Primary appointment/consultation with a gynecologist—RUB 1,700. Repeated appointment/consultation with a gynecologist—RUB 1,200. See all prices
+7 (499) 400-47-33
Cyst is a common disease. This is a large neoplasm inside or near the ovary, looking like a dense capsule with a cavity filled with fluid (watery, dense or viscous). Cysts:
- They can be single or multiple (polycystic);
- Can develop in one ovary or both;
- Since the process is hormonally determined, they develop mainly during reproductive age.
There are:
- Cystomas, which are classified as true tumors;
- Cysts, which are tumor-like formations.
The most common are cystic processes. If the formation persists for two menstrual cycles, the issue of immediate surgical removal is decided.
Reasons for the development of neoplasms
There are several reasons for the development of this process. Knowing them, you can minimize the risk of developing a problem.
- Hormonal imbalance
– an increased risk factor. Regardless of the cause of hormonal imbalance, it is important to restore hormone levels. This circumstance alone contributes to the resorption of cysts. The problem is caused by:- Overeating and dieting;
- Excess or too little weight;
- Changing of the climate;
- Bad habits;
- Stress.
- Gynecological manipulations:
- Abortion;
- Childbirth, caesarean section, normal;
- Unqualified inspections;
- Installation of an intrauterine device.
- Gynecological diseases are in an advanced stage
, as there is an increased risk of complications. - Thyroid gland dysfunction.
- Wrong lifestyle:
- High physical activity.
- Frequent change of sexual partners;
- Early onset of sexual activity;
- Sex during menstruation;
- Sexual abstinence for a long time;
- Overwork and hypothermia.
For the formation of a cyst, there is not necessarily a reason - there may not be one, so you should not only undergo an annual preventive examination with a gynecologist, but also be attentive to your body.
The following symptoms of a cyst can be distinguished.
- Asymmetrical enlargement of the abdomen
due to growth of the formation or an increase in the volume of fluid filling the capsule. - Symptoms of compression of blood vessels and organs.
An enlarging cyst can put pressure on the intestines (lower sections) and bladder. Manifestations of pathology are expressed as constipation or stool disorder. If the vessels are compressed, varicose veins in the legs may develop. - Fever.
The neoplasm itself does not affect temperature changes. An increase in temperature can only occur if there are complications. This is a sign of cyst pathology and a reason to immediately see a doctor. Delaying a visit can result in infectious peritonitis. - Pain in the lower abdomen.
The source of their occurrence may be rupture of the capsule shell, suppuration, bleeding, or pressure of a growing cyst on nearby organs. - Disruptions in the menstrual cycle
caused by hormonally active cysts. Menstruation may be heavy or prolonged, and uterine bleeding may occur.
Exceeding the norm of male sex hormones provokes the following changes:
- Hirsutism - male pattern hair growth;
- Increasing the size of the clitoris;
- Rough voice;
- Feeling tired, overworked;
- Lack of orgasm, reluctance to have sex;
- Colored discharge, uterine bleeding;
- Nausea;
- Insomnia.
Ovarian cystoma - symptoms and treatment for women
Women who know about ovarian cysts do not always clearly understand the signs of pathology. A small cyst does not reveal itself for a long period of time. Often, the disorder is detected during a routine examination of the pelvic organs. When the formation increases in volume to 3 cm or more, the first symptoms appear. They begin with aching, pulling pain in the lower abdomen. Often the pain radiates to the groin and lumbar region. Large ovarian cystoma is accompanied by:
- feeling of heaviness, fullness in the stomach;
- increase in abdominal volume;
- menstrual irregularities;
- increased frequency of urination due to compression of the bladder tumor;
- intestinal dysfunction - diarrhea, constipation;
- swelling in the legs.
During exacerbations associated with violation of the integrity of the cystoma, the following may be observed:
- increased body temperature;
- stabbing pain in the abdomen;
- tachycardia;
- tension in the anterior abdominal wall.
For a disease such as cystoma, treatment is only possible through surgery. At the initial stages, organ-preserving operations are performed. Doctors remove only the affected areas of ovarian tissue. At the same time, the gland itself remains functional. Extensive lesions require complete removal of the ovaries. Effective in the early stages:
- radiation therapy;
- chemotherapy.
What types of ovarian tumors are identified:
- Dermoid
- with epidermal cells in the dermis (teratoma); - Endometrioid cysts
formed as a result of endometriosis; - Cytadenomas
are benign formations in the form of a large cyst (mucinous, serous).
The following tumor-like formations are distinguished:
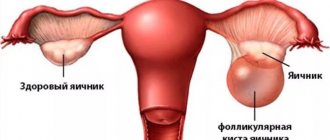
- Follicular cysts
- when the follicle continues to grow in the absence of ovulation. The most common are follicular single-chamber formations with thin walls. They are most often located on one side. The fluid accumulated inside the formation includes estrogens produced by the internal lining. The liquid has a yellowish tint and is transparent. The process of formation of this type of cyst starts if an egg does not come out of the dominant follicle. The formation grows due to the transudation of fluids from adjacent lymphatic vessels. In some cases, small cysts (no more than 4 cm) resolve on their own during menstruation. Then no treatment is required. A cyst that continues to grow and exceeds 5 cm requires attention. Drug therapy does not produce positive results. Requires surgery. - Corpus luteum cysts
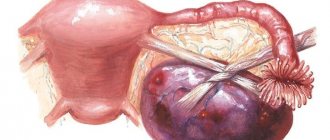
- are formed as a result of circulatory disorders after ovulation as a result of the action of the pituitary hormone; Corpus luteum cysts are the next most common and have the following features: They are structured similarly to the structure of the corpus luteum; - Single-sided, thick-walled;
- Formed only during reproductive age;
- They have an increased risk of rupture and provoke hemorrhage.
- Usually the disease develops asymptomatically and is often discovered during an examination by a gynecologist;
- If there is an inflammatory process, pain is possible in the lower abdomen;
- The cyst is palpable on the side of the uterus, smooth and elastic;
- There are frequent cases of such a cyst occurring in pregnant women; after termination of pregnancy, the formation resolves on its own.
are single-chamber formations formed from appendages; A paraovarian cyst is formed from the epididymis. This is a round tumor-like cavity with a chamber containing liquid with a predominant protein component. It grows slowly, can reach 20 cm, does not resolve on its own, and does not turn into a malignant form. As they increase, the walls become transparent. It is not anatomically connected to the ovary, therefore it does not affect its functioning. It has a high risk of complications - suppuration, torsion of the leg, rupture. May cause problems with conception, as it may compress the fallopian tube. During pregnancy it is asymptomatic and detected at the first screening.
Classification and causes of appearance
A cyst of the left or right ovary is diagnosed in women of different ages and affects their reproductive function. Previously, the pathology was called cystoma and always involved bilateral removal of the ovaries. Now, surgical intervention for such a tumor, if done on time, allows the woman to become pregnant in the future - the ovarian tissue is preserved.
Varieties
Depending on the structure of the epithelial wall, cystadenoma has the following varieties.
- Serous. Smooth-walled is the most common form of cystoma. It mainly occurs in the form of a round, single-chamber capsule and affects only one ovary. A bilateral process like this should always raise suspicion for malignancy. The average size varies from 3 to 15 cm. A cyst with a diameter of less than 3 cm often does not cause severe symptoms. Sometimes neoplasms measuring about 30 cm are also found.
- Papillary. Characterized by the presence of parietal papillary growths. If there are several neoplasms and they are concentrated into a cyst, it is quite difficult to diagnose such a pathology. The symptoms of this type of formation are similar to those of cancer, so the term “borderline ovarian cystadenoma” is often used. Treatment may be supplemented with chemotherapy or repeated surgery.
- Mucinous. A benign neoplasm that includes several chambers filled with a gel-like liquid - mucin. The epithelial lining of this cyst resembles the epithelium of the cervical canal, which is why it is filled with similar mucus. The cystic formation can reach impressive sizes - up to 50 cm. It is most often found in women after menopause.
The ICD-10 code for cystadenoma is N83. Pathology refers to non-inflammatory formations of the appendages. In the case of cancer growth, the code changes to D25.
Nature of education
At the moment, it has not been possible to establish specific causes for the development of cystadenoma. Most experts are inclined to believe that the neoplasm occurs due to serious hormonal disorders or complications after inflammation of the appendages. However, there are a number of probable factors that provoke the development of the disease. These include:
- early menarche (first menstruation);
- ovarian dysfunction;
- suffered stress;
- excessive physical and emotional stress;
- prolonged absence of sexual activity;
- sexually transmitted and infectious diseases;
- ectopic pregnancy;
- abuse of hormonal contraceptives;
- abortions, surgical interventions on the appendages.
The most common theory of the origin of cystadenoma is the following. Functional formations on the ovaries, which include follicular and corpus luteum cysts, periodically appear and resolve, which is due to a special cell layer in their wall. This process is allowed even in healthy women. Over time, the number of cells responsible for cyst regression decreases, along with the ability of such formations to resolve on their own. As a result, cystadenomas are formed. Depending on the accompanying processes, they can have a serous, mucinous or papillary structure.
Cyst. Lead tactics
The cyst is observed for 2 months. If positive dynamics are not recorded, the issue of surgery is decided. Such formations do not disappear on their own, there are no medications for treatment, and traditional methods will not help.
If the formation is small, you can simply observe it, but over time the cyst must still be removed.
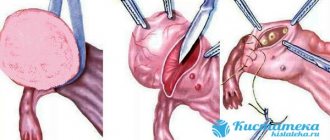
If a cyst is detected, a cystectomy is performed - the formation is removed along with the capsule to prevent recurrence. Modern capabilities (laparoscopy) make it possible to do this without damaging healthy ovarian tissue. The paraovarian cyst is removed with minimal intervention. In case of complications, surgery is also indicated.
Indications for surgery
- In the presence of a formation (cyst, tumor), which within three months of existence has not disappeared on its own or while taking anti-inflammatory or hormonal therapy.
- Cysts or tumors formed during menopause;
- The occurrence of complications: hemorrhage into the cyst, torsion of its legs, rupture, suppuration;
- High probability of developing a malignant process.
For the above indications, surgical intervention is necessary. However, the extent of the operation is individual for each patient. In women of fertile age, in the absence of a malignant process, cystectomy is performed - enucleation, while the ovarian tissue remains intact (not affected by the process). In women over 50 years of age or in cases where the ovarian tissue is affected, an ovariocystectomy is performed - removal of the formation along with the membranes. In the event that the fallopian tubes are involved in the process, a cystadnexectomy is recommended, in which case the cyst together with the appendages must be removed.
In severe cases of the disease and a widespread process, in the presence of large cysts in the ovary, healthy tissue may be absent, so in such cases it should be completely removed. But removal of one ovary cannot lead to significant hormonal disturbances in women of fertile age. In the future, such patients do not experience menstrual irregularities, and the ability to give birth to a healthy child is preserved.
To preserve the functions of the ovary, reducing tissue burns is of great importance. Therefore, to excise the cyst, the use of electrosurgery during the operation is minimal. In addition, in order to reduce the risk of adhesions, new generation anti-adhesion gels are widely used today. To prevent the contents of the cyst from spreading into the abdominal cavity during surgery, a special plastic container is used, into which the cyst is placed during removal from the peritoneal cavity.
Cystoma
Cystoma is an enlarging tumor, often having a multi-chamber cavity. Growth occurs both due to the accumulation of fluid inside the cavity and as a result of the division of cells that make up the formation. This tumor is real. Can be benign, malignant or potentially malignant.
There are groups of patients whose risk of developing cysts is especially high:
- patients with chronic diseases of the genital area, as an addition to complex therapy, such women are recommended to use hormonal contraceptives;
- patients with hormonal disorders: lack of pregnancy (hormonal infertility), disrupted menstrual cycle;
- patients who have undergone ovarian surgery, incl. cystectomy;
- Bad heredity – endometriosis and ovarian tumors in the family;
- Patients with breast cancer;
- Women who have had a pathological pregnancy.
There are difficulties in finding screening - identifying certain signs in many patients. It is necessary to conduct an in-depth examination of women if there is a formation larger than 3 cm on the uterine appendages during a two-hand examination.
Types of ovarian cysts
Ovarian cysts and tumors are divided into three types:
- Benign formations and cysts
- Borderline ovarian formations
- Malignant formations (tumors) of the ovaries
Benign ovarian formations (cysts) are more common in young women and may be associated with a disease such as endometriosis (when cells of the endometrium, the inner layer of the uterine wall, grow outside this layer), and may also be a consequence of menstrual irregularities.
Borderline ovarian tumors are more common in women over 30 years of age. Under a microscope, cysts can be identified as malignant, but they have a clinical course that is more reminiscent of benign formations. Borderline tumors in rare cases cause the spread of metastases (dropouts), but often provoke relapses (when after a while the tumor returns to the ovary or appears elsewhere) - in these cases, repeated operations are necessary. Chemotherapy is not effective in this case.
Malignant ovarian tumors (ovarian cancer) most often occur in women after menopause. Unfortunately, 80% of patients consult a doctor only with the manifestation of symptoms - at the third or fourth stage of the disease. In these cases, the most radical operations are performed, aimed at removing all tumor nodes from the abdominal cavity, and chemotherapy is administered after the operation (in some cases before the operation). Despite the late stage at presentation, 30-40% of patients have a chance of complete recovery.
What studies are carried out for ovarian tumors
- Bimanual examination remains relevant even with the most modern equipment, as it allows one to obtain important information.
- Speculum examination provides access to the cervix for examination, allows you to take aspirate and examine the endometrium.
- Washing and puncture of the abdominal cavity for cytological examination.
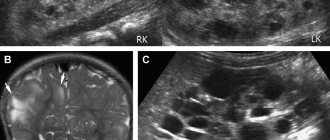
- Ultrasound using vaginal and abdominal sensors.
- Nuclear MRI and computed tomography allow for precise layer-by-layer studies to identify the presence of metastases in the lymph nodes.
- Ultrasound and mammography - examination of the mammary glands.
- Study of the condition of the endometrium.
- Examination of the intestine for the presence of a tumor (irrigoscopy, rectromanoscopy).
- Examination of the gastrointestinal tract, since the appearance of a metastatic tumor in the pancreas, intestines, and stomach is possible.
- Tumor markers. Increase in tumor marker CA-125 - more than 35 units. indicates an increased risk of developing an oncological process. But this statement is not always true, since there are cases where a significant excess of the tumor marker norm in endometrial ovarian cysts and endometriosis is not related to oncology.
- Carrying out laparoscopy
Ovarian cyst or cancer: how to distinguish
The greatest difficulty in diagnosis is the problem of distinguishing a cancerous ovarian cyst from a benign one. To accurately determine the etiology, doctors conduct a series of examinations and tests.
Attention! According to statistics, 75% of patients with ovarian cancer are admitted at an advanced stage, which indicates a latent form of oncology. When the formation develops into malignant, surgery is necessarily indicated.
In most cases, the cavity detected on ultrasound is benign, but if oncology is hidden inside, then it must be diagnosed immediately. Diagnostic methods to distinguish cancer from benign formations will be:
- Ultrasound performed 2 months after the initial examination, which revealed a cyst;
- laboratory tests: general and biochemical blood tests, where the results are presented by modified indicators;
- determination of CA-125 level - oncological detection of ovarian cancer;
- in the presence of bloody discharge, a histological examination is performed;
- MRI as indicated.
Lead tactics
- Surgery for a malignant ovarian tumor.
The uterus and cervix, appendages, as well as the greater omentum are removed. Removing the oil seal is important because... In some cases, it contains micrometastases. In addition, the omentum promotes the production and accumulation of ascityl fluid.
- Surgery for a benign tumor
Adnexectomy is performed - removal of appendages. Simultaneously with surgical treatment:
- the internal lining of the formation is examined in detail for malignant growths;
- Histological examination is performed.
A modern approach to diagnosing and treating cysts and other diseases of the female genital area is offered by gynecologists at the RAS clinic in Moscow. Here you can undergo a preventive examination by a gynecologist and have a pelvic ultrasound performed. You can make an appointment for a consultation on the website or by calling the numbers provided.
Stages of ovarian cancer
| Stage 1 | Stage 2 | Stage 3 | Stage 4 |
Stage Ia
Stage Ib
Stage Ic
| Stage IIa
Stage IIb
Stage IIc
| Stage IIIa
Stage IIIb
Stage IIIc
| Tumor with distant metastases (lungs, liver and other distant organs) |
DETAILS: Treatment of ovarian cancer: surgical and drug treatment of ovarian cancer
Treatment
Regardless of the size and clinical picture of the ovarian cyst, its surgical removal is indicated. The need to remove an ovarian cyst is dictated by the possibility of its malignancy, excessive growth, and disruption of the pelvic organs. During the operation, the cystoma is removed and its nature is clarified. The extent of surgical intervention for ovarian cystoma is determined by the type, size of the tumor, the woman’s age, and pregnancy planning. Surgeries for ovarian cystomas are performed through laparoscopy or laparotomy.
To determine the extent of the operation, urgent intraoperative histological examination of tumor tissue is indicated. In the postmenopausal period, the optimal treatment option for ovarian cystoma is removal of the uterus by panhysterectomy.
If the pedicle is torsed or the capsule of an ovarian cystoma is ruptured, the intervention is emergency.