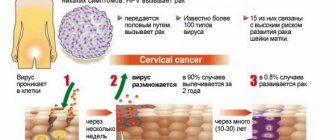
Adenovirus infection is one of the infectious pathologies included in the group of acute respiratory viral infections (ARVI). The ARVI group includes influenza, adenoviral infection, parainfluenza, MS infection, etc. This is one of the most common groups of infectious pathologies worldwide.
The clinical manifestation of adenovirus infection is determined by the serotype of the adenovirus. From the point of view of DNA structure, the human adenovirus has 3 antigens:
- group A antigen, which is common to all serotypes,
- toxic B-antigen, which suppresses interferon activity,
- a type-specific C-antigen that can affect the epithelium of the respiratory tract, conjunctiva, intestines, as well as lymphoid tissue.
Adenovirus is transmitted by airborne droplets. Affects the pharynx, tonsils, conjunctiva. The lesion also manifests itself as lymphadenopathy and fever.
What is adenovirus infection
This group of infections includes acute viral pathologies that develop as a result of adenoviruses entering the body.
For reference. Adenovirus infection is less common in adults than in children.
However, children in the first six months of life rarely suffer from this disease. This is due to the presence of maternal specific antibodies (passive types of immunity). After 6 months of life, passive immunity weakens, and the child becomes highly susceptible to adenoviruses. The maximum incidence rate is recorded from six months to seven years.
After seven years, the incidence of adenoviruses decreases, as patients develop natural acquired immune responses. However, since immunity is type-specific, when infected with another serotype of the virus, an adenoviral infection develops again.
Code for adenoviral infection according to ICD10:
- B34.0 – for unspecified forms of the disease;
- A85.1 – for adenoviral encephalitis;
- A87.1 – for adenoviral meningitis;
- B30.1 and B30.0 – adenovirus infection of the eyes (conjunctivitis and keratoconjunctivitis);
- J12.0 – for adenoviral pneumonia.
Transfer methods
Adenovirus infection in children and adults is transmitted in several ways. Among them:
- Airborne droplet route. In this situation, the patient secretes viruses along with nasopharyngeal mucus. Microorganisms can enter the respiratory tract of a healthy person after ordinary contact. This route of infection is typical at the early stage of the disease.
- Fecal mode of transmission. In the later stages of the disease, adenoviruses leave the body along with feces. This method is found in those people who do not adhere to the rules of personal hygiene.
- Water route of infection. Adenoviruses live in aquatic environments. They can become infected when swimming in a pool (if disinfection rules have not been followed).
Viruses enter the mucous membranes of the body, reach the lymph nodes, infect cells and synthesize their DNA in their nuclei. After the end of the incubation period, pathogens enter the bloodstream and spread throughout the body. This leads to damage to the mucous membranes of the nasopharynx, lungs, bronchi, tonsils, even the conjunctiva of the eyes. The course of adenovirus infection in children can be mild, moderate or severe.
Etiological factors of adenoviral infection
Adenovirus is a deoxyribonucleic virus. It has a high level of sustainability in the environment. Also, the pathogen is not destroyed when treated with organic solvents.
Attention. Adenovirus is capable of maintaining high levels of activity for 2-3 weeks in fresh water, drug solutions, and household items.
When exposed to temperatures above fifty-six degrees, the adenovirus is destroyed within half an hour, and the virus is also destroyed under the influence of ultraviolet radiation and disinfectants containing chlorine.
The main specific feature of adenoviruses is their high tropism for epithelial cells of the respiratory tract, lymphoid tissues, as well as mucous membranes of the eyes and intestines.
Antigens produced by the causative agent of adenovirus infection are able to suppress interferon activity and have a cytopathic effect on tissues, helping to maintain the inflammatory process.
Attention. Some serotypes of adenovirus infection are capable of causing a chronic inflammatory process (latent course of adenovirus infection in the form of chronic tonsillitis or adenoiditis).
It should also be noted that the clinical picture of adenovirus infection is largely determined by the serotype of adenovirus that caused the inflammatory process.
The third type of adenovirus causes predominantly adenoviral pneumonia, conjunctivitis and mesadenitis, the eighth type of virus – epidemic keratoconjunctivitis, the ninth type – enteritis, etc.
How is adenovirus infection transmitted?
For reference. The sources of pathogens are patients with acute or latent forms of the disease.
The release of viral particles occurs with mucus, during coughing, sneezing, etc. In the later stages of the disease, the adenovirus is actively excreted in the feces.
Infection with adenovirus infection occurs primarily through airborne droplets and fecal-oral routes (through household and personal hygiene items).
Epidemic keratoconjunctivitis can also be transmitted by using eye drops on an infected patient.
Due to the high volatility of the pathogen, transmission of the virus is most often carried out by airborne droplets.
The peak incidence is recorded in summer and autumn.
Symptoms
In children and adults, the symptoms of adenovirus infection appear approximately the same. The disease is characterized by:
- headache;
- cough;
- dyspnea;
- pain and pain in the eyes, inflammation, copious mucous discharge;
- intoxication of the body;
- pharyngoconjunctival fever;
- chills;
- diarrhea;
- discomfort in the navel area (mostly paroxysmal pain);
- aching pain in the bones (in the right iliac region);
- swelling of the nasolabial sinuses;
- increased body temperature;
- enlarged lymph nodes;
- conjunctivitis.
In infants, convulsions may develop against the background of fever, the attacks of which must be stopped immediately in order to avoid complications. At this age, the symptomatic picture is not very pronounced, so intestinal dysfunction and elevated body temperature may indicate the need to show the child to a specialist.
Laryngopharyngotracheitis
As the infection progresses, laryngopharyngotracheitis or damage to the larynx up to the bronchi begins. It is characterized by: a dry “barking” cough, constant wheezing on inhalation and exhalation, cyanosis of the nasolabial triangle, shortness of breath and hoarseness of voice. If treatment is not started in time, the primary disease will develop into persistent bronchitis, sometimes of the chronic type.
Adenoviral eye infection
Adenovirus eye infection can be caused by different types of adenovirus virus. The disease is transmitted by airborne droplets or by failure to comply with personal hygiene rules. The main signs of the presence of adenovirus infection are:
- intolerance to bright sunlight;
- profuse lacrimation;
- redness of the mucous membrane of the eyes;
- itching, burning;
- sensation that there is a foreign body in the eye.
An adenoviral infection of the eye affects one visual organ, and soon (in the absence of proper treatment) provokes the development of complications. The most common of these are bacterial or allergic conjunctivitis and dry eye syndrome. The disease often develops into a stagnant chronic form, which will be much more difficult to cure completely.
- Viral diseases - symptoms, diagnosis and treatment
- Main clinical symptoms and syndromes of infectious diseases
- How to treat ARVI in children
Rash
A symptom such as vomiting due to an adenovirus infection manifests itself mainly in infants. Initially, the rash affects the face, gradually spreading throughout the body. The rash goes away within a few weeks and if the inflammation is not subjected to mechanical stress, no traces remain. Hydrocortisone ointment, which has an anti-inflammatory effect, will help speed up the disappearance of adenoviral papules. An alternative to it is prednisolone ointment, which gives a similar result, but is based on a different active ingredient.
Pneumonia
Acute adenoviral pneumonia involves the progression of an infection of the same name in the patient’s body, to which secondary bacterial flora joins. The pathogen has more than 40 varieties that affect patients of different age groups. The disease is worst experienced by children under 5 years of age due to the lack of immunity. This type of pneumonia is transmitted by airborne droplets and the fecal-oral route.
Sore throat and conjunctivitis at the same time
Viral sore throat and conjunctivitis at the same time occur very often if the respiratory tract disease is provoked by an adenovirus. Here it is important to address the problem comprehensively, eliminating not only the symptomatic picture, but also the pathogen itself. Polyionic crystalloid solutions, antihistamines and antibiotics, taken according to a regimen strictly determined by the doctor, are excellent for these purposes. Otherwise, there is a high probability that conjunctivitis will become chronic.
Acute rhinopharyngotonsillitis
Clinically, acute upper rhinopharyngotonsillitis of a bacterial nature is practically no different from its viral equivalent. A throat swab will help accurately diagnose the form. Its results will allow you to form a clinical picture and prescribe effective treatment to the patient. The incubation period lasts from 1 day to two weeks, after which the disease manifests itself fully.
Pathogenesis of the infectious process
The clinical picture of the disease is determined by the specific effect of the virus on epithelial and lymphoid tissue. The infectious process is manifested by the development of local inflammatory reactions in the mucous membranes of the respiratory tract, hyperplasia of lymphoid tissues, intoxication and febrile symptoms.
For reference. The mucous membrane lining the respiratory tract acts as an entrance gate for pathogens of the infectious process. Less commonly, the entry points for adenoviruses are the mucous membranes of the conjunctiva and the gastrointestinal tract.
Reproduction of viral particles begins almost immediately after its introduction. One day after infection, the multiplication of viral particles in cells reaches a maximum.
In this regard, the incubation period of an adenoviral infection can range from two to twelve days (most often from five to seven days).
After the initial reproduction of viruses in cells, they enter the blood and a period of viremia begins (the virus has already entered the blood and begins to spread in the body), lasting up to ten days.
For reference. During viremia, damage to the vascular endothelium occurs, leading to the development of exudative inflammatory processes in the mucous membranes and the appearance of fibrin deposits on the surface of the mucous membranes (plaques).
Plaques on the mucous membranes of the tonsils, posterior pharyngeal wall, conjunctivae, etc. are filmy in nature (due to the production of thrombokinases against the background of necrotic damage to epithelial cells).
When adenoviruses penetrate the lungs, adenoviral pneumonia can develop.
Attention. Due to the constant ingestion of mucus containing viruses, the adenovirus enters the gastrointestinal tract. Viruses also begin to actively multiply in the small intestine.
Due to the fact that viruses circulate and multiply in the gastrointestinal tract longer than in the respiratory tract, the development of adenoviral mesadenitis and temporary degenerative changes in the tissues of the liver and spleen can occur.
Some types of adenovirus infection pathogens are capable of long-term persistence in lymphoid tissues, contributing to the development of chronic infections.
Clinical forms of the disease
Most often, the inflammatory process occurs in the form of:
- pharyngoconjunctival fever;
- tonsillopharyngitis;
- catarrh of the upper respiratory tract (upper respiratory tract);
- keratoconjunctivitis;
- enteritis;
- lymphadenopathies;
- meningitis and encephalitis (in rare cases).
What are adenoviruses?
Adenoviruses are viruses whose genome consists of double-stranded DNA. They belong to the genus Mastadenoviruses (lat. Mastadenovirus). Adenoviruses show high resistance to environmental factors. To date, 51 serotypes of adenoviruses have been identified, but only a third of them are pathogenic for humans. Some serotypes have been shown to be oncogenic in rodents, but no association has yet been demonstrated between adenoviruses and their transformation into tumors in humans.
Research is currently underway on the use of adenoviruses as a DNA vector in gene therapy. Adenoviral infections affect the respiratory, digestive and visual systems. They can be especially dangerous for newborns and people with weakened immune systems. Infection usually occurs by droplet or fecal-oral route. The reservoir of the virus is humans.
Places such as kindergartens, nurseries, boarding schools, hospitals and military barracks contribute to the spread of infection.
Conjunctival infection (conjunctivitis) may occur from contact with sick people's towels, contact lenses, or swimming pools. Remaining an infection on a particular serotype of a virus creates permanent resistance to that particular serotype (but not to others).
Infection occurs through the mucous membranes of the respiratory tract, gastrointestinal tract, conjunctiva and cornea.
Adenoviruses also have a special affinity for lymphoid tissue, and infiltrates of lymphocytes form in infected tissues and organs.
Adenoviral infection - symptoms
For reference. The main symptoms of adenoviral infection are the development of intoxication and febrile symptoms, damage to the mucous membranes lining the respiratory tract and gastrointestinal tract, the development of adenoviral conjunctivitis , as well as damage to lymphoid tissues.
The onset of adenoviral infection is always acute. Leading syndromes of the disease
are:
- intoxication symptoms;
- catarrhal symptoms;
- damage to lymphoid structures;
- gastrointestinal tract damage.
The first manifestations of the infectious process are intoxication, febrile and catarrhal symptoms.
Patients are concerned about headaches, severe lethargy and weakness, arthralgia and myalgia (joint and muscle pain). Some patients also experience vomiting and nausea.
For reference. The maximum increase in temperature during adenoviral infection is observed on the second or third day of illness. The elevated temperature can persist for up to five to ten days of illness. In rare cases, low-grade fever can persist for a month in the form of a two-wave, less often three-wave fever.
Due to the high level of tropism of the causative agent of adenoviral infection to lymphoid tissues, symptoms of damage to the lymphatic system develop from the first days of the disease.
Damage to the nasopharyngeal tonsils is accompanied by severe difficulty in nasal breathing, nasal congestion, a characteristic nasal voice, puffiness of the face, and the appearance of adenoviral pharyngitis.
Patients are concerned about moderate sore throat and sore throat. Symptoms of rhinitis are also common.
For reference. When examining the mucous membrane of the posterior pharyngeal wall, congestive hyperemia, swelling and granularity (due to hyperplasia of lymphoid elements) of the mucosa are revealed. The tonsils are swollen and enlarged. Often thin, filmy, whitish deposits are found on the tonsils, which can be easily removed with a spatula.
A common symptom of the disease is a wet cough with copious non-purulent sputum (clear, viscous sputum without an unpleasant odor).
A characteristic symptom of the disease is enlarged lymph nodes (submandibular and cervical). There may also be an increase in mediastinal and mesenteric lymph nodes.
A severe course of the infectious process may be accompanied by the development of adenoviral mesadenitis. This condition is manifested by abdominal pain, vomiting and diarrhea. Sometimes symptoms of peritoneal irritation may be observed (in this case, acute appendicitis may be suspected).
Clinic of the disease in children
Adenoviral infection in children is manifested by the following symptoms:
- Intoxication syndrome. The child is often capricious, becomes restless, sleeps poorly, often spits up, his appetite worsens, intestinal colic and diarrhea occur.
- Breathing through the nose becomes difficult , pharyngitis, tracheitis, and tonsillitis develop. At the beginning of the disease, nasal discharge is serous in nature, and then thickens and becomes mucopurulent.
- Symptoms of pharyngitis are pain and sore throat, coughing. The tonsils hypertrophy and extend beyond the palatine arches, which become red and swollen. On the hyperemic back wall of the pharynx, bright red lesions appear, covered with mucus or whitish deposits.
- Bronchitis develops when a bacterial infection occurs. It manifests itself as a dry, persistent cough, which greatly worries the baby. After some time, the cough becomes moist and sputum appears.
- Conjunctivitis is a common sign of the disease, which appears by the 5th day of illness. Children are bothered by pain and burning in the eyes, pain, tearing, a feeling of obstruction, and itching. The mucous membrane of the eye turns red and swells, the eyelashes stick together, and crusts appear on them, which are dried discharge from the inflamed conjunctiva.
- It is possible to develop gastroenteritis , as well as the spread of infection to the urinary tract, which is manifested by a burning sensation when urinating and the appearance of blood in the urine.
A sick child has a typical appearance: pasty face, swollen and hyperemic eyelids, narrowed palpebral fissure. On palpation, mobile and enlarged lymph nodes are detected. For young children, bowel dysfunction is common - diarrhea.
In infants, the disease develops extremely rarely, which is due to the presence of passive immunity. If infection does occur, the disease is severe, especially in children with perinatal pathology. In patients, after the addition of a bacterial infection, signs of respiratory failure appear. This can be fatal.
Based on severity, there are three forms of adenoviral infection:
- Mild - with a temperature of less than 38.5°C and intoxication.
- Moderately severe – with a temperature of up to 40°C without intoxication.
- Severe - with the development of complications: inflammation of the bronchi or lungs, keratoconjunctivitis.
Complications of the pathology in children are inflammation of the middle ear, croup, bronchitis, pneumonia, encephalitis, dysfunction of the cardiovascular system, maculopapular rash on the skin.
Diagnostics
The diagnosis is made based on the clinical picture of the disease:
- history characteristic of a viral infection,
- the onset is acute, with a further expansion of the observed symptoms (polymorphism),
- the presence of catarrhal syndrome in a pronounced form,
- presence of intoxication syndrome,
- inflammation is exudative in nature (profuse nasal discharge),
- inflammation in the conjunctiva.
To detect adenovirus antigens, immunofluorescent as well as enzyme immunoassay methods for studying epithelial cells can be used.
To clarify the types of ARVI, indirect hemadsorption, ELISA, etc. can be used.
The data from a general blood test will be indicative:
- moderate leukocytosis in the first days (sometimes),
- shift in neutrophil formula,
- presence of atypical mononuclear cells (5 – 10%%),
- leukopenia and lymphocytosis (on the 2nd – 3rd day).
Unfortunately, most patients do not bother to clarify the diagnosis. The vast majority do not do a full examination. And they immediately start taking antibiotics.
Diagnostics and differential diagnostics
Recognition of adenoviral infection is usually made on the basis of clinical data: fever, catarrh of the respiratory tract, conjunctivitis, polyadenitis, and the sequential development of symptoms. Immunofluorescence reaction and immune electron microscopy are methods for rapid diagnosis of adenovirus infection. Retrospective confirmation of the etiological diagnosis is carried out using ELISA, X-ray, and RSK methods. Virological diagnosis involves isolating adenovirus from nasopharyngeal swabs, scrapings from the conjunctiva and feces of the patient, but due to its complexity and duration it is rarely used in clinical practice.
Differential diagnosis of various clinical forms of adenoviral infection is carried out with influenza, other acute respiratory viral infections, diphtheria of the pharynx and eyes, infectious mononucleosis, mycoplasma infection, yersiniosis. For this purpose, as well as to prescribe local etiotropic treatment, patients need consultation with an ophthalmologist and otolaryngologist.
Adenovirus infection - treatment
Treatment of adenovirus can be carried out at home. Children with obstructive symptoms, patients with severe infectious process, patients with complicated forms of the disease (mesadenitis, meningitis, etc.) are subject to hospitalization.
During periods of febrile and severe intoxication symptoms, bed rest is indicated.
For moderate and severe disease, the use of interferon drugs, arbidol, vitamin therapy, etc. is indicated. According to indications, nasal and eye drops with interferons can be used.
Attention. Antibiotics are not used for pure viral infections. The use of antibiotics is justified only when secondary bacterial flora is attached (complicated forms of adenoviral infection).
Treatment
Adenoviral infection must be treated under the supervision of a doctor, especially if we are talking about a disease in a child. Choosing the wrong medications can do more harm than good.
Medication
Treatment of adenoviral diseases in most cases is symptomatic, and in an uncomplicated process, the prescription of antibiotics is not necessary.
Main goals of therapy:
- normalization of body temperature (if the temperature rises > 38.5 ° C, antipyretic drugs are indicated, such as Paracetamol, Ibuprofen);
- fight against cough - for wet cough, mucolytics and expectorants (Ambroxol, Mucaltin, Bromhexine, ACC) are recommended, both orally (syrups, tablets) and inhalation. Antitussive drugs are prescribed only in case of prolonged dry cough;
- treatment of conjunctivitis - use furatsilin solution, oxolinic ointment, eye drops (Ophthalmoferon, Levomycetin);
- fight against a runny nose - for nasal congestion, saline solution or sea water is prescribed, vasodilators are also used (Nazivin, Otrivin, etc.);
- strengthening the body - vitamin and mineral complexes;
- restoration of microflora (Bifiform).
If complications develop or there is a high risk of their occurrence, antibiotic therapy is prescribed. Etiotropic therapy (aimed at eliminating the root cause of the disease), including drugs such as Viferon, Cycloferon and Isoprinosine, which kill the virus, is also widely used.
The main drugs to combat adenovirus - table
| Product name | Drug group | Mechanism of action | Release form and age at which the drug is used | Contraindications |
| Viferon | Antiviral, immunomodulatory. | Contains interferon (stops the proliferation of viruses), vitamin C and vitamin E (increase the effectiveness of interferon, have an antioxidant effect). | Available in the form of suppositories. Prescribed from the newborn period, including premature babies with a gestational age of more than 34 weeks. | Hypersensitivity to the components of the drug. |
| Isoprinosine | Antiviral, immunomodulatory. | Damages the genetic apparatus of viruses, suppressing their reproduction | Available in tablets. Prescribed for children over three years of age. |
|
| Enterofuril | Antimicrobial drug. | Suppresses the activity of viruses. | Available in capsules - for children over two years of age and adults, as well as in the form of a suspension for children from one month to two years. |
|
| Paracetamol | Antipyretic, analgesic drug. | Inhibits the excitability of the thermoregulation center, reduces the level of prostaglandins and inflammatory mediators. | Available in the form of tablets, capsules, powder, oral solution, suppositories, suspensions. Prescribed to children from the first month of life. |
Prescribed with caution when:
|
| Ambroxol | Expectorant mucolytic drug. | Stimulates secretion in the bronchi, increases the amount of mucous secretion. | Available in the form of tablets, syrup, solution for oral administration/infusion/inhalation. There are no age restrictions. |
Prescribed with caution in renal failure |
| Oftalmoferon | Eye drops. | The drug contains interferon, which has an antiviral and antihistamine effect, which reduces itching, inflammation, and swelling. | Available in drops. There are no age restrictions. | Intolerance to the components of the drug. |
Drugs for adenovirus infection - photo gallery
Viferon is an effective immunomodulatory and antiviral drug
Kipferon is used for adenovirus
Isoprinosine is an effective and modern antiviral drug
Cycloferon is an antiviral drug
Traditional medicine methods
Traditional methods are widely used in the treatment of adenoviral diseases. So, for a dry cough, it is advised to take breast milk, drink hot milk with a pinch of soda, teas with viburnum, raspberries, elderberries, linden, and chamomile.
There are also many recipes for preparing decoctions to combat adenoviruses, the most common are the following:
- Pour a glass of unpeeled oats with boiled milk (5 glasses) and cook for about an hour. Strain, add 1-2 tablespoons of honey, cool and drink in small portions throughout the day.
- Boil finely chopped turnips for about 15 minutes in boiled water, leave the broth for an hour, then strain and drink ¼ cup 3-4 times a day.
- Mix finely chopped onion (150 g), honey (25 g), sugar (200 g). Pour the mixture with warm water and cook over low heat for about an hour. Then pour into a dark bowl. Take a teaspoon 7 times a day. Store in a cool place.
- Mix two egg yolks, two tablespoons of butter, a teaspoon of flour and two teaspoons of honey. Take one tablespoon 5 times a day.
- Mix anise seeds with honey, add salt, cook over low heat, then strain and take one tablespoon four times a day.
Folk remedies for adenovirus - photo gallery
Oat decoction
Turnip
Raspberry tea
Prevention of adenovirus infection
Preventive measures for adenoviral infections consist of increasing the level of nonspecific resistance of the immune system (routine vitamin therapy, balanced nutrition, etc.).
It is also recommended to avoid hypothermia and contact with patients infected with adenovirus infection. When outbreaks of adenoviral infection are detected in children's groups, children are separated for ten days from the moment the last patient is identified.
For reference. To prevent massive outbreaks of infection, all contacts with the patient are prescribed interferon drugs or interferon inducers according to standard preventive regimens.
Prevention
A specific vaccine has not yet been developed.
During seasonal outbreaks, you should visit crowded places (including public transport) with your child as little as possible. The baby needs general strengthening of the body, which involves hardening and proper nutrition.
During the cold season, additional intake of multivitamin complexes can be recommended. The child must be taught to strictly observe the rules of personal hygiene.
A good prophylactic agent is leukocyte interferon (diluted with water and instilled into the nasal passages).
To get more information about the treatment of infectious diseases in children, in particular, about the treatment of adenovirus infection, we recommend watching this video review - Dr. Komarovsky gives advice to parents:
Chumachenko Olga, pediatrician
51, total, today
( 45 votes, average: 4.11 out of 5)
Flu shots: truth and myths
Hepatitis B vaccination: timing of vaccination, indications, complications
Related Posts
Clinical recommendations (treatment protocol) for adenovirus infection in children
This document was developed and introduced by the Federal State Budgetary Institution "Research Institute of Influenza" of the Ministry of Health of the Russian Federation, Federal State Budgetary Institution Scientific Research Institute of Influenza, Federal Medical and Biological Agency of Russia. Approved at a meeting of the Profile Commission on October 9, 2013. Its full name is “Clinical recommendations (treatment protocol) for providing medical care to children with adenovirus infection.”
When treating adenovirus in children, a regime, diet, as well as medications (medicines of etiotropic and symptomatic therapy, immunotherapy and immunocorrection) and non-medicinal methods (antipyretics, physiotherapeutic methods of treatment, sanitation of the nasal passages, room ventilation and hygiene procedures) are used.
The following drugs are used as immunomodulators: Interferon alfa, Meglumina acridone acetate, Tiloron, Anaferon, Arbidol. Children are prescribed ascorbic acid as an antioxidant, and paracetamol and ibuprofen as antipyretics.
For concomitant fungal infection with adenovirus, nystatin or fluconazole are used. For the purpose of detoxification and replenishment of electrolyte imbalances, dextrose, Meglumina sodium succinate, sodium chloride, potassium chloride and others are prescribed.
For intestinal damage with the development of enteritis or gastroenteritis, Probifor, Bifiform, Enterol, Acipol, Dioctahedral Smectite, Hydrolyzed Lignin, Pancreatin, Mezim-Forte, Creon are used. In the presence of catarrhal syndrome - Acetylcysteine, Ambroxol, Fenspiride, Codelac Broncho.
Consequences and complications
At any stage of adenoviral conjunctivitis, a secondary bacterial infection may occur, which will give impetus to the development of diseases such as pneumonia, tonsillitis or sinusitis. In this case, additional signs may appear, for example, intoxication, shortness of breath or fever.
With an advanced form of the disease, complications such as the formation of a cataract on the eyeball, clouding of the cornea, and sometimes the appearance of scars can be observed . Also, one of the consequences of adenoviral conjunctivitis can be dry eye syndrome, which requires the use of special eye drops. Often the disease can develop into otitis or adenoiditis.
Expert opinion
Ermolaeva Tatyana Borisovna
Ophthalmologist of the highest category, Candidate of Medical Sciences
The most severe consequence of the disease can be blindness.
Is it contagious?
The name of the disease contains the word “virus” (that is, one of the types of infection), which means that adenoviral conjunctivitis is considered a contagious disease . It is transmitted by airborne droplets, household, fecal-oral and waterborne routes, as well as through direct contact with a sick person.
If a patient sneezes or coughs in the presence of another person, then this will be enough for the disease to be transmitted to a healthy person. But the easiest way to become infected is considered to be dirty hands. A slight touch to the eye area with dirty hands that contain pathogens is enough to initiate the development of the disease.
4Adenoviral infection in adults. Symptoms
During the first 14 days, a person is a carrier of a viral infection and poses a danger to others.
For adults, symptoms such as weakness, headache, chills, aching joints, nasal congestion and runny nose are typical. The temperature often rises to 38-39 degrees, drops after a couple of days, but in case of complications it can last up to two weeks.
The tonsils become inflamed, possible loss of voice, shortness of breath, dry, tearing cough, which periodically becomes wet, which indicates the development of bronchitis.
In some cases, the functioning of the gastrointestinal tract is disrupted, the disorder manifests itself in the form of diarrhea. The infection affects the mucous membrane of the eye (hypothermia of the mucous membrane, conjunctivitis), the eyelid area swells, and sometimes the vessels of the eyeball burst.
Complications of the disease can include laryngospasms, disseminated intravascular coagulation syndrome, and toxic shock.
Adenovirus infection: what symptoms are observed in children, methods of treatment and prevention
Adenoviral infection is one of the types of ARVI. The causative agents are DNA viruses. Most often, the disease is diagnosed in children and adolescents. Outbreaks of the disease are most often recorded in the cold season. The infectious agent affects the mucous membranes of the respiratory system and intestines. Lymphoid tissue is often involved in the process. One of the rather characteristic symptoms is damage to the conjunctiva of the eyes, which is why this pathology is also called “pharyngoconjunctival fever.”
Important: the disease is characterized by seasonality, but individual cases are recorded year-round.
Adenovirus is most often spread by airborne droplets. Contact and nutritional transmission of the pathogen is also possible.
Clinical signs of the disease are varied, but the most common symptoms are sore throat, runny nose and fever, i.e. symptoms characteristic of ARVI.
The disease can be quite severe, especially in a small child (under 3 years old) with a weak immune system.
If your child develops acute symptoms, you should definitely contact your pediatrician. By self-medicating, you can only harm the patient. With adenovirus infection, quite serious complications cannot be ruled out.
Please note: do not be surprised if a child is diagnosed with ARVI several times during one autumn-winter season. This does not mean that he does not develop immunity. Diseases from the ARVI group can be caused by a wide variety of pathogens, and acquiring immunity to one of the strains of the influenza virus does not completely exclude infection with an adenovirus.
Source: https://okeydoc.ru/adenovirusnaya-infekciya-u-detej-simptomy-i-lechenie/
Causes
Adenoviruses (Adenovirosis) were discovered in 1953 in the laboratory of W. Rowe while studying the tissues of the palatine tonsils and adenoids. In 1954, researchers M. Hilleman and S. Werener isolated adenoviruses from patients with acute respiratory disease and atypical pneumonia. In 1957, the International Committee on Taxonomy of Viruses classified adenoviruses into the family Adenoviridae, consisting of two genera: Mastadenovirus (mammals) and Aviadenovirus (birds). Currently, the family includes about 130 viruses.
Etiology
Human adenoviruses are DNA viruses belonging to the family Adenoviridae, genus Mastadenovirus. The virus has a 12-gonal (icosahedral) shape, 70-90 nm in size, consists of proteins (87%) and carbohydrates (13%). Has three soluble antigens:
- A-antigen - group, common to all serotypes;
- B-antigen is toxic, causing a cytopathic effect in tissue culture, suppressing the activity of interferon;
- C-antigen is type-specific.
There are currently 49 known serotypes of human adenovirus (1-49). The antigenic structure is stable. Based on the level of oncogenicity (for newborn hamsters), hemagglutinating characteristics and pathogenicity for humans, they are divided into 7 subgroups (A, B, C, D, E, F, G).
Symptoms of adenovirus infection in manifest form are caused predominantly by epidemic serotypes (3, 4, 7, 14, 21) of subgroups B and E. Serotypes 1,2,5,6 of subgroup C cause persistent infection in the tonsils and adenoids. One serotype can cause the development of various clinical forms of adenoviral infection. However, some serotypes are isolated relatively constantly in certain clinical settings:
- 1 - 7, 14, 21 - for acute respiratory diseases;
- 1, 3, 4, 7 - viral pneumonia;
- 3, 7,10, 14, 19, 37 - conjunctivitis;
- 8 - epidemic keratoconjunctivitis;
- 9, 11, 31 - diarrhea;
- 40 and 41 - gastroenteritis;
- 1, 2, 3, 5 - mesadenitis.
Important properties of human adenoviruses are epitheliotropy and toxicity; they affect the epithelium of the respiratory tract and intestines, conjunctiva, and lymphoid tissue.
Adenovirus infection in children is relatively stable in the environment, persists for several weeks in water, medicinal solutions, on household items, and is resistant to ether. Viruses are destroyed at a temperature of +56° C for 30 minutes and die under the influence of ultraviolet irradiation and chlorine-containing drugs.
Adenoviruses are cultivated in a culture of human epithelial cells with the development of characteristic cytopathic changes (rounding of cells, their separation from glass) and the formation of intranuclear inclusions.
Epidemiology of adenovirus infection
The source is patients and virus carriers. Children who show signs of adenoviral infection are most at risk during the first 2 weeks. In some cases, adenoviruses are isolated from the respiratory tract up to the 25th day, and from feces up to 2 months. Virus carriage can be long-term (3-9 months).
Transmission mechanisms: droplet (main), possibly fecal-oral. Routes of transmission: airborne droplets, rarely food, water, household contact.
Susceptibility is highest in children aged 6 months and older. up to 3 years.
Seasonality and periodicity - recorded everywhere and year-round with an increase in the cold season. Periodicity is typical at intervals of 5 years.
Currently, the most common pathogens are serotypes 3 and 7. Adenovirus infection in children is observed in the form of sporadic cases and epidemic outbreaks, which are characterized by slow development and long duration.
After treatment is completed, immunity after an illness is type-specific and long-lasting.
The entrance gates are the mucous membranes of the upper respiratory tract, conjunctiva, and sometimes the intestinal epithelium. The introduction of adenoviruses into epithelial cells occurs by pinocytosis. Replication of viral DNA in the nucleus reaches its maximum level one day after infection. The affected cell is destroyed, viral agents spread to neighboring cells and to regional lymph nodes, where they continue to multiply. Viruses enter the blood directly from the lesion or through the lymphogenous route. Viremia usually lasts more than 10 days. It affects the vascular endothelium, which causes an exudative type of inflammation of the mucous membranes and a tendency to fibrin loss. Thrombokinase, formed during necrosis of the epithelium, coagulates the fibrinogen of the exudate into fibrin, and filmy deposits appear on the mucous membrane.
Pathogenesis
The pathogen enters the gastrointestinal tract through ingested mucus or hematogenously. In the small intestine, adenoviruses multiply for a longer period than in the epithelium of the respiratory tract. Replication of adenoviruses in the intestines is observed not only in patients with diarrhea, but also in children with other manifestations. The most pronounced inflammatory changes are localized at the entrance gate - the nasopharynx, tonsils, conjunctivae. Adenoviruses can enter the lungs through bronchogenic or hematogenous routes and cause the development of pneumonia.
The first symptoms of adenovirus infection: a tendency to lymphadenopathy, enlarged tonsils and adenoids. Mesadenitis occurs during the period of maximum proliferation of viruses in the intestinal mucosa. The liver and spleen are involved in the pathological process.
The destruction of epithelial cells and decreased activity of cellular and humoral immunity contribute to the accumulation of secondary bacterial flora. At the same time, with the normal functioning of the immune system, effective interaction between interferon and other lymphokines, macrophages, lymphocytes, and specific antibodies occurs, leading to the elimination of the pathogen from the macroorganism and clinical recovery. Infections of latent serotypes (1, 2, 5, 6) tend to persist for a long time in the lymphoid tissue of the tonsils, adenoids, and lymph nodes due to the integration of the viral genome with the genome of human lymphoid cells.
Pathomorphology
Morphological changes are characterized by the development of necrotic changes, mainly in the bronchi and lung tissue. Epithelial cells lose contact with each other and are rejected in entire layers. Serous fluid is found under the epithelium, and serous exudate, giant and mononuclear cells are found in the bronchial lumen. In the nuclei of cells, basophilic inclusions and accumulations of adenoviral antigens are found, and in the later stages, proliferation of the epithelium is noted. Giant cell degeneration of the epithelium in limited areas is detected in other organs (intestines, kidneys). Dystrophic changes are determined in the liver, myocardium, and kidneys.
Possible complications
The most common complications include:
- viral encephalitis;
- pneumonia, bronchitis;
- functional bowel disorders;
- sinusitis;
- otitis;
- false croup;
- damage to the urinary system (impaired kidney function);
- in rare cases - bradycardia (slowing the frequency of contractions of the heart muscle).
In young children, high body temperature may cause seizures.
Symptoms and diagnosis of the disease
Symptoms for adenoviral infection are as follows:
- Signs of body intoxication. In the first days of the disease, an increase in temperature to 39°C is observed. Fever is accompanied by general weakness, increased fatigue, headaches, daytime sleepiness, and enlarged cervical lymph nodes.
- Signs of catarrhal inflammation of the upper respiratory tract. The patient complains of a sore throat that gets worse when swallowing. In the first days of the disease, problems with nasal breathing and profuse nasal discharge are observed. Upon examination, swelling of the tonsils and the presence of a yellowish coating on the mucous membranes are revealed.
- Signs of damage to the lower respiratory tract. In the early stages of the disease, a dry cough appears, which over time begins to be accompanied by sputum discharge.
- Symptoms of viral conjunctivitis. The patient's eyelids swell, a burning sensation appears in the eyes, and when light enters the eyes, lacrimation begins. Purulent discharge from the conjunctiva is rarely observed. The infection can involve one or both eyes.
- Signs of intestinal damage. The patient complains of lack of appetite, pain in the mid-abdomen, bouts of vomiting and loose stools.
To identify the disease use:
- Examination and interview of the patient. The disease does not have typical symptoms, so it is quite difficult to make a diagnosis during the initial examination. Questioning the patient helps to find out the route of infection and assess the general condition of the body.
- Clinical blood test. Changes in the composition of the blood indicate the course of the inflammatory process. An increase in the number of leukocytes indicates damage to the respiratory system.
- Biochemical blood test. In cases of uncomplicated infection, no deviations in the analysis results are observed. With pneumonia, the concentration of sialic acid, C-reactive protein and fibrinogen increases.
- Immunoenzyme reaction. The material for research is epithelial cells. Antigens to adenovirus are detected in the sample.
- Immunofluorescence reaction. The diagnostic procedure allows you to detect antibodies to the infectious agent in the blood.
- PCR study. The method is aimed at detecting viral DNA in blood or other body fluids.
- Virological examination of sputum. Using this procedure, not only adenoviruses are detected, but also their sensitivity to antiviral agents is determined.