The pancreas is a complex organ in which benign and malignant tumors develop. Benign neoplasms are represented by adenoma, lipoma (lipomatosis), fibroma (fibromatosis). Serous benign tumors include microcystic and macrocytic serous cystatomas, solid serous adenomas and serous neoplasms. Benign tumors of the pancreas are asymptomatic for a long time. Gastroenterologists at the Yusupov Hospital often find them by chance during an examination of a patient for a disease of the digestive system.
Doctors take an individual approach to treating patients. In the absence of tumor symptoms and signs of malignancy, patients are actively monitored using the latest laboratory and instrumental research methods. If a benign tumor rapidly increases in size, compresses the pancreatic ducts, or has signs of malignancy, combined treatment is performed. Surgeons masterfully perform all surgical interventions on the pancreas. Medical staff provides professional care for patients.
Causes of benign tumors of the pancreas
The causes of benign pancreatic tumors have not been established. They are believed to develop under the influence of the following factors:
- Genetic pathology predisposing to neoplastic processes;
- Unfavorable environmental conditions;
- Smoking tobacco;
- Alcohol abuse.
A large role in the development of benign tumors of the pancreas is played by inflammatory processes in the organ, primarily chronic pancreatitis. Risk factors for the development of benign tumors include poor nutrition - a predominance of fatty foods, mainly of animal origin, in the diet, lack of proteins, fiber, vitamins, and improper diet (overeating, lack of regular meals).
Prognosis and prevention
How long patients live depends on the nature, location and stage of the cancer. In the case of a malignant tumor, the prognosis is often disappointing - in the majority of cases, the life expectancy of such patients does not exceed six months. In some cases of the disease, with timely diagnosis and treatment, patients can live from five to ten years. When this disease is detected, patients must strictly adhere to all prescriptions and recommendations of the attending physician.
There are no specific preventive measures to prevent the development and formation of such tumors. However, you can reduce the risk of tumor formation if you adhere to a proper diet, lead an active lifestyle and carry out timely treatment for pancreatitis.
Symptoms of benign pancreatic tumors
Symptoms of benign pancreatic tumors are determined by the type of tumor. Hormonally inactive neoplasms are usually a diagnostic finding. They do not manifest any symptoms until they reach a significant size and compress neighboring organs, stretch the pancreatic capsule or impair blood flow. Doctors usually detect such neoplasms during instrumental diagnostics of other diseases.
They are distinguished from malignant tumors by the following characteristics: absence of clinical symptoms (including manifestations of intoxication syndrome - fatigue, weakness, nausea, decreased appetite, low-grade body temperature), slow growth with normal levels of tumor markers in the blood.
When a large benign tumor of the pancreas compresses neighboring organs, pain is possible. Patients complain of constant, aching pain that intensifies with changes in body position. Their localization depends on the location of the benign formation.
Tumors of the head of the pancreas manifest themselves as pain in the right hypochondrium and epigastric region, the body of the organ - in the upper abdomen, the tail - in the lumbar region and left hypochondrium. The mass may compress the pancreatic or common bile ducts. In this case, signs of obstructive jaundice appear:
- Icterus (yellowness) of the sclera and skin;
- Itching;
- The appearance of dark colored urine;
- Discoloration of stool.
If any part of the intestine is compressed, intestinal obstruction may develop.
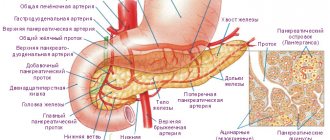
Hormone-producing benign tumors of the pancreas have specific symptoms. They are determined by the secreted hormone. Insulomas produce insulin. This hormone affects blood glucose levels. Gastrinoma (a gastrin-producing benign tumor of the pancreas, developing from cells of the islets of Langerhans) is manifested by the development of multiple ulcers of the stomach and duodenum, resistant to pharmacotherapy. Patients feel intense pain in the epigastric region. They are worried about sour belching and heartburn.
Due to excess gastrin production, a large amount of hydrochloric acid enters the lumen of the gastrointestinal tract. This leads to impaired intestinal motility, damage to its mucous membrane and deterioration of absorption processes.
Glucagonoma is manifested by symptoms of increased blood glucose levels:
- Significant weight loss;
- The appearance of necrolytic migratory erythema (red-brown rash on various parts of the body, mainly in the groin, thighs, buttocks);
- Peeling of the skin;
- Damage to the mucous membranes (gingivitis, stomatitis, vaginitis).
Diabetes mellitus may develop against the background of glucagonoma. Its distinctive features are the fairly rapid achievement of compensation and the rare development of ketoacidosis, nephropathy and angiopathy (damage to the kidneys and blood vessels).
Classification
Pancreatic cancer is classified according to the international TNM classification system for malignant neoplasms, where T is the size of the tumor, N is the presence of metastases in regional lymph nodes, and M is metastases in other organs.
However, in this case, the classification is not sufficiently informative regarding the operability of cancer and the prognosis of the effectiveness of therapy, since the general condition of the body plays a significant role in the prospect of cure.
- intraductal adenocarcinoma - the dominant structural form of pathology - glandular squamous cell carcinoma, undifferentiated (anaplastic) carcinoma, mucinous non-cystic carcinoma, signet ring cell carcinoma, mixed ductal endocrine carcinoma;
- acinar cell carcinoma;
- giant cell tumor;
- mucinous cystadenocarcinoma;
- intraductal papillary mucinous carcinoma;
- pancreatoblastoma;
- serous cystadenocarcinoma;
- solid pseudopapillary carcinoma;
- mixed carcinomas.
The glandular type of tumor (adenocarcinoma) is the most common. It originates in the head of the organ and comes from the bile ducts. The most common structural (histological) forms of pancreatic cancer and the features of their manifestation can be seen in Table 1. Table 1
| Tumor type | Features of the flow |
| Ductal adenocarcinoma | Absolutely predominates, accounting for 95% of neoplasms among exocrine tumors. It is characterized by a specific aggressive course according to a specific algorithm:
|
| Osteoclast-like giant cell tumor | Rare tumor. People aged 60–70 years are affected. It can be combined with mucinous cystadenoma or cystadenocarcinoma, as well as with ductal adenocarcinoma. They look like tumor nodes with a diameter of up to 7 cm and have clear contours. Microscopically, the cells are represented by undifferentiated cancer - atypical cells, when it is impossible to determine which tissue was the source of the tumor. |
| Serous cystadenocarcinoma | The cells produce serous fluid. A large number of glycogen granules, a polysaccharide formed by glucose residues, accumulate in tumor cells. The neoplasm can grow large, more than 10 cm. It is characterized by germination into adjacent tissues and the formation of metastases. |
| Mucinous cystadenocarcinoma | It appears more often in women and is located in the tail and body of the organ. Malignant cells produce mucous secretion (mucin) and dense connective tissue - stroma. |
| Intraductal papillary mucinous invasive carcinoma | Cystic tumor with high malignant potential. It affects the pancreatic duct or its branches. It is characterized by segmental or diffuse expansion of the pancreas ductal system, in which there is a proliferation of cells that produce mucin. Papillae form on the surface of the epithelium, which can be microscopic in shape or form large nodular masses. |
| Acinar cell carcinoma | The neoplasm contains gland enzymes - amylase, lipase, trypsin, and cytokeratin proteins. Among tumor cells there are endocrine cells and pancreatic hormones. |
| Pancreatoblastoma | The tumor practically does not occur in adults; it is typical for children under 15 years of age. With surgical removal, the oncological prognosis is more or less favorable. |
Neoplasms in the pancreas are most often discovered at a late stage. Therefore, the following classification is often used in medical practice:
- Operable tumor of the pancreas. The tumor affected only the gland or spread, but did not affect vital veins and arteries. There are no secondary lesions in distant organs. At this stage, the percentage of detection of pathology is low - in 10 - 15% of cases.
- Locally advanced pancreatic tumor. Malignancy has spread to adjacent tissues and organs, but is limited. It is no longer possible to remove the formation, since it has grown into the blood vessels passing nearby, into neighboring organs. There are no secondary tumor foci (metastases). Locally advanced tumor is detected in 35–40% of cases.
- Metastatic tumor of the pancreas. Malignant cells have expanded beyond the organ area. There are metastases. This prevalence is found in half of the observations.
Quite often, adjacent organs - secondary tumors - metastasize to the pancreas. The primary focus “matures” in the kidneys, colon, and lungs.
Functional neuroendocrine tumors are more often diagnosed: gastrinoma (gastrin-producing neoplasia of the pancreas from the cells of the islets of Langerhans), insulinoma, glucagonoma. Despite the fact that such formations are usually small in size and not prone to rapid growth, their manifestations are very specific, since the cells of the neoplasms produce hormones that enter the systemic circulation.
Benign neoplasia of the pancreas also includes hemangioma (a formation with a vascular structure), fibroma (from connective tissue), lipoma (from adipose tissue), leiomyoma (a formation from muscle fibers), neuroma or schwannoma (a neoplasm from Schwann cells that are located in nerve sheaths). These types of tumors are characterized by the absence of clinical manifestations until they reach a significant size.
Diagnosis of benign pancreatic tumors
Doctors at the Yusupov Hospital make a final diagnosis based on the characteristic clinical picture of some benign tumors and the results of instrumental and histological research methods. A consultation with a gastroenterologist allows you to guess the type of tumor, find out how long ago the symptoms appeared and whether they are progressing.
A biochemical blood test in the case of glucagonoma and insulinoma confirms changes in blood glucose levels. Tumor markers must be determined: carcinoembryonic antigen, CA 19-9. Their level in the case of a benign nature of the disease is not increased.
The most informative methods for diagnosing benign pancreatic tumors in gastroenterology are instrumental studies. Doctors at the Yusupov Hospital perform an ultrasound examination of the abdominal organs to visualize the formation, determine the size of the tumor, and the condition of the regional lymph nodes. Highly informative research methods are magnetic resonance and computed tomography. They can detect small benign pancreatic tumors.
To identify benign pancreatic tumors with multiple foci, scintigraphy is performed at the Yusupov Hospital. Radioactive drugs are introduced into the body, which are actively accumulated by tumor cells. Their radiation is recorded in the image. If a pancreatic hemangioma is suspected, doctors perform angiography to assess the blood flow in the formation and its relationship with the systemic blood flow. In order to study the histological structure of the neoplasm and differentiate it from malignant tumors, surgeons perform a puncture biopsy of the pancreas, followed by a morphological examination of the biomaterial.
Treatment of benign pancreatic tumors
Treatment of benign pancreatic tumors is only surgical. Surgeons at the Yusupov Hospital perform enucleation (enucleation) of the tumor. Resection of the head of the gland or tail is performed if there is a tumor in the corresponding part of the organ. If a large tumor is located in the area of the head of the gland and causes a violation of the outflow of bile, pancreaticoduodenectomy is performed - the tumor is removed along with part of the gland and the duodenum). An effective method of treating pancreatic hemangioma is selective arterial embolization - blocking the blood supply to the space-occupying lesion.
In cases where radical surgery cannot be performed for multiple hormone-producing benign tumors of the pancreas, doctors at the Yusupov Hospital provide symptomatic treatment. For insulinoma and glucagonoma, endocrinologists prescribe medications to normalize blood glucose levels. With the development of episodes of hypoglycemia and hyperglycemia, appropriate correction is carried out with glucose or insulin solutions.
Diet therapy must be prescribed. The cooks at the Yusupov Hospital prepare dietary meals from high-quality ingredients. Their organoleptic properties are no different from home cooking.
When treating gastrinoma, drugs are used that suppress gastric hypersecretion (ranitidine, omeprazole, famotidine). In severe cases, surgeons perform excision of the gastrinoma with gastrectomy (to prevent relapses due to incomplete removal of the tumor).
Pancreatic adenoma
Serous cystadenomas of the pancreas can occur at any age, but are more common in older people. They are mostly asymptomatic. If the tumor is located in the head of the pancreas, it may interfere with the flow of bile.
The average diameter of serous neoplasms is about four centimeters. They are found in the body of the pancreas. The tumor has the appearance of a circumscribed and well differentiated from the surrounding tissues of the pancreas. Serous benign tumors of the pancreas are partially encapsulated, the lobules consist of countless small cysts. In larger pancreatic adenomas, calcifications can be seen.
Benign adenomas of the endocrine pancreas are much less common than other pancreatic tumors. About 60% of all pancreatic endocrine tumors secrete insulin. This is manifested by hypoglycemia syndrome:
- Increased sweating;
- Trembling;
- Attacks of severe weakness;
- Periodic loss of consciousness.
Most often, adenomas occur in the tail and body of the pancreas. They are located under the capsule. The size of the formations can range from a few millimeters to 3-6 cm in diameter. The tumor is round in shape, covered with a thin capsule. The consistency of the neoplasms can be dense or soft.
The following variants of the microscopic structure of pancreatic adenomas formed from islet cells are distinguished:
- Parenchymal (tubular, solid, trabecular, cribriform, adenomatous, pericytic);
- Fibrous (with hyalinosis or amyloidosis);
- Angiomatous;
- Mixed.
Based on the nature of the hormone produced, pancreatic adenomas are divided into 3 groups:
- Orthoendocrine - secrete hormones that are characteristic of the physiological function of the islets (insulinoma, glucagonoma);
- Paraendocrine - produce hormones, both characteristic and unusual for normal endocrine cells (corticotropinoma, gastrinoma, VIPoma, melanocyte-stimulating neoplasms);
- Polyendocrine - their cells simultaneously produce several hormones.
Doctors at the Yusupov Hospital determine the location of the adenoma in the pancreas using angiography, echography and computed tomography. For small benign tumors, surgeons perform enucleation. If the tumor is large or multiple tumors are suspected, part of the pancreas is resected. If you suspect a benign tumor of the pancreas, make an appointment with a gastroenterologist by phone.
Author
Natalya Aleksandrovna Vyaznikova
Oncologist
General information
The concept of “pancreatic cancer” includes a group of malignant neoplasms that develop in the parenchyma of the pancreas: the head, body and tail.
The main clinical manifestations of these diseases are abdominal pain, anorexia, weight loss, general weakness, and jaundice. Every year, 8-10 people out of every hundred thousand people in the world develop pancreatic cancer. In more than half of cases, it occurs in elderly people (63% of patients diagnosed with pancreatic cancer are over 70 years of age). Men are more prone to this type of malignancy; they develop pancreatic cancer one and a half times more often. A malignant tumor of the pancreas is prone to metastasis to regional lymph nodes, lungs and liver. Direct tumor growth can lead to its penetration into the duodenum, stomach, and adjacent parts of the large intestine.
Pancreas cancer
Benign pancreatic tumors are a rare pathology. Neoplasia occurs with a frequency of 1-3 cases per 1 million population. They primarily affect middle-aged and older people. They can be single or multiple, located in the tail, body or head of the organ. Small hormonally inactive tumors are usually asymptomatic and become an incidental finding during examination for other diseases. Hormonally active neoplasms are characterized by specific changes in the endocrine background.
Benign pancreatic tumors
Bibliography
- ICD-10 (International Classification of Diseases)
- Yusupov Hospital
- Cherenkov V. G. Clinical oncology. — 3rd ed. - M.: Medical book, 2010. - 434 p. — ISBN 978-5-91894-002-0.
- Shirokorad V.I., Makhson A.N., Yadykov O.A. The state of oncourological care in Moscow // Oncourology. - 2013. - No. 4. - P. 10-13.
- Volosyanko M.I. Traditional and natural methods of preventing and treating cancer, Aquarium, 1994
- John Niederhuber, James Armitage, James Doroshow, Michael Kastan, Joel Tepper Abeloff's Clinical Oncology - 5th Edition, eMEDICAL BOOKS, 2013