© Author: A. Olesya Valerievna, candidate of medical sciences, practicing physician, teacher at a medical university, especially for SosudInfo.ru (about the authors)
Intestinal infarction is a necrotic process caused by blockage of the arterial or venous trunks supplying the organ. Acute disruption of blood flow causes gangrene and rapid development of peritonitis, and mortality reaches 100%.
Thrombosis of mesenteric vessels (which is the main cause of intestinal infarctions) is a very dangerous phenomenon, the frequency of this pathology is inexorably growing. More than half of the patients are women, the average age of patients is about 70 years. Age plays a significant aggravating role, because radical operations in older people can be risky due to severe concomitant diseases.
An intestinal infarction develops similarly to a heart or brain infarction. Unlike the latter, one hears much less often about acute disruption of blood flow in the vessels of the mesentery. Meanwhile, despite the availability of modern diagnostic methods and the development of new treatment methods, mortality from intestinal vascular thrombosis continues to remain high, even with urgent surgery.
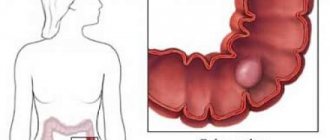
blood supply to the intestine – small (left) and large (right)
The severity of the pathology, the rapidity of development of irreversible changes, and the high probability of death require specialists to pay close attention to people at risk, and these are elderly patients with atherosclerosis, hypertension, and heart failure, who make up the majority among the population of many countries.
Kinds
Depending on the etiology of occurrence, intestinal necrosis can be:
- Ischemic (the term “intestinal infarction” is synonymous). The cause of the ischemic necrotic process is blockage of large blood vessels (arteries and veins) supplying blood to the intestines. In case of acute disturbance of blood flow, the patient quickly develops gangrene and peritonitis, and the mortality rate approaches 100%.
- Toxigenic , arising as a result of microbial infection of the intestines of the gestating fetus with coronaviruses, fungi of the genus Candida, rotaviruses, bacteria of the genus Clostridia.
- Trophoneurotic , provoked by certain diseases of the central nervous system.
The presence of clinical and morphological signs is the basis for identifying the following types of intestinal necrosis:
- Coagulation (or dry), developing as a result of coagulation (clotting) of proteins and dehydration of tissues. Atrophying intestinal tissues, becoming dense and dry, begin to separate from healthy structures. The impetus for the emergence of this type of pathology, which does not have any special clinical manifestations, is chronic arterial insufficiency. The most unfavorable option for resolving coagulative necrosis is its transformation into a wet-type pathology.
- Colliquation (wet). A characteristic manifestation of wet necrosis is the active proliferation of putrefactive microflora in the cells of dead tissue, provoking the development of extremely painful symptoms. Since liquefaction necrosis is fraught with the development of gangrene, its treatment requires mandatory surgical intervention.
- Strangulation , caused by acute intestinal obstruction, which can be caused by blockage of the intestinal lumen with a foreign body or intestinal contents that have difficulty evacuating. A fairly common cause of intestinal obstruction is pathological processes occurring in the structures of the intestinal walls. Another factor contributing to the occurrence of this pathology is compression of the intestinal tube from the outside (usually by rapidly growing tumors that have affected nearby organs). Strangulated intestinal obstruction can occur as a result of significant narrowing of the intestinal lumen and thrombosis of the mesenteric vessels, provoking circulatory disorders, the development of necrosis of the intestinal walls and peritonitis (inflammation of the peritoneum).
Photo of gangrenous necrosis of a section of the small intestine
- A fairly common type of intestinal necrosis is gangrene , characterized by the presence of communication with the external environment, the development of an infectious process provoked by putrefactive bacteria and leading to rejection of dead tissue. Gangrene has two forms: dry and wet. Dry gangrene is characterized by impaired blood circulation, wet gangrene - by the presence of edema, venous and lymphatic stasis (impaired outflow of blood from the veins and lymphatic fluid from the lymphatic capillaries and vessels).
Classification
Based on the etiology of the disease, the following forms are distinguished:
- ischemic intestinal necrosis - the etiology is based on intestinal infarction, and in the acute form of necrosis, peritonitis quickly develops and the probability of death is very high;
- toxicogenic – develops against the background of intestinal damage by infection, pathogenic microorganisms;
- trophoneurotic – develops due to diseases of the nervous system.
Based on localization, the following forms of this disease are distinguished:
- necrosis of the large intestine;
- necrosis of the small intestine;
- necrosis of the fatty pendant of the sigmoid colon;
- necrosis of the rectum.
Based on clinical and morphological characteristics, the following types of pathology are distinguished:
- coagulative necrosis;
- colliquation;
- strangulation;
- gangrenous.
The following stages of development of this pathological process are also distinguished:
- prenecrosis - a stage at which a slight change in tissue occurs, there is no threat to life;
- tissue death - destruction of tissue cells occurs, the process is already irreversible;
- tissue breakdown.
It should be noted that the last stage of the disease almost always leads to death.
Causes of tissue necrosis
Irreversible necrosis of intestinal tissue can be caused by infectious, mechanical or toxic factors, most often represented by:
1. Impaired blood circulation in the vessels supplying the intestinal walls and leading to intestinal infarction. The cause of cessation of blood flow can be thrombosis (blockage of the lumen of a blood vessel by a formed thrombus) or embolism (blockage caused by a foreign body or an air bubble that has penetrated into the bloodstream). In any case, the death of cells in bloodless tissues occurs as a result of their intoxication with decay products, an acute lack of oxygen and nutrients.
- As a rule, blockage of the vessels supplying the intestinal walls occurs in patients suffering from severe diseases of the heart muscle. Mostly elderly women are at risk.
- The realities of our time are such that intestinal infarction, often the culprit of necrosis, is increasingly affecting young people. According to statistics, in every tenth case the patient is under thirty years of age. Impaired blood flow can cause total necrosis, ending in death in half of the patients suffering from infarction of the small or large intestine.
- One of the most dangerous pathologies is thrombosis of the mesenteric vessels, which supply blood to both the large and small intestines, since in this case it is not just some part of the intestine that will fail, but the entire organ. The insidiousness of mesenteric infarction lies in its complete asymptomatic occurrence in the early stages of the disease. Clinical manifestations of the pathology are absent until the development of total necrosis, which claims the lives of 70% of patients.
2. Intestinal obstruction resulting from intestinal volvulus - a most dangerous condition in which compression and twisting of the blood vessels of the intestinal walls (along with the affected intestine itself) is observed. Loops of the large intestine are most often affected by volvulus; the small intestine suffers from it much less frequently. The impetus for its occurrence can be a full intestine, overeating and severe tension in the abdominal muscles that accompanies any excessive physical activity (for example, lifting a heavy object or a high jump).
3. Exposure to pathogenic microflora. A striking representative of this pathology is necrotizing enterocolitis, which occurs mainly in newborn infants and affects the intestinal mucous membranes. A characteristic feature of necrotizing enterocolitis is not total, but focal development. In the absence of timely treatment, the necrotic process, initially localized in the epithelial layer, can spread to the entire thickness of the intestinal wall. In case of intestinal damage by bacteria of the genus Clostridium, a rapid development of a necrotic process is observed, quickly leading to pneumatosis (a rare pathology characterized by the accumulation of gases with the formation of cavities - air cysts) and intestinal gangrene, fraught with perforation of the intestinal walls. Pathologies that follow this scenario often result in death.
4. Dysfunction (malfunctions) and diseases of the central nervous system, provoking dystrophic changes in the structures of the intestinal walls (up to the occurrence of necrosis).
5. An allergic reaction to the presence of foreign bodies in the digestive tract.
6. Exposure to certain chemicals.
7. Surgery on the stomach.
Prevention
Recommendations are made when the causes of necrosis are identified. You need to try not to get food and drug poisoning, eat right, add more fruits and vegetables to your diet, and exclude solid foods. Avoid fatty and sweet foods. Quit smoking and drinking alcohol. Start treatment for various diseases of the digestive tract and central nervous system in a timely manner.
To deliver missing nutrients to the body, doctors prescribe parenteral nutrition. Pay special attention to your health, pay attention to painful sensations, do not treat at home and do not delay seeking help from medical specialists. Everyone should know what intestinal necrosis is, its symptoms and principles. This could save the life of your loved one or yourself. Take care of your health and be happy!
If you find an error, please select a piece of text and press Ctrl+Enter.
Intestinal necrosis is the death of organ tissue due to cessation of blood flow. Accompanied by severe intoxication and a sharp deterioration in general condition. Intestinal necrosis is irreversible and can be fatal. If pathology is detected, emergency surgical intervention is indicated.
Symptoms of intestinal necrosis
Tissue death during intestinal necrosis is accompanied by:
- increased fatigue;
- general weakness and malaise;
- decreased immunity;
- high body temperature;
- decreased blood pressure (hypotension);
- increased heart rate;
- the presence of nausea or vomiting;
- dry mouth;
- significant reduction in body weight;
- cyanosis and pallor of the skin;
- a feeling of numbness and lack of sensitivity in the affected organ;
- increased urge to have bowel movements;
- the appearance of blood in the stool;
- dysfunction of the liver and kidneys.
If the disruption of blood flow occurs not in the artery, but in the vein of the affected intestine, the patient will experience vague discomfort in the abdominal area, and the increase in his body temperature will be insignificant.
The occurrence of sudden, painful and sharp pain in the abdomen indicates the presence of necrosis caused by intestinal infarction. Unlike the pain that accompanies pancreatitis, it is not girdling and is often accompanied by nausea or vomiting. In an attempt to alleviate his condition, the patient tries to change the position of his body, but none of them brings relief.
Necrosis that affects the intestinal walls leads to a change in their odor and color: they become white or whitish-yellow. In patients with intestinal infarction, necrotic tissue soaked in blood appears dark red.
In patients with necrosis that arose against the background of intestinal volvulus, the symptoms are completely different:
- They often experience penetration of intestinal contents into the stomach, causing vomiting, characterized by the specific smell of vomit.
- Against the background of a complete absence of stool, active discharge of gases is observed, despite which the patient’s abdomen swells, becoming asymmetrical. During a physical examination of the patient, a specialist who palpates the abdomen may detect the presence of abnormally soft areas.
The condition of patients with necrosis, provoked by the influence of pathogenic microorganisms or circulatory disorders, is sharply complicated by the addition of clinical manifestations of peritonitis:
- the color of the skin acquires a grayish tint;
- there is a drop in blood pressure;
- the heart rate increases (tachycardia develops).
The stages in the development of intestinal necrosis are:
- Pre-necrosis, characterized by the presence of changes in tissues that are reversible.
- Tissue death. Pathology that has entered this stage of development is accompanied by the death of affected cells; the affected areas of the intestine change their color.
- Tissue breakdown.
- Diagnosis of intestinal necrosis begins with a thorough history taking, including examination of the nature of feces, clarification of the frequency of bowel movements, identification of factors contributing to increased gas formation and bloating, clarification of the nature of abdominal pain and the frequency of their occurrence.
- During a physical examination of the patient, which includes mandatory palpation of the abdomen, at the location of the necrotic zone, the gastroenterologist may detect a painful area that does not have clear boundaries.
Plantain decoction
Plantain is an affordable medicinal plant that has:
- antibacterial and anti-inflammatory effects;
- antitumor effect;
- analgesic properties.
To prepare the decoction you need:
- Pour 2 tbsp. leaves into a small warming container.
- Pour 250 ml of hot water over them.
- Cook in a water bath for about 30 minutes. under the lid.
It is recommended to drink the drink 0.5 cups after meals 3 times a day.
Rose hips contain many vitamins, carotene and organic acids. Due to its composition, rosehip has strengthening and astringent properties, which determines its use in treating the intestines. Infusions from this plant actively help eliminate nausea and vomiting.
They are prepared simply:
- 20-25 dry berries are crushed and poured into a small saucepan.
- Next, the mixture is poured with 350 ml of boiling water.
- Leave for 3-4 hours.
- Decant and drink the infusion 1-2 times a day.
Decoctions and infusions of rose hips are also used in the presence of blood in the stool. During the period of remission of diseases of the sigmoid colon, the concentration of berries can be increased.
Diagnostics
- Diagnosis of intestinal necrosis begins with a thorough history taking, including examination of the nature of feces, clarification of the frequency of bowel movements, identification of factors contributing to increased gas formation and bloating, clarification of the nature of abdominal pain and the frequency of their occurrence.
- During a physical examination of the patient, which includes mandatory palpation of the abdomen, at the location of the necrotic zone, the gastroenterologist may detect a painful area that does not have clear boundaries.
Laboratory blood testing is of little use for screening and early diagnosis of intestinal necrosis, since clinically significant changes begin to appear only with tissue necrosis.
However, the diagnostic examination of the patient involves the following:
- General blood test. At the initial stage of pathology, it may be within normal limits. In the final stages of intestinal necrosis, it will indicate the presence of leukocytosis and a high erythrocyte sedimentation rate (ESR).
- Biochemical blood test.
- Coagulograms are a special study of the blood coagulation system. The presence of acute intestinal ischemia may be indicated by an increased level of D-dimer, a small protein fragment formed as a result of the breakdown of fibrin and found in the blood after the destruction of blood clots.
To make an error-free diagnosis, a whole range of instrumental studies is required, which requires:
- X-rays. This procedure is most informative at the second and third stages of intestinal necrosis, while at the initial stage the pathology, even accompanied by pronounced clinical symptoms, is not always detectable.
- Radioisotope scanning, prescribed in cases where radiography has not yielded any results. Before performing the procedure, a drug containing a radioactive substance – an isotope of technetium – is injected intravenously into the patient’s body. After a few hours, the zones of radioactivity that have arisen in the patient’s body are recorded. An area of the intestine affected by a necrotic process and therefore deprived of blood circulation will appear as a “cold” spot in the image.
- Angiography or magnetic resonance angiography are computer procedures that involve introducing a specially colored substance into the bloodstream and taking pictures using a computer or magnetic resonance tomograph. These diagnostic procedures make it possible to identify problem areas of the intestine that have clogged vessels.
- Dopplerography is an ultrasound examination performed using a Doppler apparatus, which makes it possible to establish the speed of blood flow in the intestinal arteries and, based on the data obtained, to identify possible disturbances in the blood supply to any part of the large or small intestine at the earliest stages of pathology.
- Contrast radiography, which reveals the width of the lumens of the intestinal blood vessels. Before X-rays are taken, a contrast agent is administered intravenously.
- Diagnostic laparoscopy of the intestine is a surgical research technique that allows a specialist to assess the condition of this organ without resorting to making large incisions in the anterior abdominal wall. Three small punctures are made in the patient's abdominal wall using a thin tube (trocar). Through one trocar, a telescope tube is inserted, equipped with a light source and a miniature video camera connected to a high-magnification monitor. Thanks to these devices, the doctor can see the organ being examined and control the progress of the manipulations being performed. Two other trocars are needed to insert special instruments (manipulators). During laparoscopy, a biopsy and puncture of intestinal vessels can be performed. Tissue samples are subjected to further histological examination.
- Colonoscopy is an endoscopic examination of the large intestine, carried out using an optical probe or a special device - a flexible and soft fiber colonoscope. Due to the significant (up to 160 cm) length of its tube, the endoscopist can examine the large intestine along its entire length. The fiber colonoscope has a cold light source (which does not burn the intestinal mucous membranes during the procedure) and a portable optical system that transmits a greatly enlarged image to a special screen, allowing the specialist to carry out any actions under visual control. Given the significant pain of the procedure, it is carried out under local anesthesia, using dicaine ointment and special gels containing lidocaine: Luan, Xylocaine, Kategel, etc.
- A study called “diagnostic surgery” has recently become firmly established in the practice of many modern clinics. Having discovered necrotic tissues during the procedure, the specialist begins to immediately remove them.
Forecast
The prognosis for intestinal necrosis depends on the timeliness of the patient seeking medical help. At the first stage of the disease, recovery is achieved in the vast majority of cases. The number of patients seen at this stage of the disease is minimal.
Surgical treatment of intestinal necrosis does not guarantee recovery. Only 50% of patients manage to return to their usual rhythm of life after surgery. A third of them have postoperative complications: adhesions, suppuration, bleeding.
Treatment
A doctor treating necrosis will first take into account:
- type and form of pathology;
- stage of the disease;
- the presence or absence of concomitant diseases.
Complete healing of a patient suffering from intestinal necrosis, which can lead to the restoration of lost health, is quite possible, but for this the disease must be identified at one of the early stages.
There are different methods of treating this serious pathology, the choice of which depends on the preferences of the treating specialist. Regardless of the etiology of intestinal necrosis, the patient suffering from it should be immediately hospitalized in a surgical hospital.
A patient admitted to the clinic first goes through the procedure of plain radiography of the abdominal cavity or radiocontrast irrigography (for this, a radiopaque substance - a suspension of barium sulfate - is introduced into his body using an enema).
The absence of symptoms of inflammation of the peritoneum (peritonitis) is the basis for starting conservative treatment, carried out under the guidance of a surgeon. Conservative therapy involves introducing into the patient’s body:
- electrolytes;
- protein solutions;
- antibiotics that prevent the active proliferation of putrefactive bacteria;
- anticoagulants (drugs that reduce blood clotting) that prevent thrombosis of blood vessels.
Simultaneously with drug treatment, all (both upper and lower) parts of the digestive tract are washed with the help of special probes.
To reduce the load on the affected areas, intestinal intubation (probing) is performed - a procedure during which a thin tube is inserted into the intestinal lumen, designed to suck out the contents from the distended and overcrowded intestine.
A tube is inserted into the small intestine through:
- nose;
- mouth;
- gastrostomy (an artificially formed opening in the anterior wall of the abdomen and stomach);
- ileostomy (small intestine removed and surgically attached to the anterior wall of the abdomen).
Intubation of the large intestine is carried out through the anal canal or through a colostomy (an unnatural anus created by bringing the end of the sigmoid or colon onto the abdominal wall).
Great importance is given to detoxifying the body and eliminating the consequences of dehydration.
If conservative treatment does not give the expected result, the patient undergoes resection - a surgical operation to remove part of the intestine affected by necrosis. During resection, either an individual dead loop or an entire section of the small or large intestine can be removed.
Resection of the small intestine belongs to the category of rare surgical interventions necessary in cases where necrosis is a consequence of intestinal obstruction or fusion of the walls of this organ.
Resection of the large intestine may require a colostomy, an artificial anus to pass stool.
During the long postoperative period, the patient is prescribed a course of antibiotics and detoxification therapy, as well as correction of possible digestive disorders.
Polyps
Polyps are tumor-like growths on the intestinal mucosa, often affecting the sigmoid region. Polyps have different structures and shapes. In most cases, such growths are amenable to treatment or surgery. The outcome of therapy is favorable. Signs of polyp formation appear only in the acute stage, when polyps interfere with the normal passage of feces.
Patients note:
- constipation and diarrhea;
- blood impurities in stool;
- a large amount of mucus in the stool.
In addition, pain is observed in the left side of the abdominal cavity. With inadequate therapy, polyps can turn into cancer.
Features of rehabilitation
After resection, intravenous nutrition is prescribed for the first two days. Then - liquid food. Gradually the patient is transferred to fractional meals (6-8 meals). The food is mainly protein. But preference is given to plant and dairy products.
The diet depends on the magnitude of the impact. But in any case, the digestive tract will have to adapt to a new mode of operation.
Let's take painkillers. After minimally invasive surgery - Diclofenac tablets. After resection, the first two days are given intramuscular narcotics (Droperidol), then Ketorolac. The duration depends on the patient's condition.
To prevent relapses, it is important to minimize the consumption of sweets
Respiratory and therapeutic exercises, early activity, physiotherapy (treatment with currents and heat, laser) are indicated. It is important to maintain suture hygiene to avoid infection and adhesions. The duration of rehabilitation depends on the scale of the operation and the initial condition of the patient.
To prevent relapse, it is recommended to avoid stress and change your diet. It is necessary to exclude rough foods, avoid excess fiber, fatty and fried foods, alcohol, and desserts.
There is no specific prevention. It is important to adhere to a balanced diet and an active healthy lifestyle. Go to the hospital in a timely manner, follow the doctor’s prescriptions, and monitor chronic cardiovascular and gastroenterological pathologies.
With early diagnosis and treatment of the disease, the patient has a greater chance of recovery