema and swelling is carried out with the mandatory use of glucocorticoids. In order to increase the energy supply to the brain, piracetam and nootropil are prescribed; to improve the aggregative properties of blood and improve cerebral circulation - Cavinton and Trental.
After suffering from encephalitis, children are observed by a pediatrician and a neurologist with instrumental research methods (EEG, ECHO-EG, neurosonography, CT, NMRI). During the first year, examination by specialists is carried out once every 3-4 months, in the second year - once every 6 months. Deregistration is carried out no earlier than 2 years after the illness in the absence of residual effects.
How does the disease progress?
The first symptoms of viral encephalitis can be flu-like: general malaise, fever, runny nose, sore throat and sore throat.
After this they join:
- headache;
- nausea, vomiting;
- hypersensitivity to light and sounds;
- disorientation in space and time;
- loss of consciousness;
- in some cases, hallucinations;
- convulsions (in about half of patients).
In infants with encephalitis, the fontanel bulges.
Depending on the specific area of the brain affected, focal neurological symptoms may occur. For example, speech disturbances can occur with inflammation in the frontal or temporal lobes, disorders of vision and oculomotor functions - in the occipital and temporal lobes, changes in coordination, decreased muscle tone, tremor - due to damage to the cerebellum.
- oculomotor and auditory disorders;
- loss of skin and taste sensitivity;
- speech and breathing disorders;
- paralysis or paresis of facial, lingual muscles, larynx.
Intrauterine infection is accompanied by damage to other internal organs (liver, kidneys, lungs).
The disease can often involve the meninges, which leads to the development of meningeal symptoms:
- stiffness of the neck muscles, the patient adopting a characteristic pose with legs pulled up to the stomach and head thrown back;
- inability to straighten the patient’s leg at the knee while it is bent at a right angle at the hip joint (Kernig’s symptom);
- flexion of the leg at the knee and hip joints with passive flexion of the patient's head, pressing on his pubic symphysis and flexion of the other leg (Brudzinski's symptoms).
The course of viral encephalitis can be sluggish or acute.
The first option is not always preferable; in its case, the risk of death even increases: symptoms can “masquerade” as other diseases, and if treatment is not started on time, it leads to the development of complications. This can, for example, happen with herpetic encephalitis. In this case, signs can only be expressed in a slight rise in temperature, asthenic syndrome, and the appearance of short-term convulsions without loss of consciousness.
Features of the disease
The development of this type of brain inflammation occurs under the influence of a viral infection. Encephalitis is caused by different types of viruses. Most often, the lesion occurs as a result of herpes, childhood viruses similar to measles. The disease can also be caused by bites from infected mosquitoes. In this case, the membrane of the brain and the peripheral nerve are affected.
Pathology can develop in primary and secondary forms. In the first case, a viral disease occurs in the brain and spinal cord. With a secondary infection, other organs become infected, from which the virus spreads through the bloodstream throughout the body.
The causative agent of encephalitis can be transmitted by people and insects. Infection occurs:
- by air;
- sexually;
- through the consumption of dairy products;
- when touched.
Disease activity increases in the spring and summer. The development of enterovirus infections subsides at the end of summer.
Characteristics of common forms
According to statistics, the herpes virus is detected in 90% of the population. In approximately 20% of cases, a viral infection causes serious disruptions in the body's functioning. Once entering the body (hematogenous, neuronal route), HSV (herpes simplex viruses) remain in it forever. An infectious agent can be in different states, which determines the degree of its impact on health. The following forms of pathology are distinguished:
- Latent (hidden).
- Persistent (chronic).
- Progressive (with increasing symptoms).
- Recurrent (with alternating periods of progression and remission).
Under favorable conditions, reactivation of a latent infection occurs. The acute form of the pathology can lead to loss of ability to work, disability, and death. HSV is characterized by pantropism - the ability to infect different organs and systems. Infectious agents cause pathological autoimmune reactions, induce the formation and growth of malignant neoplasms, and cause perinatal pathologies.
Penetrating into the central nervous system, viruses provoke the development of temporal lobe epilepsy of the median type. Encephalitis caused by viral agents is a common (about 76% of cases) forms of encephalopathies of various (bacterial, fungal, anaplasmic) etiologies. Herpetic encephalitis in children usually occurs acutely and provokes the appearance of persistent neurological deficits, often of a focal type. The disease often causes retardation in the mental and physical development of the child.
Herpetic encephalitis in adults is more often detected in patients of two age groups: under 30 years of age and over 50 years of age. In most cases (about 95% of cases), the infectious agent is type 1 HSV, which affects the mucous membrane and skin of the face in the mouth area. HSV type 2 affects the mucous membrane of the genital organs. It is more often detected in newborns, who are transmitted from an infected mother during fetal development.
In the body of 70-90% of infected people, antibodies to the viral agent are detected, which in normal conditions helps to suppress the activity of HSV by one’s own immune system. From the point of view of pathomorphology, the disease is an acute necrotizing process, which is characterized by the appearance of multiple foci of hemorrhage, lymphocytic and plasmacytic infiltration in the brain tissue.
In the acute stage of the disease, eosinophilic elements (granulocyte leukocytes) are found in the nuclei of nerve cells (neurons, neuroglia). Typical localization of the pathological focus is the medial (middle) part of the temporal lobes and the orbital (lower) part of the frontal lobes. In the residual (after the acute stage) stage of the course, cystic-glial tissue is formed at the site of foci of necrosis.
Below is information about the etiology, pathogenesis, clinical symptoms, treatment methods and prevention of various types of viral encephalitis.
In the International Classification of Diseases, 10th revision (ICD 10), tick-borne encephalitis is considered under heading A84. The disease is caused by the penetration of the virus as a result of a tick bite or when an insect is crushed. The primary site of localization is the skin, from where the infectious agent penetrates the central nervous system through hematogenous or lymphogenous routes. Tick-borne encephalitis is characterized by damage to the gray matter of the brain and its membranes.
The incubation period ranges from one to three weeks. The first sign of the disease is a rise in temperature to hyperfebrility. The patient indicates severe cephalalgia, chills and fever, nausea and repeated bouts of vomiting. Already on the first day, redness of the skin of the face and injection of scleral vessels are noticeable. A typical symptom of tick-borne encephalitis is excessive sensitivity to light sources.
When the eyes work, severe pain occurs. The person looks lethargic and drowsy. On the third day, disturbances of consciousness are observed, sometimes to the point of coma. A convulsive syndrome develops until the patient acquires status epilepticus. The death of the patient most often occurs on the first or third day.
No specific treatment has been developed. As an emergency measure, the patient is given a specific immunoglobulin. In epidemically unfavorable regions, it is recommended to take measures to prevent viral tick-borne encephalitis. The main method is active immunization by administering a vaccine.
Mosquito (Japanese) encephalitis is considered in ICD-19 under code A83. The disease occurs in an acute form and is characterized by severe damage to brain tissue. The reservoir of infection is wild animals and birds. The carrier of the virus in nature is mosquitoes. Human infection occurs through insect bites. Mosquito encephalitis is a seasonal disease; outbreaks of the disease occur during the breeding season of bloodsucking mosquitoes. At risk are people living or working in humid regions or wetlands.
The virus has a pronounced neurotropic effect. After a bite, the pathogenic agent enters the structures of the central nervous system by hematogenous route, where it rapidly multiplies in neurons. The first evidence of infection is hyperfebrile fever, debilitating chills, and unbearable headache.
Patients' complaints include severe nausea and repeated vomiting attacks. The skin of the face turns red. Scleritis and conjunctivitis are detected. A neurological examination performed on the third day reveals meningeal syndrome. The person is in a depressed state of mind and does not respond to environmental stimuli.
The prognosis for mosquito encephalitis is unfavorable. The fatality rate reaches 50%. Complications of the disease are asthenic syndrome, impaired cognitive functions, and the development of psychoses. Treatment of viral encephalitis is pathogenetic and symptomatic. The main preventive measure is the destruction of blood-sucking insects.
Lethargic (epidemic) encephalitis Economo is an infectious lesion of brain structures caused by an unidentified virus. Sources of infection are infected and sick people. The entrance gate is the upper respiratory tract, since the pathogenic microorganism is transmitted by airborne droplets. It is possible for the fetus to become infected from an infected mother during pregnancy.
Upon penetration into the blood and then into the central nervous system, the virus accumulates in the neurons of the gray matter. At the end of the replication period, microorganisms again enter the bloodstream, which is manifested by the development of disease symptoms.
The classic signs of Economy encephalitis are intoxication syndrome: fever, headache, nausea and vomiting. Catarrhal phenomena similar to the symptoms of acute respiratory viral infections are observed. A typical evidence of the disease is a sleep pattern disorder, manifested by insomnia at night and excessive sleepiness during the daytime. Traditional symptoms are oculomotor disorders and vestibular disorders.
The disease is fraught with transition to a chronic form. In the stage of fading of symptoms, a person is worried about fatigue, weakness and nervousness. As the disease worsens, symptoms of parksionism occur. The outcome of the disease is the development of persistent intellectual impairment.
For this form of the disease, the treatment strategy is similar to the treatment of other viral encephalitis. Preventive measures have not been developed.
Lymphocytic meningoencephalitis is a disease caused by infection of the human body with viruses of the arenovirus family. The carriers and reservoir of infection are rodents: mice, rats, guinea pigs. A larger number of cases are rural residents and people working in their summer cottages.
Infected animals excrete the pathogen in excrement and mucous membrane secretions. In this case, viruses accumulate on household items, food, and water sources. The virus enters the human body through nutritional or airborne routes. Infection can occur through direct contact with infected rodents.
From the moment of infection until the appearance of the first clinical symptoms, an average of 8-9 days pass. The first sign is an increase in body temperature to 40°C. The person is overcome by severe chills and intense cephalgia. He feels broken and weak. The patient's complaints include repeated bouts of vomiting. Typical symptoms of this type of encephalitis are increased sensitivity to presented stimuli, severe sleep disorders, and meningeal signs. In the flowering phase of the disease, paresis, convulsive syndrome, and impaired consciousness in the form of stupor occur.
The disease is benign in nature and most often ends in complete recovery of the person. There are no specific drugs, so therapy is carried out aimed at eliminating the demonstrated symptoms. The main preventive measure is the regular implementation of measures to eliminate domestic rodents. A vaccine against lymphocytic meningoencephalitis has not been developed.
Causes and method of transmission of the virus
It is not always possible to determine the cause of this infectious disease, so you should carefully monitor how the disease progresses in order to identify its specifics.
Epidemiology
In most cases, disease carriers are sick people and arthropods. Birds and some animal species have been designated as additional reservoirs for vector-borne infections.
This virus enters the human body through airborne droplets, fecal-oral, contact and sexual contact, as well as through consumption of stale milk. The culmination of parasitism and the spread of infection occurs in spring and summer.
Pathomorphology
There is a predominance of perivascular inflammation, swelling and various modifications of the nerve elements are observed. The focus of damage and spread in the brain is in the subependymal zone of the ventricles, as well as the ependyma.
In the cells of epithelial tissue, giant cells with nuclear inclusions can be traced. Rabies is characterized by Babes-Negri bodies found on the skin of the base of the neck and the brain.
Multiseasonal encephalitis
Multiseasonal encephalitis. This is a collective group of encephalitis of unknown etiology. The disease is not characterized by seasonality and manifests itself with a variety of symptoms. The most common syndromes that develop are brainstem, cerebellar and hemispheric syndromes.
Stem syndrome is characterized by dysfunction of the oculomotor and abducens nerves, and damage to the pons is characterized by dysfunction of the facial nerve. Vestibular and even bulbar disorders are sometimes observed. Cerebellar syndrome is manifested by disturbances in statics, gait and coordination, hypotonia and dysmetria, ataxia, and asynergia.
Some patients experience various combinations of brainstem, cerebellar and pyramidal symptoms. Hemispheric syndrome is characterized by epileptic seizures (focal or cerebral), acute paresis or paralysis, and hyperkinesis. There may be a disturbance of consciousness, up to stupor and coma. Cerebrospinal fluid leaks iodine pressure, lymphocytic pleocytosis and a slight increase in the amount of protein are noted.
Types of pathogen
The genetic composition of the causative agent of tick-borne encephalitis varies in different natural foci, which is taken into account when classifying the disease. Based on the gene encoding the capsular protein E, several viral varieties are distinguished:
- 1 genotype – Far Eastern;
- genotype 2 – Central European or Western;
- genotype 3 – Greek-Turkish;
- genotype 4 – East Siberian;
- Genotype 5 – Ural-Siberian (it is one of the most common; in the Russian Federation, in most cases this is what is detected in sick people).
Genotypes have differences in virulence and the nature of the disease, which explains some of the features of tick-borne encephalitis in different countries and regions.
Encephalitis: medical history, causes and types
First, a short historical excursion.
Epidemic encephalitis: historical background
- The disease was first described by Sydenham in 1673. Then the pathology was called something like nervous cerebral fever.
- Epidemic encephalitis first manifested itself at the end of the 19th century: in 1891, an epidemic of hemorrhagic E. broke out in Europe. The reason was the increased migration of people from Asia, Africa, Egypt, where encephalitic mosquito fever had been observed for centuries. But then they did not yet know about the viral nature of E.
- In 1917, a new type appeared - lethargic or Economo. Encephalitis lethargica is transmitted by airborne droplets, leading to a pandemic outbreak between 1918 and 1926. Later, lethargic encephalitis was renamed Japanese (after the name of the country where there were the highest number of cases and the highest mortality rate, which reached 60%).
- In 1933-36, it was finally proven that the causative agents of epidemic E. are viruses.
Causes of encephalitis
The causative agents of the disease are:
- arboviruses transmitted by ticks and mosquitoes;
- viruses of meningitis, rabies, polio;
- steam viruses (mumps, measles, rubella, chickenpox, influenza);
- bacteria (coccal, brucellosis, Koch's bacillus, spirochetes, enterobacteria);
- intracellular parasites (rickettsia);
- single-celled protozoa (amoeba, toxoplasma, mycoplasma, etc.);
- fungal bacteria;
- helminths.
In most cases, the presence of infection in the blood does not lead to the disease E. Low immunity and failure to comply with preventive and precautionary measures can contribute to the disease.
Primary encephalitis
Based on the cause, the pathology can be primary or secondary.
Types of primary encephalitis:
- tick-borne;
- mosquito;
- lethargic encephalitis (or Japanese);
- equine (mainly distributed in the USA, South and Central America);
- meningoencephalitis;
- acute disseminated encephalomyelitis;
- acute hemorrhagic E.;
- amoebic meningoencephalitis;
- chorioencephalitis.
How is encephalitis transmitted?
Pathogen transmission:
- when bitten by a parasite through the hematogenous route;
- through food;
- when swimming in a dirty pond (amoebic E.);
- contact method; by airborne droplets.
Primary E. begins with selective damage to the central nervous system, for example, by arboviruses or amoebas. Arboviruses have RNA and live in the blood of infected animals: rodents, birds, horses, cows, goats, pigs, etc.
Primary E. are observed in children and adults, more often in men, due to their greater love of travel and spending time in nature
Tick-borne encephalitis
The carrier of the causative agent of encephalitis (arbovirus) is a blood-sucking parasite, mainly ticks and mosquitoes. Epidemics caused by arboviruses are seasonal (spring-autumn periods).
- The main share of all primary diseases is tick-borne encephalitis, which is widespread in Europe, Russia and parts of Asia. It is transmitted mainly from sick animals (mice, cattle and birds) through a tick bite in a hematogenous way, but it can also become infected through raw dairy products.
- The incubation period of tick-borne E. is from 7 to 14 days.
Mosquito encephalitis and mosquito fever
- Mosquito encephalitis is common in Japan, the Pacific coast and the Far East. It is transmitted primarily from horses, pigs and occasionally birds. Epidemic Japanese encephalitis can begin in the summer.
- Rift Valley mosquito fever is also known, which occurs in African countries (Kenya, Sudan, Egypt). It can also be transmitted by contact, that is, from person to person: this is caused by crushing mosquitoes on the body, scratching bites and introducing infection to the mucous membranes eyes or oronasal cavity.
Sleeping sickness
But the most unstudied remains lethargic encephalitis, which has claimed thousands of lives. It is still unknown exactly what caused the pandemic in 1924: presumably, a neurotropic virus that was transmitted by sick people, as well as by healthy virus carriers. What saves humanity is that a pandemic of this kind has simply never happened again. Since then, only isolated cases of lethargic E. have been observed.
Secondary encephalitis
Secondary E. can be:
- Necrotic: cytomegalovirus and herpetic encephalitis.
- Parainfectious, due to: measles, rubella, mumps, chickenpox, influenza.
- Enterovirus (Coxsackie, Escherichia coli, etc.).
- Neuroviral (meningitis, rabies, polio, tetanus, typhus).
- Neurocollagenous (rheumatism, lupus erythematosus, periarteritis nodosa).
- Specific (due to tuberculosis or syphilis).
- Post-vaccination (based on vaccinations against meningitis, encephalitis, tetanus, etc.
- Serum (cause - serum sickness).
- Medicinal (caused by taking certain drugs).
- Septic (due to traumatic brain injury).
- Gangrenous (from gunshot and shrapnel wounds).
The incubation period for secondary pathologies is on average five to seven days. However, it can be shorter or longer:
- for example, for acute meningitis or rubella from 2 to 5 days;
- with tetanus from several days to three weeks;
- with rabies, the incubation period ranges from several days to several months, and depends on the distance of the bite site from the head - the further it is, the longer the period of absence of symptoms.
Secondary encephalitis is observed more often in early childhood (with the exception of traumatic encephalitis). However, a type such as chickenpox encephalitis is diagnosed in the vast majority of adults who have chickenpox. As you know, chickenpox in adults is much more severe than in children.
Slow encephalitis
A separate group includes encephalitis caused by slow viral infections, the incubation period of which can reach many years:
- Virchow's encephalitis of newborns (a disease that develops mainly due to congenital rubella, occasionally chickenpox, mumps, measles: the virus is transmitted to the fetus from a sick mother);
- subacute sclerosing E.;
- congenital interstitial E. Vilyuisky or Kola (named after the Vilyui River in Yakutia and the Kola Peninsula - those geographical areas where the disease is common).
Slow-onset encephalitis, although generally rare (approximately one in a million cases), has a poor prognosis, is difficult to diagnose, and has a high mortality rate.
Virchow's encephalitis of newborns
In the United States, 60 thousand children die every year from Virchow's encephalitis. The virus can penetrate the brain at the embryonic level, manifest itself in a newborn, or lie dormant for many years. The cause of Virchow's encephalitis is most often rubella contracted by the mother in the first months of pregnancy.
Such a child may not be sick, but pose a threat as a carrier of the virus. Symptoms of the lesion may appear late, sometimes even during adolescence. The disease leads to:
- to blindness, deafness, heart defects, decreased immunity (these are typical symptoms of rubella);
- paralysis, convulsions, mental disorders;
- progressive dementia, up to complete idiocy.
What is viral encephalitis of the brain?
The process of inflammation of brain cells, provoked by a virus that entered the body along with an infection (secondary encephalitis), is called viral encephalitis.
In most cases, when talking about patients who have been exposed to the disease, they mean a complication of a viral infection (herpes, enterovirus).
With secondary encephalitis, there is a hypersensitivity reaction (immunological mechanism), which manifests itself from two to twelve days from the moment of infection.
This type of disease involves changes in the reactions of brain cells with subsequent disruption of their functions. In addition to the presence of the virus, the consequences of this infection are also dangerous. In severe forms of the disease, mental disorder, memory impairment, loss of personality, paralysis of the limbs and loss of coordination are observed.
The disease is specific and, if contacted late, leads to death in 40% of cases.
Research shows that this disease is also hereditary. The mother can pass it on to her children if she is infected during pregnancy. In such cases, they speak of chronic encephalitis in infants.