Pavel Anisimov
Health depends much more on our habits and nutrition than on the art of medicine
calendar_today
February 1, 2017
visibility
Adrenal tumors in most cases are benign neoplasms, which are a proliferation of the cellular structures of these organs. They differ from each other in their method of occurrence, structure and many other factors. The latter determine the nature of the symptoms of tumors in the adrenal glands in women.
The adrenal glands have a rather complex structure, consisting of outer, cortical, inner and medulla layers, and are part of the body's endocrine system. The synthesis of hormones that provoke the occurrence of neoplasms occurs in the cortex of the organs. However, it has not yet been established exactly why such tumors appear.
Diagnosis of pathology involves the release of the main hormone that provoked the appearance of the disease in question. In cases of adrenal tumors, surgeons are usually involved in treatment, although in some cases (discussed below) doctors limit themselves to corrective hormone therapy.
Adrenal tumors
https://youtu.be/tTwti-vn6qk
There are benign and malignant adrenal tumors. Neoplasms, differing in structure and characteristic symptomatic signs, are located in the form of foci in the adrenal tissue, which consists of the medulla and cortical layers.
Statistics show that patients more often suffer from a benign tumor; a malignant tumor of the adrenal gland is rare. An endocrinologist can determine the nature of the disease based on symptoms and examination results.
Surgery
A tumor of the adrenal glands (symptoms in women can appear already at an advanced stage) in most cases is treated radically, that is, with the help of surgery. The absolute indication for surgery is the detection of a large malignant or hormonally active tumor.
Today, the intervention can be abdominal, that is, it is done through standard incisions with a scalpel in the anterior abdominal wall. But laparoscopy is considered simpler and safer. The essence of the method is to remove the tumor by inserting a laparoscope into minimal incisions on the anterior abdominal wall.
This reduces blood loss, shortens the recovery period and reduces the likelihood of tissue damage that occurs during abdominal surgery. Both types of intervention are performed under general anesthesia. After this, the patient is under observation for at least 10 days.
After removal, a course of chemotherapy and hormonal drugs are prescribed. Often only the tumor and part of the organ that was affected is removed, but in some cases radical resection is required to remove the entire adrenal gland. If the neoplasm is malignant, nearby lymph nodes are additionally removed.
Classification of tumors
https://youtu.be/O1OfS3x8NHU
There is a multi-level typology of adrenal tumors:
- Localization area:
- cortical;
- cerebral.
- Character of the tumor:
- benign;
- malignant;
- neuroendocrine.
- Development stage:
- first;
- second;
- third;
- fourth.
- Hormonal activity of formation:
- active;
- inactive.
- Pathological physiology:
- androsteromes;
- corticoestroma;
- corticosteromas;
- aldosteromas;
- corticoandrosteromes;
- pheochromocytomas.
Tumors
Endocrine glands have an outer cortex and a medulla.
The organ synthesizes steroid substances:
- glucocorticoids;
- mineralocorticoids;
- estrogens;
- progesterone;
- androgens.
Benign organ tumors practically do not cause symptoms and are discovered by chance during a comprehensive examination of the body. But adrenal tumors can also be malignant. Primary ones develop from organic tissue, secondary ones appear during metastasis.
Localization
Tumors of epithelial (aldosteroma, androsteroma, adenoma, corticoestroma, carcinoma) or connective (fibroma, myeloma, angioma, adrenal lipoma) tissue of the adrenal cortex are uncommon. Neoplasms that affect the medulla are:
- ganglioneuromas;
- pheochromocytomas.
Ganglioneuroma is a focal proliferation of nerve cells - ganglia. The tumor, which is small in size, is most often located inside the left adrenal gland.
The disease is more often diagnosed in young women. This is due to emotional and physical stress in the body. Pheochromocytoma affects neuroendocrine cells in the inner layer of the adrenal glands. This type of tumor may be accompanied by disturbances in the functioning of the nervous system and changes in skin color.
General symptoms
General symptoms common to most types of adrenal glands are divided into:
- Primary.
They appear as:
- disturbances in nerve conduction in body tissues;
- increased blood pressure, development of persistent hypertension;
- nervous overexcitation;
- panic caused by fear of death;
- pain in the chest and abdominal cavity, of a pressing nature;
- frequent urination.
- Secondary.
Secondary signs are characterized by the appearance of the following pathologies:
- renal dysfunction;
- diabetes;
- sexual dysfunction.
https://youtu.be/UNgeHUKj5YM
Character
https://youtu.be/fgR_GNtgVrc
Benign tumors are characterized by the absence of symptomatic signs, slow cell division and small size (up to 5 cm in diameter). It is possible to detect the formation only with ultrasound examination.
Malignant tumors are characterized by obvious signs of pathology in the form of intoxication, rapid division of pathological cells and large sizes (diameter - from 5 to 15 cm). Formations of this type differ in the nature of their occurrence:
- primary – the neoplasm initially arises in the tissues of the adrenal glands;
- secondary - damage as a result of the spread of metastases from a tumor of another organ.
Neuroendocrine tumors, which form in the medulla of the endocrine system organ, are malignant in nature and are characterized by slow tumor growth.
Classification
Diagnosis of the disease determines treatment. In order to facilitate the treatment of the disease in question, several classifications have been adopted in medical practice.
Adrenal tumors are usually divided depending on their location. It is formed from two parts of the organ:
- Adrenal cortex. From it arise tumors such as androsteroma, aldosteroma, corticoestromy, corticosteroma, mixed.
- Adrenal medulla. These include ganglioneuromas and pheochromocytomas.
The main difference between benign and malignant tumors is that cancer cells divide more actively and, accordingly, attack new tissues faster. The former, in turn, in most cases develop slowly. Moreover, benign tumors in the adrenal glands rarely show symptoms. Therefore, the diagnosis of such diseases is usually carried out as a preventive measure.
Even less commonly, people develop formations from neuroendocrine cells. They develop very slowly. However, at their core they are a type of malignant oncology.
In addition, the type of tumor in question is divided into:
- Hormonal. They include such formations as:
- pheochromocytes;
- corticosteromas;
- corticoestroma;
- androsteromes;
- aldosteromes
- Non-hormonal. Characterized by a lack of hormonal activity. Benign formations occur in the form of myomas, fibroids and lipomas; malignant - pyrogenic cancer, teratoma and melanoma.
The classification of pathology is carried out depending on the tissues in which the tumors appeared:
- In epithelial (adenoma, cortiestroma and others).
- In the connective tissue (fibroma, lipoma, etc.).
- In brain tissue (ganglioma, pheochromocytoma, neuroblastoma);
- Combined, which simultaneously affected the tissues of the cortical and medulla layers (incidentaloma).
Another classification of the problem is determined depending on the pathology that it provokes:
- Imbalance in water-salt and sodium metabolism.
- Metabolic disorder.
- The emergence of secondary male sexual characteristics in women, manifested in the form of active growth of body hair, deepening of the voice and change in gait.
- A similar process occurs in men, manifesting itself in the form of increasing breast size, a decrease in the number of body hairs and a higher voice.
- Combination of male sexual characteristics and metabolic disorders in women.
These consequences are caused only by hormonally active tumors, which will be discussed below.
Stage of development
Adrenal tumors differ according to the stages of development of pathology:
- The first stage is characterized by the presence of a tumor with a diameter of less than 5 cm, the absence of enlarged lymph nodes and the spread of metastases.
- The second is a neoplasm with a diameter of more than 50 mm, not accompanied by enlarged lymph nodes.
- The third is a tumor with a diameter of less than or more than 50 mm, accompanied by the spread of metastases.
- The last stage is a neoplasm, the localization of which has already spread to the lymph nodes and other organs, and may have a different diameter.
Traditional medicine recipes
Some alternative medicine recipes help alleviate the patient's condition. They cannot be used as the only method of therapy, and before starting the course, consultation with a doctor is required.
An infusion of mulberry fruits is considered a good remedy for eliminating the symptoms of intoxication. It must be prepared from 100 g of fruit and 1 liter of boiling water, leave for at least 30 minutes. After this, divide the resulting composition into 4 parts and consume throughout the day. Repeat the procedure daily for 2 weeks.
An infusion of medicinal lungwort can be obtained from 1 teaspoon of dry raw materials and 300 ml of boiling water. After 20 min. After infusion, the product is ready for use. You need to take 300 ml per day, the course duration is 10 days.
A decoction of geranium leaves is a powerful remedy for the treatment of adrenal glands. For 400 ml of water you will need several small crushed leaves, which should be boiled for 3 minutes. After this, filter the product and take 50 ml 3 times a day for 10 days.
Blackcurrant leaves are also used to obtain a healing decoction. For 2 liters of water you will need 10 g of fresh leaves, which must be boiled for 30 minutes. Filter the finished product and consume 100 ml 2 times a day. The duration of the course is from 10 to 14 days.
Hormonal activity
https://youtu.be/WyPBJzWPwl0
Two types of tumors can form in the adrenal glands: those that produce hormones and those that do not. The latter are often benign and are accompanied by high blood pressure, metabolic disorders in the body, and diseases of the endocrine system. Incidentalomas vary depending on the place of formation:
- cortical layer - adenoma, carcinoma, nodular hyperplasia;
- medulla - pheochromocytoma, ganglioneuroblastoma;
- mesenchymal tissue - lipoma, fibroma, angioma, wen.
There is a classification of hormonally active adrenal tumors depending on the substance secreted:
- aldosteromas;
- corticosteromas;
- androsteromes;
- corticoestroma;
- pheochromocytomas.
Aldosteroma is a hormonally active tumor of the adrenal gland that affects the outer layer of adrenal tissue. Occurs in 1/7 of patients (mostly females) with a disease of the endocrine system.
It is often benign in nature. Aldosteroma can be single or multiple, most often characterized by unilateral localization, that is, it affects only one lobar part, but it can also be bilateral.
Corticosteroma is a common type of adrenal tumor that forms in the outer layer of the endocrine system organ. According to the nature of the flow they are divided into:
- benign – glucosteroma;
- malignant – corticoblastoma, adenocarcinoma.
With corticosteroma, Itsenko-Cushing syndrome develops due to excessive release of cortisol. This pathology affects metabolism and the functioning of the endocrine system.
Androsteroma occurs in the female population as a result of the production of an active hormonal substance, androgen, in the reticular zone of the outer layer of the adrenal gland. Malignant androsteroma is called carcinoma.
The neoplasm can reach a diameter of 15 to 20 cm and weigh 1 kg, and is accompanied by the spread of metastases to the lungs, liver and lymph nodes of the abdominal cavity. Timely detection is observed in a small number of cancer patients.
Corticoestroma is a rare type of neoplasm, most often malignant in nature, with the rapid spread of cancer cells. The tumor often occurs in the middle-aged male population (up to 35 years) in the reticular and fascicular zone of the cortex.
Pheochromocytoma is a neoplasm, which in most cases is benign, originates inside the adrenal medulla.
Tumors of this type among the adult population are more often diagnosed in women, and in children - in boys. Active production of the hormonal substance catecholamine, associated with hereditary predisposition or genetic pathologies, is detected in adults from 30 to 50 years old.
Hormonally active tumors
Adrenal tumors (symptoms in women may only appear in advanced stages) can be hormonally active. Normally, the paired organ in a stressful situation stimulates increased work of the cardiovascular, digestive and excretory systems. At the same time, sweat production increases, blood vessels dilate, and heart rate increases.
With a sharp rise in stress hormones in a person’s blood, the formation of a hormonally active tumor is suspected, which, even at rest, increases their number to critical levels.
These types of neoplasms are considered dangerous because they often provoke complications in organs and systems, and in most cases they are malignant. These include aldosteromas, corticosteromas, androsteromas and other types of tumors.
Pathological physiology
Hormonally active neoplasms cause various disturbances in the functioning of the body. The results of an excess of the substance in aldosterome are:
- violation of water-salt balance;
- increased sodium levels in the blood;
- low urine density;
- increased blood pressure;
- frequent headaches;
- thinning of vascular tissues;
- muscle weakness;
- infrequent stool, constipation.
Corticosteroids contribute to metabolic disorders, which leads to obesity, early maturation in adolescents, or decreased sexual activity in adults.
Excess of androgens (male hormones), which is more common in women aged 20 to 40 years, leads to the appearance of male-pattern body hair, the formation of bald spots and bald spots on the head, changes in the timbre of the voice, and an irregular menstrual cycle.
Corticoestroma - leads to an increase in the volume of the mammary glands, the absence or reduction of hair on the body, and an increase in the timbre of the voice in men.
The mixed type - corticoandrosteromas - is associated with metabolic disorders and an increase in the production of male hormones in the female body.
A benign neoplasm in the form of pheochromocytoma, spreading inside the medulla, affects metabolism and the functioning of the cardiovascular system.
The structure of the adrenal glands and the production of hormones
The human adrenal glands are a paired organ that is located directly above the kidneys. They belong to the endocrine system. The adrenal glands consist of only 2 layers of tissue - the cortex and the medulla. The first is yellow, the second is red-brown.
In the cortical layer, 3 zones can be distinguished: glomerular, fascicular and reticular. The first produces 3 hormones responsible for regulating sodium levels in the blood and water-salt metabolism. The second produces cortisol and cortisone. These hormones are responsible for the immune system and metabolism in the body.
The zona reticularis is necessary for the production of androgenic hormones. They are responsible for the appearance of secondary sexual characteristics in humans.
The medulla is not divided into several zones. It produces adrenaline and norepinephrine. These hormones are responsible for regulating the functioning of all systems in the human body. They have the most pronounced effect on the nervous, cardiovascular and digestive systems.
Causes
Endocrinologists today cannot identify the exact cause of the formation of a benign or malignant tumor in the adrenal gland. But there are factors that contribute to the development of neoplasms:
- Genetic predisposition.
- Violation of the rules of a healthy lifestyle:
- drinking alcohol, smoking;
- unhealthy diet: inclusion in the diet of fatty, smoked, spicy foods, fast food, sweet carbonated drinks.
- Ecology, negative impact of environmental factors.
- Chronic diseases of the endocrine system, pathologies of the thyroid and pancreas.
- Mechanical damage to the adrenal glands, which are the result of accidental injuries, bruises.
- Stress, excessive emotionality.
- High blood pressure.
A tumor on the adrenal gland can appear as a result of cancer of another vital organ, accompanied by metastases - the spread of cancer cells.
Prognosis and complications
If left untreated, the tumor can provoke the spread of metastases to neighboring organs. In addition, its size may increase so much that surgery will be impossible. A common complication will be heart failure, uncontrolled arterial hypertension, and obesity.
In addition, complications may develop in any internal organ, since increased levels of adrenal hormones lead to changes in all processes. Diabetes mellitus is a common complication that worsens the course of the disease. However, surgery to diagnose pathology is performed quite rarely. The most dangerous consequence is death.
For patients who have benign and hormonally inactive tumors, the prognosis is favorable. In most cases, conservative treatment is effective or is not required at all. Then the doctor simply regularly examines the patient and monitors the tumor.
With hormonally active and malignant tumors, the prognosis in most cases is unfavorable. Only 2% of patients survive after surgery. Most often, death occurs some time after surgery due to various complications.
Adrenal tumor is a dangerous and common disease. Symptoms in women appear at different stages depending on the type of pathology, and treatment should be timely and comprehensive to avoid complications.
Article design: Vladimir the Great
https://youtu.be/11Ay4uH2kgo
Symptoms of pathology
Benign neoplasms do not have obvious signs of pathology. Symptoms of a tumor in the adrenal gland depend on the hormone produced in the inner or outer layer.
| Types of tumor | Symptoms |
| Aldosteroma |
|
| Corticoesteroma |
|
| Corticosteroma |
|
| Androsteroma |
|
| Pheochromocytoma |
|
There are general symptoms of adrenal tumors that are characteristic of all types of tumors: weakness of muscle tissue, high blood pressure, stress instability, panic fears, compressive pain in the sternum and heart area, frequent urination.
The manifestation of tumors may be accompanied by impaired renal function and sexual function. The appearance of neoplasms in children is characterized by early puberty.
For neoplasms in the adrenal glands in women, a manifestation of masculinization is typical, for men - feminization syndrome. Crises develop in the presence of a benign or malignant tumor of the adrenal cortex and medulla.
Symptoms of benign and malignant adrenal tumors in women
Benign neoplasms rarely provoke severe symptoms and are therefore diagnosed at a late stage using ultrasound. But malignant tumors of the paired organ can lead to various disorders. Symptoms depend on the type of pathology.
There are manifestations that are present in any type of education:
- Changes in blood pressure in one direction or another.
- Impaired fat metabolism and fat deposition in places atypical for a woman.
- Deterioration of wound healing on the skin.
- Heart disorders, manifested in the form of arrhythmia and tachycardia, deterioration of myocardial function.
- Menstrual irregularities.
- Infertility.
- Change in libido.
- Increased muscle mass characteristic of men.
- Changing the timbre of your voice.
- Deterioration of the skin condition, dryness.
- Hair loss and appearance on the face, which is not typical for women. In this case, baldness occurs according to the male pattern.
- Increased risk of fractures due to brittle bones.
- Muscle weakness and decreased performance.
Some patients experience frequent urination, as well as pain in the kidney area associated with their increased work.
Diagnosis of adrenal tumors
To determine the location, nature and size of the tumor, adrenal tumors are diagnosed. There are several diagnostic measures to give a complete picture of the disease.
- Laboratory diagnostics:
- general blood and urine tests;
- coagulogram;
- Hormone level tests to determine the active substance.
- Blood pressure measurement.
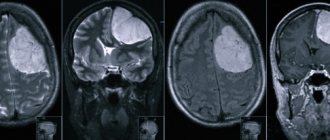
- Magnetic resonance and computed tomography, ultrasound, radiography to identify large or small formations and the possible spread of cancer cells - metastases.
- Phlebography to determine the concentration of hormones is carried out only for neoplasms of the cortex; it is prohibited in the presence of a tumor of the adrenal medulla.
Diagnostics allows you to detect signs of other diseases, as well as determine the characteristic features of the tumor and organize competent treatment.
Diagnostics
An adrenal tumor (symptoms in women differ depending on the stage of development of the disease) can be diagnosed using instrumental and laboratory examination methods.
Laboratory methods
Among laboratory diagnostic methods, the most informative and easy to carry out are distinguished, allowing you to immediately obtain results.
| Method | Description |
| General and biochemical blood test | A standard diagnostic method that allows you to determine general disorders and disorders of the kidneys, heart, and blood vessels. Blood is taken from a vein and sent to a laboratory where the study is carried out. |
| Blood test to determine levels of adrenaline and norepinephrine | Allows you to exclude or confirm the presence of a pheochromocytoma tumor, which affects the level of these hormones. |
| Diagnostics of 24-hour urine to determine free cortisol and aldosterone | Another standard method for suspected adrenal tumors helps clarify the diagnosis and identify the extent of damage to the organ. |
| Phlebography or examination of blood from the adrenal veins | Blood from the adrenal veins may contain specific components that are not yet detected in the systemic circulation. |
| Test with Captopril | Before taking blood from a vein, the patient takes a single dose of Captopril or its analogue, after which biological material is collected and tested for hormone levels. |
After receiving the results of laboratory diagnostics, the specialist prescribes additional instrumental examination.
Instrumental methods
Instrumental methods include ultrasound and MRI. The first method helps to identify a tumor whose size exceeds 0.5 cm. The specialist determines its location, shape and notes the possibility of injury to neighboring tissues.
MRI is considered a more modern and informative method, since it helps to obtain a layer-by-layer image of a tumor, even if its size does not reach 0.5 cm. In this case, the doctor sees all the details, shape and location, as well as violations of other organs. Usually, an ultrasound is performed first, followed by magnetic resonance imaging, which clarifies the diagnosis.
Treatment
https://youtu.be/bAZlR-sjZ8M
To treat tumors in the adrenal glands, chemotherapy and surgery are used. The prescription of therapy depends on the results of the examination and determination of the type of tumor. The methods of their treatment are determined by an endocrinologist. The main indications for urgent surgery are:
- malignant nature of the tumor;
- the process of degeneration of benign cells into cancerous tumors;
- tumor size more than 3 cm in diameter;
- rapid growth of cancer cells;
- excessive release of hormones.
Removal of any adrenal tumor is performed in several ways:
- Open – removal of the tumor through an incision in the abdominal cavity.
- The laparoscopic method is a puncture with a diameter of no more than 1 cm in the anterior abdomen to insert a surgical instrument and remove a tumor in the adrenal glands.
With benign tumors in the adrenal glands, only the affected organ is removed. If a malignant tumor is present, the lymph nodes located near the affected adrenal gland are removed, through which cancer cells spread throughout the body.
Removing a tumor inside the medulla is a complex surgical operation that can lead to circulatory problems.
A hypodense adrenal mass should be treated only after the results of ultrasound and computed tomography.
Before performing surgery, the doctor selects anesthetic drugs in accordance with the patient’s condition and individual characteristics of the body. After removal of the tumors, a special course of hormone therapy is prescribed.
There are contraindications to the operation:
- serious diseases that can lead to complications during surgery;
- the presence of a malignant cyst;
- age restrictions.
Chemotherapy is prescribed if there is a malignant tumor inside the medulla (inner) layer of the adrenal gland. The procedure is carried out using toxic chemicals that are administered through a vein. Injections of toxins have the effect of reducing the size of the tumor and the number of advanced cancer cells.
Classification by physiological pathologies
Depending on the physiological disorders that develop as a result of the formation of an adrenal tumor, several types of pathology can be distinguished:
- Neoplasms that provoke a disorder of water-salt metabolism in the patient’s body are quite common and difficult to treat.
- Tumors that lead to metabolic disorders. At the same time, the symptoms differ in different patients depending on the individual characteristics of the body.
- Pathology of the adrenal glands, in which a masculinizing effect is noted, is considered a rare species.
- Neoplasms that provoke a feminizing effect, that is, increasing the amount of female sex hormones in the patient’s body. For women, this tumor is not as dangerous as for men.
- Tumors that lead to the appearance of symptoms from several internal organs and systems. Such formations are common, which complicates diagnosis.
Experts also identify other types of tumors, but these are the most common. In each case, the most pronounced symptoms help determine the type of disease.
Forecast
The outcome of the operation in patients depends on the type of tumor that needs to be eliminated. Timely removal of a benign tumor in most cases has a favorable prognosis. Elimination of androsteric formation can lead to developmental arrest in childhood.
After removal of a pheochromocytoma, problems with heart rate and blood pressure often persist, but they are treated with a course of therapy. Detection of a malignant tumor rarely means a positive prognosis for the disease.
https://youtu.be/y3ijMcz_3gU
Conservative treatment of neoplasms
Drug treatment is carried out only at the initial stage, when the tumor is benign and hormonally inactive. In this case, a complex of drugs is prescribed that can relieve symptoms and improve the patient’s condition.
It is worth noting that most of the medications are aimed at normalizing heart rate and blood pressure:
- Atenolol is a drug that reduces heart rate by reducing myocardial oxygen demand. This helps improve the patient's condition and prevent deterioration. The drug is prescribed in courses of 10-20 days with daily use of 1 tablet in the morning and evening.
- Nitroglycerin is a popular remedy that is used for hypertensive crisis and the appearance of symptoms of angina pectoris. The drug dilates blood vessels and reduces the load on the heart. It is necessary to use it in case of exacerbation of symptoms, shortness of breath and increased heart rate, 1 tablet, dissolving until dissolved. The product is not used for course use.
- Enalapril – an antihypertensive drug used for regular increases in blood pressure. Prescribed in courses of 2 weeks with daily use of 1-3 tablets, depending on blood pressure levels. Many patients take the medication on an ongoing basis.
Enalapril is a vasodilator medication that hypertensive patients take every day.
In some cases, treatment with a radioactive isotope is used, which destroys tumor cells and even metastases. After penetration into the systemic bloodstream, the medicine reaches the lesion and begins to act actively. The effectiveness of the product has been proven, but in advanced stages it does not bring results.
Prognosis and prevention
Prognosis after surgery depends on the type of tumor, its nature and the treatment measures taken. Benign tumors almost never recur, which is not the case with malignant tumors. The sooner the tumor is removed, the more favorable the prognostic data. However, some patients may experience complications and consequences. For example, if an androsterome was removed and the patient was a child, the child will most likely be stunted. After successful removal of pheochromocytoma, half of the patients develop cardiac disorders within a year.
Thirty percent of patients who have their aldosteroma removed experience moderate hypertension that requires lifelong medication. If the corticosteroma is removed, the patient recovers after about one and a half to two months. The symptoms that were present during cancer gradually go away - blood pressure, weight return to normal, sexual function is restored, etc. Metastatic tumors often give a poor prognosis, especially if the pathology cannot be treated with surgery. In this case, a person can live up to two years.
Preventive measures include maintaining a healthy lifestyle:
- giving up cigarettes and alcohol;
- proper nutrition;
- avoidance of provoking factors.
After treatment, prophylaxis is carried out to prevent relapse. The patient is registered and must be examined every six months (and more often at first). After removal of a malignant tumor, only after five years a person is considered completely cured. When the adrenal gland is removed, alcohol, sleeping pills, and strong physical and psycho-emotional stress are strictly contraindicated for the patient.
Therapeutic measures
Symptoms and treatment regarding the adrenal glands are closely related.
Modern medicine knows different practices:
- innovative and conservative,
- radical and gentle.
But medical solidarity lies in the fact that in any case it is necessary to normalize hormonal levels.
Treatment of an adrenal tumor begins after a thorough examination of the condition of the body and the development of the formation. Benign new adrenal tissue does not require treatment or any invasion. Finely focal neoplasms that do not produce hormones require only regular examination, repeated over a certain period of time. As a rule, such tumors have a favorable prognosis.
Modern medicine has several treatment methods, in some cases complex treatment is used. The most common method is surgical removal of the source of the disease.
A method of irradiation of adrenal cortex cancer is used to prevent cancer cells from entering the bone tissue. The method is ineffective without direct irradiation of the immediate tumor.
Drug treatment
The most common method of treatment and preventive measures is drug therapy. With the help of medications, the hormonal secretion of newly formed cells is regulated and their growth is inhibited. Drugs are prescribed in cases where it is impossible to operate on adrenal glands with metastases, as well as when the oncological tumor has been partially removed. Mitotan is recognized as the main drug , which can be combined with chemotherapy procedures. The medicine is capable of destroying cancer formations. Other drugs are also prescribed ( Hydrocortisone, Prednisolone, Dexamethasone ).
Medrol is considered effective , which is recommended in combination with other drugs in cases of insufficiency of the adrenal cortex. Another medicine called Polcortolone contains the hormone Glucocorticoid, necessary for the body, and Cortef.
Radioisotope therapy and drug treatment require regular monitoring of the blood condition regarding indications of the presence of hormones.
Common chemicals to help a patient in the late stages of tumor treatment:
- Cisplatin;
- Doxorubicin;
- Etoposide;
- streptozocin;
- Vincristine.
Chemical therapy gives a 35% chance of successfully completing treatment.
Surgery
Adrenal cancer is a serious medical finding; in such a situation, surgical intervention is required. The operation is carried out in a specialized medical center. The existing competence in this surgical field is important.
Surgical practice has been enriched by the method of laparoscopy , in which stage 1-3 adrenal cancer is removed through special punctures in the peritoneal cavity. An undesirable aspect of this type of treatment is the possibility of recurrence of the disease. Micro metastases can persist during surgical procedures and then grow throughout the body. In such circumstances, repeated surgery is required.
Aldosteroma, or Conn's syndrome
There are actually several diseases that cause an increase in the level of the hormone aldosterone in the blood. Depending on the reasons that caused its increase, hyperaldosteronism is divided into primary (independent of the renin-angiotensin system) and secondary (dependent on it).
Normally, aldosterone production is regulated by a system called the renin-angiotensin-aldosterone cascade. Under the influence of certain factors, a number of biochemical processes are triggered that stimulate the production of a special substance by the kidneys and other organs - renin, which promotes the formation of angiotensin, from which aldosterone is subsequently formed.
In primary hyperaldosteronism, an increase in aldosterone levels occurs regardless of the formation of renin and angiotensin - this is observed in local pathology of the adrenal glands and tumor neoplasms.
Secondary hyperaldosteronism is observed in cases of serious pathology of the heart, liver, kidneys, and also as a result of taking diuretic drugs.
In almost 2/3 of cases, primary aldosteronism occurs due to small size (no more than 4 cm) unilateral adenoma of the adrenal cortex. The malignant form of primary hyperaldosteronism is diagnosed only in 2% of cases and is a carcinoma. The remaining 30% of cases of primary hyperaldosteronism are associated with an increase in the number of glandular cells - hyperplasia - of the adrenal cortex. The reasons for the development of this condition are unknown, so hyperaldosteronism in this case is called idiopathic.
An increased level of aldosterone in the blood causes sodium retention in the body and increases the excretion of potassium in the urine. Excess sodium leads to fluid retention in the body, which leads to an increase in circulating blood volume, inhibits the synthesis of renin and angiotensin, and increases the susceptibility of the vascular wall to the effects of adverse factors that cause an increase in blood pressure. Potassium deficiency negatively affects the functioning of many organs and systems, in particular, it causes disturbances in the structure and function of the renal tubules, muscles, nervous system (both central and peripheral), increases neuromuscular excitability, and reduces glucose tolerance.
Clinical manifestations of aldosteroma
As a rule, people aged 30-50 years suffer from aldosteroma, and women are 3 times more likely than men.
Patients may complain of:
- severe constant headache;
- general weakness;
- muscle weakness, inability to perform physical activities that were easily performed previously;
- constant thirst;
- increased urination, especially at night;
- paresthesia (tingling, burning, tingling sensation) of the face, hands and feet;
- convulsions;
- increased blood pressure – both stable and with periodic hypertensive crises.
Diagnosis of aldosteroma
Computed tomography can detect adrenal tumors larger than 10 mm.
Patients with symptoms characteristic of aldosteronism are shown a number of diagnostic measures to establish an accurate diagnosis and carry out a differential diagnosis of primary and secondary hyperaldosteronism.
First of all, patients who complain of a persistent increase in blood pressure and other symptoms listed above are prescribed a general and biochemical blood test, a general urinalysis and an ECG.
In the general analysis, an increased ESR is determined, signs of anemia (low hemoglobin and red blood cells) and an increased level of leukocytes, in particular neutrophils, may be noted.
In a biochemical blood test, potassium and sodium levels are determined. The level of the first is sharply reduced, while the second, on the contrary, is increased.
A urine analysis reveals a reduced density, as well as an excess of potassium content.
The cardiogram reflects measurements characteristic of low potassium levels in the blood, namely:
- voltage reduction;
- inversion (the peak is not up, but down) of the T wave;
- decrease in the ST segment below the isoline;
- prolongation of the QT interval.
If hypokalemia and hypernatremia are detected in the blood, if these minerals are sufficiently supplied to the body with food, the level of hormones in the blood - aldosterone and renin - is determined. It is found that the aldosterone content is sharply increased - 3-4 times higher than normal values. The level of renin depends on what type of aldosteronism occurs in this case - primary or secondary. In primary aldosteronism, the concentration of renin in the blood plasma is reduced, and in the case of secondary aldosteronism, when an increase in aldosterone levels is associated with some serious underlying pathology, renin activity increases in parallel with an increase in aldosterone levels.
Urinary excretion of aldosterone will also be increased.
To differentiate between primary and secondary hyperaldosteronism, functional tests can also be performed, for example, with spironolactone or furosemide.
To confirm the diagnosis, topical diagnostic methods are used - computed tomography and magnetic resonance imaging. The CT machine detects adrenal tumors larger than 10 mm in size, and MRI detects tumors even less than 10 mm in diameter.
Ultrasound of the adrenal glands is not very informative, since it can only detect a large tumor - more than 2-3 cm in size.
Treatment of aldosteroma
Patients suffering from an idiopathic form of primary aldosteronism resulting from bilateral diffuse adrenal hyperplasia are prescribed conservative therapy using the drug spironolactone in combination with drugs that lower blood pressure.
Psycho-emotional state after treatment
When treatment is over, you may feel a kaleidoscope of different emotions. This happens to every person who has fought cancer, it is nothing unusual. You begin to think about death more often. Or, perhaps, you will begin to protect your family members more, worry about friends and colleagues who may also face this serious illness. It is possible that you will reconsider your entire system of values and relationships with others. It may happen that anxiety will overcome you in the most unforeseen situations. For example, because you feel better, you will see your doctor less often. For some cancer patients, this fact can almost cause panic.
The most important thing is to understand that life goes on and begin to enjoy every day you live: in this case, you can say that you have won.
Symptoms of adrenal incidentaloma
Incidentalomas in 80% of cases have no clinical manifestations, so patients often have no idea that they have this pathology. Only some neoplasms can manifest clinically (pheochromocytomas, aldosteromas and preclinical Cushing's syndrome). As a rule, patient complaints with this disease can mainly be associated with mechanical compression of nearby organs by the tumor. If the tumor is large, pain may be associated with changes in body position. Typically, such tumors are discovered randomly. In order to promptly identify this disease, the patient must undergo regular preventive examinations and consult an endocrinologist.
Useful video about adrenal tumors
List of sources:
- Baronin A. A. Primary and metastatic tumors of the adrenal glands (clinic, diagnosis, treatment, morphological and biological prognosis factors). Author's abstract. diss. doc. honey. Sci. Ross. AMS, RONC im. N. N. Blokhina. M., 2003.
- Pilkevich O. Ya. Methodological aspects of endosurgical interventions for adrenal tumors. Author's abstract. dis. Ph.D. honey. Sci. St. Petersburg, 2000. – p. 23.
- Cherenkov V. G. Clinical oncology. – 3rd ed. – M.: Medical book, 2010. – 434 p.
Pathogenesis and symptoms of the tumor
The development of pathology in the adrenal cortex occurs with the appearance of the following symptoms:
- Aldosteroma is a tumor that activates a pathological excess of the hormone aldosterone. Its development subsequently turns into Conn's syndrome. Disturbances in muscle structure occur, spasms and convulsions, alkalosis, a quantitative decrease in potassium and alkalization of the blood appear;
- androsteroma - detected when external androgenital syndrome manifests itself: pseudohermaphrodism appears in girls, cessation of menstruation in women, anorexia, dystrophy of the uterus and breasts. Often this situation ends in infertility. In boys, the disorders lead to early puberty and acne throughout the body;
- corticosteroma - a tumor caused by increased secretion of glucocorticoids, developing into Itsenko-Cushing syndrome: obesity, red moon-shaped face due to arterial hypertension, muscle atrophy;
- corticoesteroma is an actively growing malignant tumor that causes estrogen-genital syndrome: women develop male sexual characteristics, and men have complete sexual dysfunction.
A pheochromacytoma appears in the medulla. It affects the nervous and endocrine systems and is detected in a severe state of constant psychosis of varying severity, surges in blood pressure, dizziness, constant fear, pale skin, trembling.
This state is not permanent, it manifests itself spontaneously and also quickly disappears. If this disorder is not detected in time, doctors may not be able to save the patient.
Clinical picture
Treatment tactics are selected based on the nature of the pathology, its size, and stage of development. The treatment regimen also takes into account the individual characteristics of the patient.
Basically, to suppress the tumor process, surgery is used, during which the affected tissue is removed. For adrenal cancer, the following techniques are used:
- Laparoscopy . The tumor is removed through small incisions using a special instrument.
- Transabdominal therapy . Involves making a large incision in the abdominal cavity.
- Thoracobdominal therapy . It is prescribed when the cancerous tumor has grown to a large size. During the operation, the abdominal cavity and chest are cut.
In advanced cases and for medical reasons, when surgical intervention is impossible due to the individual characteristics of the patient (age, etc.), radiation and chemotherapy are prescribed. Both treatment methods cause serious consequences in the form of nausea, vomiting, headaches and other phenomena.
Hormonal therapy is prescribed if other treatment methods are contraindicated for the patient. It is also used to normalize hormonal balance after surgery. Drugs are selected depending on the concentration of which substance is exceeded in the body.
https://youtu.be/J6-fcZr9jLc
Symptoms of adrenal oncology
Each of the described types of tumors has its own characteristics and symptomatic manifestations unique to it.
Albdosteroma
The growth of this tumor produces stable arterial hypertension, pain in the brain, shortness of breath, heart rhythm disturbances, changes in the structure of the myocardium - first hypertrophy, and with the development of the process, its dystrophy. At the same time, such hypertension does not respond to traditional therapy.
The influence of these processes leads to disruption of the visual apparatus - first vasospasms appear, then more frequent ocular hemorrhages occur, which ultimately leads to irreparable degradation and inflammation of the optic nerve.
When the tumor’s production of aldosterone is activated, the following occurs:
- Intense headaches;
- Nausea and vomiting;
- Myopathy;
- Dysfunction of the visual apparatus;
- Respiratory dysfunction;
- Moderate paralysis and paroxysmal tetany.
In addition, hypokalemia develops, with noticeably expressed irrepressible thirst, necturia and polyuria. At the same time, urine acquires a pronounced alkaline reaction. Muscle weakness increases, cramps occur, and over time cell acidosis and atrophy of muscle tissue and nerve endings develop. The development of this condition can lead to coronary pathology and stroke.
According to the reviews of the majority of patients surveyed, their aldosteroma proceeded with mild symptoms or was completely asymptomatic, however, this is only true for the initial stages of the development of the oncological process and, when a certain point is passed, symptoms appear and increase like an avalanche.
Corticosteroma
The clinical course of the disease leads to obesity, fatigue, steroid-type diabetes develops and sexual dysfunction increases. At the same time, microhematomas and striae appear in the area of the mammary glands, abdomen and thighs, in their internal area. Men are characterized by the development of testicular hypoplasia, gynecomastia, and impaired potency, while the weaker sex develops masculine characteristics - a decrease in voice timbre, male-pattern hair growth and an increase in the external size of the clitoris.
As side effects it is worth noting:
- Osteoporosis, leading to increased susceptibility to compression injury of the vertebrae;
- Pyelonephritis;
- Urolithiasis.
In difficult situations, a modification of the mental state is observed - strong causeless agitation or, on the contrary, depression.
Corticoesteroma
Symptoms of this type of tumor in children appear depending on their gender. For example, in boys, the processes of puberty are suppressed, and in girls, on the contrary, it occurs faster than in children of their peers. The female body responds to the development of corticosteroma with premature development of the mammary glands and genital organs, hair growth, early menstruation and accelerated growth of skeletal bone tissue.
Signs of corticoesteroma in men are expressed by symptoms of feminization:
- Degeneration and atrophy of the genital organs;
- Hair loss on the face, chest and pubic area;
- Increased voice timbre;
- Formation of a figure according to the female type;
- Developing infertility due to oligospermia and suppression of potency.
In mature women, the symptoms of this tumor are often very blurred or not noticeable at all. The disease can only be determined by an increase in the content of estrogen in a blood test above normal.
Androsteroma
This tumor produces a large amount of active androgens - testosterone, dehydropiandrosterone, androstenedione and the like, and has a pronounced anabolic and virile effect.
Symptomatic for children:
- Premature puberty;
- Accelerated growth of muscle and skeletal mass;
- Formation of a profuse rash on the face and body;
- Not a childish low timbre of voice.
For mature women, the following signs are characteristic:
- Violation of cyclicity and cessation of monthly cycles;
- Hypotrophy of the mammary glands and uterus with a simultaneous increase in the size of the clitoris;
- Reducing the mass of subcutaneous fat;
- Decreased voice and increased sex drive.
In men, this type of adrenal tumor is, for the most part, detected incidentally, due to extremely mild and subtle manifestations of the disease.
Pheochromocytoma
This tumor is characterized by severe hemodynamic pathologies. During the paroxysmal course of the disease, the following is observed:
- Paroxysmal bursts of arterial hypertension, accompanied by severe headaches, dizziness, and heart rhythm disturbances;
- Bleeding of the skin – pallor;
- Increased sweating;
- Nausea and vomiting;
- Polyuria;
- Pain in the chest area;
- High body temperature;
- Unreasonable panic attacks.
High physical activity, overeating, alcohol and any severe stress can lead to a paroxysmal attack. The duration of such a crisis is several hours and can be systematically repeated with varying regularity - from several times a day, to once during a month or even several.
Such a crisis arises and ends almost instantly - the rapid increase in its symptoms is replaced by an equally rapid normalization of processes. At this time, there is a strong secretion of saliva and sweat.
Unclassified adrenal tumors
Such neoplasms include tumors that do not give symptoms of feminization or virilization, the course of which is asymptomatic or does not have a clear histological classification. These neoplasms are detected for the most part by chance, during a hardware examination of the peritoneum for diagnosing diseases of a different nature.
Metastases
A tumor in the adrenal glands often forms as a secondary focus of a malignant disease. This happens because metastases form in organs: cancer cells penetrate into the blood and lymph, and then provoke the development of malignant cells in a new place or places. The kidneys and adrenal glands are permeated with blood vessels, as they release hormones into the bloodstream, and for this to happen effectively, the blood flow near these organs must be large. Therefore, the small adrenal gland is often the site of the emergence of a new focus of the disease. Metastases in the adrenal glands and kidneys are not always malignant, so serious diagnosis is needed before starting treatment, especially if we are talking about surgical intervention.
Treatment of adrenal cancer in Moscow
Yusupov Hospital is a specialized center for the treatment of adrenal cancer in Moscow and the Moscow region. It employs leading oncologists and endocrinologists. Many doctors have scientific titles and the highest medical category. The cost of operations at the Yusupov Hospital is lower than in other clinics in Moscow. The price of examination and treatment corresponds to the quality of the services provided.
If you have signs that resemble those of adrenocortical cancer, call the Yusupov Hospital. You will be scheduled for an appointment with an endocrinologist-oncologist at a time convenient for you. After the examination, professors and doctors of the highest category will make a collegial decision on treatment tactics.
Author
Yulia Vladimirovna Kuznetsova
Oncologist
Diagnosis of the disease
Usually with the above symptoms they come to an endocrinologist or oncologist. Adrenal cancer is difficult to diagnose; if a doctor suspects it, he recommends all diagnostic methods. Primary diagnosis begins with a general examination, including questioning the patient, visual examination and palpation. The diagnosis is further clarified with the help of additional studies and analyses:
- An X-ray will reveal the presence of metastases in places where there should not be organs or tissue compaction. Possible sites of metastasis include the kidney, liver and lung. This allows us to exclude the most dangerous of metastases.
- Ultrasound is also used to determine the disease: normally, the adrenal glands are not visible during examination. If they are visualized, then there are reasons for alarm. Ultrasound also reveals cancer damage to the lymph nodes and liver.
- CT is the best method; it determines not only the location of the cancerous tumor and accurately visualizes it, but also indicates the degree of malignancy in neighboring tissues. Used before surgery to determine the method, plan and course of the operation.
- MRI determines the composition of the tumor, its structure and the degree of damage to the adrenal gland. The study helps determine whether there are metastases in the spinal cord and brain.
- With MRI and CT, the method of contrast staining of blood vessels works well, helping to notice disturbances in the blood supply to the kidneys and adrenal glands. These organs are actively supplied with blood, so the condition of the vessels next to them will give a fairly accurate picture showing the condition of the organs themselves.
- A biopsy of adrenal tissue is taken, and then the collected material is analyzed for the presence of cancer cells. The most accurate test when it comes to checking for tumor malignancy.
- The results of histological tissue analysis will show how aggressive the tumor is and what the likelihood of metastases is.
- Analysis of urine. If the analysis reveals that the cortisol level is increased, it means that the functioning of the adrenal glands is impaired.
- A blood test for hormones (primarily cortisol, renin and chromogranin) will determine whether the tumor is a primary tumor or metastasis.
- PET (positron emission tomography) is a contrast study using labeled glucose molecules. Cancer cells will absorb it more actively, and this will be reflected in the scanner. This test reflects the size and extent of the cancer and the operability of the tumor.
- An indicator that the tumor is malignant (the issue of danger to life, doctors must decide first of all) will be the weight of the tumor. A tumor that is not life-threatening for the patient weighs about 30-50 g. A malignant formation is heavier than one hundred grams.
When you see a doctor on time, cancer is detected at an early stage thanks to modern equipment and diagnostic methods. If the first stages of the disease are caught, this simplifies treatment and improves the prognosis for the patient.
Prevention
Preventive measures are aimed at eliminating the possibility of relapse of the pathology. At the same time, achieving this goal is quite difficult, since the true reasons that provoke the development of adrenal tumors have not been established.
If the formation has not begun to metastasize, then the patients’ vital functions are restored: previous fertility indicators and other things return. After surgery, patients are recommended to:
- exclude the use of sleeping pills and alcohol;
- monitor your nervous and physical condition, avoiding overexertion;
- follow a diet, limiting the consumption of fatty and spicy foods.
It is also necessary to visit an endocrinologist every six months in order to correct restorative therapy and prevent relapses. If any problems arise, you should consult your doctor promptly.
Causes
Doctors have still not been able to identify the true cause of this disease, but a number of theoretical assumptions have been made on this matter. The following causes of pathology are identified:
- improper diet;
- abuse of fatty, sweet, sour and salty foods;
- lack of physical activity;
- genetic predisposition;
- presence of nicotine and alcohol addiction;
- mental tension, stress, insomnia;
- mechanical and chemical effects on the organ that is the source of the disease;
- increased blood pressure;
- polluted environment;
- diseases of the internal organs of the gastrointestinal tract.
Pathology of the adrenal gland can occur due to the spread of cancerous tissue structures of the adjacent affected internal organ.
Complications
The danger of neoplasms in the corresponding endocrine glands lies in hormonal imbalance and complex dysfunction of the body.
Complications:
- Infertility.
- Stroke, heart attack.
- Acute cardiac or adrenal failure.
- Arrhythmia.
The prognosis for the patient additionally depends on the size and functional activity of the tumor. The smaller it is, the better for the patient.
Diagnosis of formations in the adrenal glands
If adrenal cancer is suspected, the following diagnostic measures are prescribed:
- Chest X-ray . Allows to identify metastases in the lungs.
- PET . Provides information about the current stage of development of the tumor, its size and location.
- MRI . Prescribed when it is suspected that metastases have penetrated the spinal cord or brain.
- Ultrasound . Allows detection of adrenal cancer and liver metastases.
- CT scan Creates a visual image of the tumor, through which it is possible to evaluate its structure.
- Histological examination . Allows you to determine the nature of the tumor.
Additionally, urine and blood tests are performed, which show excess levels of certain hormones.
What is an adrenal neoplasm?
Adrenal cancer is a rare disease. For example, in the United States, about 300 cases are diagnosed annually. This is a relatively small figure. Most patients are between the ages of 45 and 50, but no one is immune from the tumor, not even children. Cancer of the organ's cortex, as statistics show, occurs more often in women, and neoplasms of the adrenal medulla affect both men and women equally.
Pathological changes in the left adrenal gland in this disease are the same as those in the right. As a result of adrenal cancer, a variety of changes can occur in the body. Small glands perform an important function for all systems - the synthesis of hormones (adrenaline, aldosterone, norepinephrine, cortisol).
The true cause of the disease has not yet been discovered.
Some scientists, based on numerous studies, suggest that the main provocateurs are mutational changes in DNA.
As a result, tumor suppressors are excluded and oncogenes are included. Hereditary diseases that can affect the development of cancer include:
- endocrine neoplasia;
- Li-Fraumeni syndrome;
- adenomatous polyps;
- Beckwith-Wiedemann syndrome.
The list of additional factors can include:
- smoking;
- obesity;
- external exposure to carcinogens;
- sedentary lifestyle.
Patients with a local (within the gland) type of disease have a greater chance of recovery. Five-year survival in their case is typical for 65% of patients. With the regional variant (cancer spreads to the lymph nodes and nearby tissues), this figure decreases to 44%. In the severe form - distant (active metastasis and cancer affecting other organs) - the prognosis is unfavorable: survival rate is only 7%.
Removal of the aldosteroma along with the affected adrenal gland provides good results in terms of hypertension. Blood pressure is normalized in 70% of cases, and another 30% of patients have moderate hypertension, but without crises. Elimination of androsteres can further lead to short stature.
After complete removal of pheochromocytoma, moderate hypertension and tachycardia may be observed for a long time, which are relatively easy to treat.
Prognosis and survival
The question of how long people live with stage 4 adrenal cancer is particularly relevant, but, unfortunately, not a single doctor can answer it truthfully. Life expectancy depends not only on the stage, but also on the process of metastasis, the age of the patient, the presence of diseases of the internal organs, and the state of health in general.
Of course, in the presence of metastases in adrenal cancer, the prognosis is always disappointing. The chances of living a long and happy life are reduced to zero. For patients with stage 4 adrenal cancer, the five-year survival rate is only 10%.
With small tumor sizes and the absence of metastases, the prognosis is more comforting. More than 70–80% of patients manage to overcome the five-year threshold. If the tumor is of impressive size, but metastasis has not yet started, then the prognosis is reduced to 40–50%, and in case of resection it increases to 60%.
Hormonally inactive formations of the adrenal glands
Malignant or benign tumors do not bother a person with symptomatic manifestations for a long time. They are diagnosed for the most part absolutely by chance during tomography or sonography of other organs of the body. They are called incidentalomas, the meaning of which indicates the rarity of discovering such neoplasms.
The term incidentaloma is not a diagnosis, but only denotes a certain heterogeneous (heterogeneous) group of randomly discovered tumors, each of which must be identified in order to prescribe subsequent treatment.
The following types of tumors are most often diagnosed:
- Neoplasms of the cortex: adenoma, carcinoma and nodular hyperplasia.
- Neoplasms of the medulla: pheochromocytoma, extremely rarely - ganglioneuroblastoma.
- Pathologies of the adrenal glands: neurofibroma, xanthomatosis and amyloidosis, cyst, hematoma and granuloma, lipoma, angiosarcoma.
- Metastases from the lungs or breast.
After detecting an incidentaloma, specialists find out whether the tumor is malignant and whether it affects the production of hormones by the adrenal glands.
Symptoms
Due to the large number of neoplasms included in the group of incidentalomas, the severity of symptoms of adrenal diseases in men can vary quite significantly. But the main signs are the following:
- Obesity.
- Arterial hypertension.
- Diabetes.
- Myalgia.
- Arthralgia.
For volumetric visualization, the tumor is examined using an ultrasound machine or computed tomography.
Surgery to remove a malignant adrenal tumor can save a patient’s life
Treatment
In the presence of a non-malignant tumor less than 3 cm in diameter, surgery is not performed. The patient must visit a doctor every 6 months for examination to detect the lack of growth of the tumor and the possibility of its degeneration. No symptomatic treatment is required. Malignant and non-malignant formations larger than 3 cm must be removed in a specialized hospital.
Brief physiology of the adrenal glands
The adrenal glands are paired organs, each located on top of a kidney. These are endocrine glands that play a vital role in the functioning of body systems. Each adrenal gland consists of two main parts that function separately.
- Adrenal cortex
The outer part produces three main hormones: cortisol, aldosterone and dehydroepiandrosterone. These hormones are designed to carefully control metabolism and certain anatomical and physiological characteristics, such as hair growth and body shape.
- Adrenal medulla
The inner part of the gland that produces adrenaline, norepinephrine and dopamine. These are hormones that control the body's response to stress, including the fight-or-flight system based on the adrenal system.
Pheochromocytoma
Pheochromocytoma is a tumor originating from the adrenal medulla, namely from the so-called chromaffin tissue, which produces catecholamine substances - adrenaline, norepinephrine, dopamine. The second name for this formation is chromaffinoma.
It is important to know that in the process of tumor degeneration of chromaffin tissue, in addition to catecholamines, other substances, such as adrenocorticotropic hormone or serotonin, can be produced in large quantities: this introduces significant diversity into the clinical picture of the disease and complicates diagnosis.
Unfortunately, about 60% of cases of pheochromocytoma are diagnosed posthumously. In 9 out of 10 patients, the location of the tumor is typical - the adrenal glands (usually on one side, less often on both sides), and in 10% of patients the tumor is localized in other parts of the body. The most typical places of extra-adrenal localization of chromaffin tissue are:
- sympathetic nerve trunk;
- aortic arch, abdominal aorta;
- diaphragm;
- spleen;
- kidneys;
- ovaries and testicles;
- bladder.
As a rule, pheochromocytoma is a benign neoplasm, but there is also a malignant form called pheochromoblastoma.
Causes and mechanisms of the disease
Unfortunately, it is impossible to say for sure why pheochromocytoma occurs. There is probably a genetic predisposition to this pathology, since familial cases of the disease are not uncommon.
The mechanism of development of chromaffinoma is associated with increased production of catecholamines by tumor cells - adrenaline, norepinephrine and dopamine. At the time of crisis, the level of these substances in the blood increases significantly - often their concentration exceeds the normal tens of times.
The main effects of catecholamines are an increase in blood pressure and an intensification of metabolic processes. Under the influence of these hormones, a sudden sharp spasm of blood vessels occurs and the heart rate increases. These changes lead to a sharp increase in both systolic and diastolic pressure to high numbers. Not only large vessels spasm, but also vessels of the skin and mucous membranes, abdominal organs, and muscles. The lumen of the bronchi and intestines expands, the process of breaking down glycogen into glucose in the liver accelerates. Changes in the myocardium are characterized by the development of catecholamine myocardial dystrophy and arrhythmia. The processes of metabolism, heat production, breakdown of fats and glycogen are accelerated, and the effects of insulin are weakened.
Pathomorphology of pheochromocytoma
Benign pheochromocytoma, as a rule, has a unilateral localization and is a formation no more than 5 cm in diameter and 100 g in weight. It grows gradually, invasive growth is not typical.
Pheochromoblastoma often reaches enormous dimensions - up to 30 cm in diameter and weighing 2 kg or more. It is fused to the surrounding tissues and covered with a capsule of uneven thickness. It is characterized by rapid growth, grows into surrounding organs and tissues, and metastasizes through the blood and lymph flow. The location of the tumor is usually bilateral. Not one, but several neoplasms may be present simultaneously.
There is also a conditionally malignant type of pheochromoblastoma. This tumor, in its micro- and macro-characteristics, occupies an intermediate place between benign and malignant forms. This variant of pheochromocytoma is the most common.
Pheochromocytoma may be accompanied by hyperplasia of the adrenal medulla.
Clinical manifestations of pheochromocytoma
The classic clinical picture of pheochromocytoma is peroxysmal (attacks) arterial hypertension in combination with metabolic and autonomic symptoms, such as:
- severe headache;
- pain in the heart area;
- general weakness;
- body shaking - tremor;
- paresthesia (tingling, burning, tingling sensation in the skin);
- dizziness;
- heartbeat;
- feelings of fear and anxiety;
- sweating;
- pallor or hyperemia (redness) of the skin;
- feeling of heat;
- pain in the stomach;
- nausea;
- vomit;
- dyspnea;
- excessive urine production;
- visual impairment;
- convulsions.
Depending on the characteristics of the disease, there are 4 forms of pheochromocytoma.
- Classic - paroxysmal - form. It is characterized by attacks of hypertension that occur against a background of normal blood pressure. Attacks last from 2-3 minutes to half an hour, occur at intervals from once every 2-3 months to 20 times a day. As the disease progresses, the frequency, duration and intensity of attacks increase. An attack is provoked by the following actions:
- eating;
- physical activity;
- emotional stress;
- palpation of the tumor localization area;
- injuries;
- changing position in bed;
- surgical interventions;
- pregnancy and childbirth.
The attack is usually preceded by an “aura” in the form of paresthesia, muscle tremors, and shooting pain in the abdominal area. After this, headaches, squeezing pains in the heart area, and palpitations appear and quickly increase. Patients may also experience flickering and double vision, pain in the lower back and abdomen. The patient is excited, experiences a painful fear of death, and screams. His skin is pale and covered with cold sweat. All these changes occur against the background of an increase in blood pressure to a level of 280-360/180 mm Hg. Art. The pulse is arrhythmic. At the end of the attack, redness of the skin, profuse sweat, salivation and lacrimation, nausea, vomiting, excessive urination, and severe general weakness are noted. As the classic form of the disease progresses, secondary changes occur in the cardiovascular system and kidneys, leading to a steady increase in blood pressure.
- Mixed form. Hypertensive crises do occur, but are less pronounced, since initially blood pressure is already moderately elevated.
- Permanent form. Clinically similar to essential arterial hypertension (with essential hypertension). It is most common, accounting for about 65% of all cases of pheochromocytoma.
- Disguised form. Due to the influence of catecholamines on metabolism, the disease may not proceed in a typical manner, hiding under the guise of other diseases. The leading syndromes for this form of the disease are:
- cardiovascular (arterial hypertension is accompanied by increased heart rate, and upon auscultation of the heart, the sounds are muffled, a systolic murmur is detected at the apex, an accent of the second tone at the apex; changes in cardiogram parameters are also diagnosed);
- psycho-neurovegetative syndrome (headache and dizziness, tremor, sweating, paresthesia, general weakness, fatigue, pallor, fear, and so on);
- abdominal syndrome (salivation, nausea and vomiting, abdominal pain during meals; sometimes signs of an “acute abdomen”);
- endocrine-metabolic syndrome (weight loss up to cachexia, development of symptomatic diabetes, menstrual irregularities);
- tumor syndrome (abdominal pain in the projection of the tumor location, inferior vena cava syndrome (dizziness and loss of consciousness when lying on the stomach), palpable tumor in the abdomen).
If a pregnant woman has pheochromocytoma, it can simulate late gestosis - up to eclampsia, or be combined with it. In the absence of timely diagnosis, in 50% of cases both mother and fetus die. A pheochromocytoma diagnosed during pregnancy is a direct indication for its termination or premature delivery.
In pediatric patients, chromaffinoma occurs without its typical paroxysms, but is characterized by a persistent increase in blood pressure. Children's vision is also impaired: when examined by an ophthalmologist, hemorrhages are detected on the retina.
Diagnosis of pheochromocytoma
The clinical picture described above allows the doctor to suspect the disease. To confirm the diagnosis, a biochemical blood test is performed, determining the level of adrenaline, norepinephrine and dopamine. With pheochromocytoma, the content of these substances in the blood can increase even tenfold.
Against the background of an increase in catecholamines in the blood, the content of them, as well as their metabolic product, vanillylmandelic acid (VMA), also increases in the urine. The condition is to collect urine either within the first three hours after the crisis, or within 24 hours.
To make an accurate diagnosis, the above studies must be repeated 3-4 times.
Functional tests can also be carried out with histamine, glucagon (these substances provoke the release of adrenaline by the adrenal glands) or tropafen, regitin, clonidine (block the vasoconstrictor effect of catecholamines).
In addition, if you take blood for analysis at the time of an attack, it will reveal an increased content of leukocytes (leukocytosis) and glucose.
For the purpose of topical diagnosis, as with other adrenal tumors, computed tomography or magnetic resonance imaging is used. When pheochromocytoma is localized outside the adrenal glands, scintigraphy (scanning) is performed with preliminary introduction into the body of a substance that accumulates in chromaffin tissue, or an angiographic study. Ultrasound in this case is not very informative.
Treatment of pheochromocytoma
The main treatment method for chromaffinoma is surgery involving unilateral adrenalectomy (removal of the adrenal gland from the affected side) along with the tumor. The criterion for complete tumor removal is absolute regression of symptoms and normalization of catecholamine levels in the blood.
In case of adrenal crisis, the patient must be administered an adrenolytic - phentolamine. It is administered in a certain dosage every 5-10 minutes until the crisis is completely relieved. Once the goal is achieved, the same dose of the drug is administered once every 2-4 hours for 24 hours, and then the patient is transferred to oral administration immediately before surgery. If palpitations or arrhythmias persist while taking adrenaline, a β-blocker is added to treatment.
Forecast
As was said at the beginning of the article, 60% of patients die without knowing their diagnosis. The causes of death are, as a rule, severe vascular complications: strokes and heart attacks against the background of uncontrolled arterial hypertension.
With timely surgical treatment, five-year survival is observed in more than 95% of cases. Sometimes - in every tenth patient - unfortunately, relapses occur.
Survival prognosis
When diagnosed with adrenal cancer, much is determined by the current stage of the cancer and the degree of spread of cancer cells. But even with proper treatment and successful surgery, there remains a high probability of relapse. According to statistics, if the cancer is stage 1, the probability that the patient will survive is 80%; in other cases, treatment does not give visible results. If we are talking about stage 2, the chance is reduced to 50%. Stage 3 - 20-25%, and stage 4 only 10%, since uncontrolled metastasis has developed.
A separate prognosis is made if adrenal carcinoma is detected, which negatively affects the patient’s life. Even if it was detected and operated on in time, patients with this diagnosis live less than 1.5 years.
If treatment for adrenal cancer is successful, the patient will need to maintain a healthy condition with ongoing drug therapy. Patients are prescribed hormonal drugs that maintain the balance of substances in the body, but their use is associated with obesity.
Therefore, the outcome is similar to other cancers: the earlier the tumor is detected, the greater the likelihood that the patient will survive. For different types of cancer, prognosis statistics vary, as well as the rate of disease development and characteristic symptoms. The first stage is the most favorable time for the patient, and the last stage usually comes with a negative prognosis.
How to diagnose
Today, there are a number of techniques that provide informative diagnostics, allowing both to determine the presence of a tumor and to clarify its location and nature:
- The degree of tumor activity can be determined thanks to the hormonal level; the daily amount of homovanillic and vanillylmandelic acid in urine is also examined.
- If there is a suspicion that a patient has pheochromocytoma, blood and urine sampling for testing should be carried out directly during the crisis or immediately after it ends. This approach will make it possible to accurately determine the content of catecholamines.
- Instrumental methods that allow obtaining the most reliable information include selective venography.
- When scanning using ultrasound or using a tomograph, it is possible to determine the diameter of the lesion and its exact location, the presence of secondary lesions.
Thanks to hardware techniques, doctors are able to detect hormonally inactive neoplasms with sizes not exceeding 5 mm. As for measures to eliminate pathology, symptoms and treatment in this matter are interrelated.
Hormone-producing tumors
The tumor - aldosteroma , leads to a disruption of the mineral-salt balance of the body, since it produces large quantities of the hormone - aldosterone. Its excess leads to muscle atrophy, hypertension, hypoglycemia and alkalosis. The vast majority of cases of detection of such neoplasms occur in single tumors, and approximately a tenth of them have multiple foci on one or both adrenal glands. No more than 4% of all cases are malignant.
Glucosteroma is a tumor that produces a secretion - glucocorticoid. Its focus grows in the fascicular area of the adrenal cortex and leads to premature maturation of the genital organs in children, decreased libido and sexual function in mature patients. In addition, glucosteroma manifests itself in arterial hypertension and obesity. This type of tumor can also have a dual nature - benign and malignant and is considered the most common oncopathology of the adrenal cortical tissue.
Corticoesteroma grows from the cortical tissues of the reticular and fascicular areas and secretes secretions - estrogens - in the form of products of its vital activity, and this leads to the development of sexual dysfunction in men and the restructuring of the female hormonal background according to the male principle. Most often, such an adrenal tumor is malignant in nature, develops quickly and aggressively, and is detected mainly in men at a young age.
Androsteroma is localized, as a rule, in the ectopic area of the adrenal gland, somewhat less often in the reticular area of the cortex. It produces the hormone androgen in large quantities. For women, this results in symptoms of virilization, for girls in pseudohermaphroditism, and the consequences of the development of this tumor for the male sex are accelerated puberty. Androsteromas are twice as likely to affect the weaker sex, mainly under the age of 40, and more than half of those diagnosed with androsteromas turn out to be malignant. In the latter case, the development of the tumor is extremely aggressive, with early production of metastases in the liver, lungs and regional lymph nodes.
Pheochromocytoma is a neoplasm, in most cases affecting cells of brain tissue, less often tissue of the neuroendocrine system, accompanied by autonomic disorders. In nine out of ten patients, the identified phoechromocytoma is benign in nature, however, some of these tumors are prone to degenerate into malignant ones - approximately 10 per hundred cases. This type of tumor has a pronounced hereditary predisposition and is characteristic primarily of the female sex in the period 30–50 years.