Features and types of the disease
Carcinoma is a malignant tumor that is formed from epithelial cells of an atypical structure. The epithelium (the so-called integumentary layer) is a layer of cells that make up the epidermis, as well as mucous membranes that cover the inner surface of various organs. Based on the shape of the cells, several types of epithelium are distinguished (flat, cylindrical, cubic, prismatic and others). Squamous cell carcinoma is a tumor that arises in stratified squamous epithelium. This type of cancer affects the skin and internal organs. In women, this is the name given to a malignant tumor of the cervix.
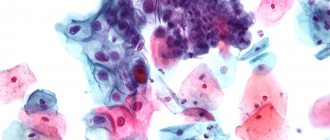
The disease develops gradually. First, a precancerous condition occurs (the so-called stage 0), when cells of an atypical structure (with 2 nuclei, increased in size) appear in the uppermost layer of the epithelium. The tumor then spreads to deeper layers.
Stages of the disease
There are 4 stages of development.
Stage 1. The diameter of the affected area is no more than 4 cm. Cancer cells do not spread beyond the tumor and are not found in the lymph nodes. Treatment of carcinoma at this stage is successful in most cases.
Stage 2. The tumor begins to grow, its size can reach 50 mm. Cancer cells travel to the lymph nodes. In more than half of cases, a cure occurs (the survival rate depends on the location of the cancer and the complexity of treatment).
Stage 3. There is a rapid increase in the size of carcinoma, cancer cells penetrate various organs, and numerous metastases appear. The 5-year survival rate of a patient with this stage of cancer is usually 25%.
Stage 4. Many internal organs, as well as lymph nodes, are damaged, and the person quickly dies.
Video: Stages of cervical carcinoma. Diagnostic methods
Types of tumors
Depending on the external picture that can be observed on the surface affected by the tumor, squamous cell carcinoma is divided into the following types:
- Carcinoma with areas of keratinization. Tumor growth is accompanied by changes in tissue structure. In this case, keratinized areas (“cancerous pearls”) appear. This type of tumor is the easiest to detect and has the best chance of cure.
- Carcinoma without signs of keratinization. The neoplasm does not have clear boundaries; areas of tissue necrosis are observed. This form of the disease is divided into poorly differentiated, moderately differentiated and highly differentiated according to the degree of malignancy. The most favorable prognosis is with a high degree of differentiation.
- Undifferentiated squamous cell tumor. This type of carcinoma is less treatable than all others.
Carcinoma is diagnosed by the absence of “cancer pearls”, the appearance of foci of necrosis, atypical cell division with a violation of the chromosomal composition, and the formation of cells of an uncharacteristic shape with nuclei that differ significantly in size.
Stages of development
Squamous cell carcinoma has four stages of development, excluding stage zero:
- Stage 1 – diagnosis is possible only through instrumental examination, since the cancer does not yet produce symptoms. The tumor can grow into epithelial tissue up to four centimeters.
- Stage 2 of squamous cell carcinoma occurs with germination of the serous layer, but so far only the cervix is affected. There are no metastases, symptoms are also absent or appear to a very slight extent.
- Stage 3 – tissue damage near the uterus occurs. Oncopathology covers not only the tissue of the cervix, but also the pelvic wall or the lower third of the vagina.
- Having reached the fourth stage, the tumor grows into the pelvis, and the tumor also spreads to nearby and distant organs.
We recommend reading Follicular thyroid cancer - causes, treatment, prognosis
The squamous cell carcinoma metastasizes through lymphogenous and hematogenous routes.
Signs of squamous cell carcinoma
When squamous cell cancer of the cervix or other internal organs occurs, symptoms do not appear at an early stage or do not attract much attention. Trouble can be judged by some indirect signs. For example, a person gets tired quickly and experiences weakness. A blood test shows that the hemoglobin level is low, but an indicator such as ESR (erythrocyte sedimentation rate) is significantly higher than normal.
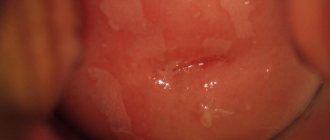
If the cervix is affected by carcinoma, then an unusual slightly yellowish liquid discharge appears (it can be quite abundant) with or without an odor. Sometimes blood appears in them, especially after sexual intercourse or a gynecological examination. In this case, sexual intercourse is painful, and constant aching pain appears in the lower abdomen. In the later stages they are very strong.
Carcinoma located in the pelvic organs puts pressure on neighboring organs, disrupting their function. In this case, frequent or infrequent painful urination may occur, constipation or frequent intestinal disorders may appear. One of the indicative signs of the development of carcinoma is a person’s sudden weight loss and intolerance to certain smells and foods.
Symptoms
At the first stages, symptoms of squamous cell carcinoma of the cervix do not appear, which is associated with late diagnosis if a woman neglects a routine examination with a doctor. When the tumor grows into the deeper layers of the cervix, signs of cancer appear, such as pain, abnormal vaginal discharge and bleeding. Leucorrhoea can be clear, serous or bloody. If the tumor disintegrates or becomes infected, they become cloudy or acquire a purulent character and a foul odor.
The discharge of blood may be spotty or copious. Most often, women experience contact bleeding that occurs after sexual intercourse, therapeutic douching, examination by a gynecologist, or straining when going to the toilet. Because squamous cell carcinoma often develops after menopause, bleeding like menstruation should prompt a woman to see a doctor for evaluation.
Painful sensations can range from mild to very strong, and can be localized in the tailbone, genital area, lower back, and lower abdomen. Pain indicates that the tumor has already grown into the parametrial tissue and affected the nerve plexuses. When cancer pathology spreads to neighboring organs, such as the bladder and intestines, disruption of the functioning of these organs begins, and genitourinary fistulas occur. At the terminal stage, there is a sharp depletion of the body and cancer intoxication.
Causes of carcinoma
Factors that provoke the appearance of squamous cell carcinoma are:
- Hormonal disorders. The cause of their occurrence may be long-term treatment or contraception with hormonal drugs, diseases of the endocrine organs, as well as aging of the body.
- Early onset of sexual activity, frequent changes of partners, and multiple abortions contribute to the occurrence of diseases of the reproductive organs, in particular cervical cancer.
- The presence of infectious, including sexually transmitted diseases, leading to inflammation and scarring of cervical tissue.
- Infection with human papillomavirus (HPV). Most women diagnosed with cervical carcinoma have this virus in their blood. Under its influence, the gene mechanism of cell division is disrupted, resulting in the formation of a cancerous tumor.
- Living in unfavorable environmental conditions, contact with certain chemicals, harmful substances contained in industrial waste, radiation exposure.
- Exposure to ultraviolet radiation is a common cause of skin cancer. Prolonged exposure to direct sunlight or visiting a solarium can trigger the accelerated development of malignant tumors in other organs.
- Addiction to smoking, alcoholism, drug use.
The hereditary factor is of great importance.
Height
In addition to distinguishing squamous cell carcinoma without and with keratinization of the cervix, experts also distinguish the disease by its growth pattern. Since this parameter is well visualized, it is quite simple to determine it, even after the first examination if the development of oncology is suspected. Let's consider how squamous cell carcinoma of the cervix can grow with and without keratinization.
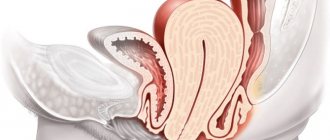
Exophytic growth form. In this case, the tumor formation will always have a pronounced and clear shape, so it is not difficult to determine its size. It grows inward into the lumen of the reproductive organ, but if it is in the uterus, then it grows into its cavity. Detected by ultrasound examination of the pelvic organs.
Oncology can grow into different layers of the organ. Source: pro-rak.ru
Endophytic form. In this situation, atypical cells spread deep into the tissues, that is, they grow inward. Due to this, damage to several layers is noted at once. The tumor does not have defined boundaries, so it may go undiagnosed for a long time, since there is no violation of the shape of the organ.
Mixed form. This type of growth is considered intermediate, between the endophytic and exophytic forms. In this case, the tumor can grow both deeper into nearby layers and into the lumen of the reproductive organ. The boundaries of the neoplasm are blurred, but the possibility of visualization remains.
Diagnosis of carcinoma
Laboratory and instrumental diagnostic methods are used to recognize squamous cell carcinoma.
Blood tests and other studies are performed:
- General. Allows you to determine the hemoglobin content, detect characteristic changes in ESR, leukocyte levels and other indicators.
- Biochemical. The content of proteins, fats, glucose, creatinine and other components is determined. Based on the results obtained, one can judge the state of metabolism, the functioning of the kidneys, liver and other organs, as well as the presence of vitamin deficiency.
- Hormone analysis. It is carried out to confirm the fact that the tumor develops as a result of hormonal imbalance in the body.
- Analysis for the presence of antigens - protein substances, the increased content of which is most often observed with the appearance of squamous cell tumors of the cervix, lung, esophagus and other organs.
- Microscopic analysis of scrapings from the surface of tumors, samples of mucous membranes (smears), and tumor contents (biopsy). For example, squamous cell carcinoma of the cervix is often detected using a PAP test (a test of a smear taken from the cervix).
- Endoscopy of internal organs (bronchoscopy, echoscopy of the uterus, bladder, colonoscopy).
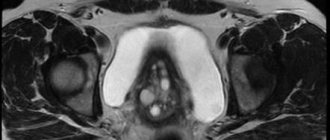
- X-ray of various organs, computed tomography, ultrasound of the pelvic organs, MRI.
Cervical carcinoma
Cervical carcinoma is a malignant disease characterized by damage to the endothelium (flat cells lining the inner surface of blood and lymphatic vessels, heart cavities) and the endometrium (the mucous membrane lining the body of the uterus, which contains blood vessels). During the course of the disease, rapid uncontrolled growth of uterine cells is recorded.
Carcinoma is very common among cancer diseases and is mainly characteristic of women aged 40 to 60 years.
Cervical carcinoma has 2 forms: glandular (pathology of the glandular epithelium or adenocarcinoma) and squamous cell (malignant changes in the squamous epithelium). The squamous cell form is much more common and accounts for 90% of carcinoma cases.
Treatment methods
The main treatment method is surgical removal of the squamous cell tumor. This takes into account its location, the general health of the patient, and age.
When treating superficial tumors, methods such as laser surgery, burning the tumor with an electric current (electrosurgery), and freezing with liquid nitrogen (cryosurgery) are used. Photodynamic therapy (PDT) is also used. A special substance is injected into the carcinoma, which, under the influence of light, kills the tumor within a few minutes.
When deciding on the treatment method for cervical cancer, the doctor takes into account the patient’s age. If a woman is of reproductive age, then at an early stage of the disease only the cervix is removed. The body of the uterus and appendages are preserved. The ovaries are removed in the most extreme cases. In this case, subsequent hormonal therapy is required to maintain normal levels of sex hormones.
Women over 45-50 years old usually undergo a hysterovariectomy (removal of the uterus along with the cervix, appendages and nearby lymph nodes). The operation is performed by laparoscopy or laparotomy.
After removal of the carcinoma, complex treatment with radiation and chemotherapy is prescribed.
Squamous cell carcinoma is a malignant neoplasm of epithelial tissue. Cancer cells can be localized in the lungs, on the cervix in women, in the larynx, on the skin and other places. Characteristic manifestations of the disease are the rapid growth of cancer cells and penetration into nearby tissues due to metastases.
The pathological process can be observed in both sexes, regardless of age.
The disease is diagnosed after a comprehensive examination, including the following procedures:
- radiography;
- CT scan;
- bronchoscopy;
- cytological analysis of sputum or smear;
- colposcopy;
- tissue biopsy and histological examination.
The squamous cell carcinoma antigen SCCA, which is produced in epithelial cells, is very important in the study. Molecular weight is 45–55 kilodaltons. The substance should not leave the cellular space. In cancer, the antigen content increases significantly.
The prognosis depends on the stage of cancer, the patient’s condition, and age. Metastatic cancer leads to death in most cases.
Forms
Therapeutic measures, as well as prognostic data, mainly depend on the form of squamous cell carcinoma. Oncopathology of the cervix of the reproductive organ can occur with or without keratinization.
Using this classification, doctors determine how mature carcinoma cells are:
- In keratinizing squamous cell carcinoma of the cervix, the structure of tumor cell complexes is very similar to the structure of squamous epithelium. Keratinized neoplasms are characterized by slow growth. In the center of the tumor there is an abundant accumulation of keratin, and around there are immature cells that have a round shape. Doctors diagnose this form of squamous cell carcinoma in twenty-five percent of cases.
- Doctors encounter non-keratinizing squamous cell carcinoma of the cervix much more often. Histologically, cellular elements with different structures are determined. They may have differences in kernels and degree of maturity. The non-keratinizing form of cancer is characterized by rapid progression and is more unfavorable in terms of prognosis.
We recommend reading Head cancer - symptoms, first signs, treatment
This disease is also classified according to the degree of invasion of cancer cells:
- During the pre-invasive form of cancer, treatment is very simple, since this type belongs to the zero stage of pathology. The neoplasm is intraepithelial, and according to the classification, it completely coincides with the third degree of cervical neoplasia. There is no risk of metastatic tumors or stromal invasion yet.
- With microinvasive squamous cell carcinoma of the cervix, pathological elements penetrate into the stroma no more than half a centimeter, or even less. The microinvasive form is not aggressive; it progresses to the next type no earlier than two years later. Prognostic data for such squamous cell carcinoma are very high. The risk of metastatic tumors is still very low, and the surrounding organs and lymphatic system function completely normally.
- We can talk about invasive squamous cell carcinoma of the cervix when the penetration of cancer cells into the stroma occurs to a depth of more than three millimeters. At this point, the tumor begins to actively grow, and the lymphatic system stops doing its job. With the invasive form, the risk of metastases and carcinoma spreading beyond the cervix greatly increases.
The degree of differentiation plays a significant role in the matter of prognosis, since oncologists use this classification to indicate the aggressiveness of neoplasm cells:
- Diagnosis of poorly differentiated squamous cell carcinoma of the cervix occurs least often. The prognosis for this form of tumor is unfavorable, the cancer is aggressive, develops quickly, and metastasizes early. Malignant cells are completely different from healthy cells and do not function.
- Well-differentiated squamous cell carcinoma has a good prognosis. The tumor grows very slowly and is not aggressive. The neoplasm cells are as similar as possible to healthy ones and do their job.
- A moderately differentiated type of squamous cell formation occurs most often. The tumor has an average rate of progression, and metastases form at the final stage of cervical cancer pathology. The prognosis varies and depends on the stage at the time of diagnosis.
The degree of invasion can be determined by examination through a colposcope, and differentiation and keratinization are determined by histological examination of the biomaterial after a biopsy.
Etiology
Squamous cell carcinoma is an oncological disease with an aggressive course. The pathological process begins in the skin or mucous layer of the epithelium, spreads to the lymph nodes, neighboring tissues and organs, destroying their anatomical structure and functional activity.
The main causes of cancer:
- radioactive exposure - when working in nuclear production, in the process of abusing diagnostic procedures with x-rays);
- aggressive environmental influences - if a person lives near industrial facilities;
- the presence of viruses (HPV, herpes), erosion and polyps - provoke squamous cell carcinoma of the cervix; women who neglect contraceptives and abuse frequent abortions are at risk;
- hormonal disorders;
- deficiency of immunological functions of the body;
- long-term nicotine addiction;
- pathological processes in the lungs and bronchi caused by pneumoconiosis, chronic bronchitis, pneumonia and tuberculosis;
- taking medications with immunosuppressive effects;
- work in enterprises with increased occupational hazards - in mines, chemical facilities and metallurgy;
- age 1 the risk of getting sick is higher after 50–65 years.
Skin pathological conditions increase the risk of malignant neoplasms.
Prognosis and prevention
The prognosis of squamous cell carcinoma of the cervix primarily depends on the stage at which the pathology was detected. At the zero stage of squamous cell carcinoma (third degree of dysplasia), a favorable prognosis after treatment is observed in one hundred percent of women. The first stage of the disease is successfully cured in ninety out of one hundred patients. When diagnosed in the second stage of development, the five-year survival rate is seventy-five percent. At the third stage, prognostic data drop sharply, and only forty percent of patients can count on recovery.
If squamous cell carcinoma has developed to the terminal (fourth) stage, then only in sixteen percent of cases doctors manage to achieve a complete recovery. If the disease is left to chance and not treated, the patient’s death occurs in less than five years after the discovery of a malignant neoplasm in the cervix. Keratinizing squamous cell carcinoma of the cervix has a more favorable prognosis and is better treatable than a tumor without keratinization.
Prevention of squamous cell neoplasm of the uterine cervix involves an annual visit to the gynecologist.
Timely treatment of precancerous diseases and having one regular sexual partner will help prevent cancer. The onset of sexual activity after the age of seventeen, as well as the prevention of surgical manipulations in the genital tract, reduce the risk of cancer.
Classification
Squamous cell carcinoma has several varieties. The disease has two forms of spread:
According to the degree of cellular differentiation of squamous cell carcinoma, the following are distinguished:
- Keratinizing form. It grows slowly, forms from limited structures and has a greyish-white shiny surface. The structure is differentiated; there are particles with keratinization, which are located on the outside of the tumor, forming a yellowish edging. The most common location is the skin surface. This form of cancer is the most favorable.
- Non-keratinizing form. The presence of a cluster of undifferentiated cell structures is characteristic. The highest percentage of malignancy. The lesion grows quickly and spreads to nearby tissues. The favorite place of localization is mucous tissue; it is very rarely found on the skin.
- Poorly differentiated form. It consists of spindle-shaped cell structures and resembles sarcomatous formations. The degree of malignancy is high - it grows and spreads quickly.
- Glandular form. Localized in the uterus or lung tissues. The structure of the neoplasm contains squamous epithelium and glandular structures. The tumor is growing rapidly, the prognosis is unfavorable.
When invasive carcinoma is diagnosed, the tumor has a high risk of spreading to adjacent tissues and lymph nodes. The prognosis for the non-invasive form of carcinoma is more favorable.
Initial stage of squamous cell skin cancer
The initial manifestations of squamous cell skin cancer have many different variations and depend on the form of cancer, morphology and location.
squamous cell skin cancer: photos of the initial stage
Changes develop on different parts of the body (scalp, facial skin, perianal area, palms, soles of feet).
- plaque form, with a distinctly colored area with rising above the skin
it has tubercles, this area feels dense and rough to the touch.
- nodular form, characterized by a cluster of different-sized nodules, like cauliflower, which are brown in color and dense to the touch. At first, painful cracks appear, nodules gradually form in them, these nodules gradually grow and become denser.
- the ulcerative form of the malignant process is manifested by the development of ulcers of the upper layer of the epidermis, raised above the skin with a smooth depression, the edges are surrounded by a ridge. Such ulcerative defects have a characteristic odor.
Based on the morphostructure, squamous cell keratinizing skin cancer can be distinguished, non-keratinizing, differentiated and undifferentiated.
Squamous cell keratinizing skin cancer occurs from epidermal cell structures that have undergone keratinization. This form of the malignant process is the most benign, as it progresses gradually and slowly infiltrates into the underlying tissues. It is quite difficult to diagnose, since the area of malignant formation is not stained.
The nonkeratinizing form of squamous cell skin cancer is the most malignant process and quickly infiltrates into the lower layers of the skin. With this type of oncological process, mitosis is pronounced, the cells have disintegrating nuclei, and there is no keratinization. The main elements are fleshy granulations of soft consistency.
Although the manifestations of this oncological pathology are varied, the initial manifestations have common features - at first the formation affects only the upper layer of the epidermis, and palpation is painless, then, gradually, the formation grows, thickens, and a plaque appears that rises above the skin.
Symptoms
Squamous cell carcinoma manifests itself in different ways: in addition to the main symptomatic manifestations of cancer, particular features of the location of the pathological process are added.
- fast fatiguability;
- weight loss;
- decreased appetite;
- headache.
With cervical cancer, hemorrhages from the genital tract are possible during sexual intercourse, douching or examination by a gynecologist. With the increase and spread of the cancer process, constipation, the appearance of genitourinary fistulas, and intoxication are noted.
- changes in the skin and mucous membranes - redness, swelling, thickening;
- hemorrhages in organs;
- severe cough or cough with sputum containing blood;
- pain;
- nausea;
- severe itching;
- hoarse voice;
- dizziness.
Cancer develops over time. Stages (stages) of development of malignant formation:
- Zero stage. The primary focus is not detected, there are no metastases in the lymph nodes and organs.
- First stage. The tumor is no more than 5 cm with no metastases.
- Second stage. The size of the neoplasm exceeds 5 cm, the lesion grows into nearby tissues, there are no metastases.
- Third stage. The presence of metastases only in the lymph nodes is typical.
- Fourth stage. The size of the carcinoma varies, and there are metastases in distant organs.
If a person exhibits the above symptoms, they should undergo examination.
Symptoms of squamous cell carcinoma of the cervix
Asymptomatic manifestations of the initial stages of neoplasm development are dangerous. The first symptoms appear when the tumor increases in size and moves to later stages. This disrupts the functioning of the intimate organs. Symptoms noted:
- Painful sensations. The intensity and nature of pain depends on the stage of the cancer process. In the early stages, the pain is not severe and intermittent. As the process progresses to the later stages, the intensity increases and the pain becomes constantly pronounced.
- The appearance of swelling in the legs and genitals. Occurs as a result of the spread of metastases throughout the body through the lymph nodes and circulatory system. As a result of this process, the outflow of fluid from organs affected by cancer worsens. As a result, swelling occurs (the medical term is dissemination).
- Purulent and bloody discharge from the genital area. In this case, the speed and volume of discharge does not matter. They may be accompanied by a pungent odor.
- Chronic fatigue syndrome. The woman does not feel cheerful even after a long period of rest.
- Loss of appetite. The patient forces herself to eat food without feeling hungry.
- Elevated temperature for a long time without the presence of other symptoms of cold-viral pathologies. The temperature is low-grade (within 37.1-38 degrees Celsius). Possible manifestations of low-grade fever (chills).
When the presented symptoms appear, both as individual symptoms and as a combined effect on the body, it makes sense to undergo medical diagnostics in order to make sure that there is no cervical cancer.
Diagnostics
After the patient comes to the clinic, the doctor examines the medical history, listens to complaints, examines the patient and sends him for additional procedures:
- colposcopy;
- X-ray of the lungs;
- CT scan;
- bronchoscopy;
- cytological analysis of smears, sputum;
- tissue biopsy;
- checking the amount of SCC antigen in the blood.
The squamous cell carcinoma antigen SCC is a tumor marker that makes it possible to diagnose cancer in the cervix, nasopharynx, esophagus, lungs, and ear.
The antigen allows a specialist to identify cancer cells, establish the multiple form of the tumor, and the number of foci of metastases in the body. If the concentration is more than 1.5 ng/ml, the patient is diagnosed with cancer in 95%. The SCC level increases significantly during treatment as a result of the breakdown of pathological cells.
Completing a full range of medical diagnostics makes it possible to identify pathology, determine the degree of development of the lesion and select effective therapy.
Some details
One of the most common malignant epithelial tumors is gastric carcinoma, found predominantly among the male population of Japan, Russia, Belarus, and the Baltic countries. Its structure in most cases corresponds to adenocarcinoma - a glandular tumor, which can be papillary, tubular, trabecular, etc. Among the undifferentiated forms, mucous (ring cell carcinoma) can be detected, and such a variety as squamous cell carcinoma in the stomach is extremely rare.
development of carcinomas on the epithelium of the stomach/intestines
Cervical carcinoma also cannot be called a rare pathology. It is diagnosed not only in the elderly, but also in young patients of reproductive age against the background of various precancerous processes (pseudo-erosion, leukoplakia), viral damage or cicatricial deformities. Since most of the cervix is covered with stratified squamous epithelium, the development of squamous cell carcinoma is most likely here, and adenocarcinoma is more common in the cervical canal, which leads into the uterus and is lined with glandular epithelium.
Skin tumors are extremely diverse, but the most common type is considered to be basal cell carcinoma (basal cell carcinoma). This neoplasm affects older people, and its favorite location is the face and neck. Basalioma has a peculiarity: although there are signs of malignancy in the cells and the ability to grow into underlying tissues, it never metastasizes, but grows very slowly and tends to recur or form multiple nodules. This form of cancer can be considered favorable in terms of prognosis, but only if you consult a doctor in a timely manner.
Clear cell carcinoma is the most common malignant tumor of the kidney. Its name suggests that it consists of light cells of various shapes, inside of which fat inclusions are found. This cancer grows quickly, metastasizes early and is prone to necrosis and hemorrhage.
Breast carcinoma comes in a variety of forms, including lobular and ductal varieties, which are “cancer in situ”, that is, non-invasive options. Such tumors begin to grow within the lobule or milk duct and may not make themselves known for a long time and may not show any symptoms.
ductal (left) and lobular (right) breast carcinoma, the difference is in the area of appearance of atypical cancer cells
The moment of development of infiltrating breast carcinoma characterizes the progression of the disease and its transition to the next, more severe stage. Pain and other symptoms are not typical for invasive cancer, and women often discover the tumor themselves (or during a routine mammogram).
A special group of malignant tumors consists of neuroendocrine carcinomas. The cells from which they are formed are scattered throughout the body, and their function is to form hormones and biologically active substances. With tumors of neuroendocrine cells, characteristic symptoms appear, depending on the type of hormone produced by the tumor. Thus, nausea, diarrhea, high blood pressure, hypoglycemia, exhaustion, development of stomach ulcers, etc. are possible. Neuroendocrine carcinomas are extremely diverse in their clinical characteristics.
The World Health Organization has proposed to distinguish:
- Well-differentiated benign neuroendocrine carcinomas;
- Well-differentiated carcinomas with a low degree of malignancy;
- Poorly differentiated tumors with a high degree of malignancy (large cell and small cell neuroendocrine carcinoma).
Carcinoid tumors (neuroendocrine) are more common in the gastrointestinal tract (appendix, stomach, pancreas, small intestine), lungs, and adrenal glands.
Urothelial carcinoma is a transitional cell cancer of the bladder, accounting for more than 90% of malignant neoplasms of this localization. The source of such a tumor is the transitional epithelium of the mucous membrane, which has features similar to multilayered squamous and single-layered glandular epithelium at the same time. Urothelial cancer is accompanied by bleeding, dysuric disorders and is more often detected in older men.
Individual types of carcinomas of different organs are described in more detail in materials devoted to specific types of cancer, so here we have only touched upon their main features.
Metastasis of carcinomas occurs predominantly by the lymphogenous route, which is associated with the good development of the lymphatic network in the mucous membranes and parenchymal organs. First of all, metastases are detected in nearby lymph nodes (regional) in relation to the site of cancer growth. As the tumor progresses and grows into blood vessels, hematogenous seedings appear in the lungs, kidneys, bones, brain, etc. The presence of hematogenous metastases in a malignant epithelial tumor (cancer) always indicates an advanced stage of the disease.
Treatment
Squamous cell carcinoma involves a course of:
- chemotherapy - the use of antitumor drugs;
- radiation therapy - irradiation of the tumor with gamma rays.
In some cases, surgical intervention is prescribed in the initial stages of the disease. Surgeons remove the tumor and metastases, and subsequent chemotherapy or radiation therapy will get rid of the remaining pathological cells.
When the carcinoma is located on the surface and is small in size, electrocoagulation, photodynamic therapy or cryotherapy are used.
After the course of treatment, the patient is registered at the oncology clinic and undertakes to periodically visit the attending physician to monitor the condition.
Prognosis for squamous cell carcinoma depends on the person’s age, stage and location of the carcinoma:
- Cervical cancer of the first stage - 90% survival rate, second - 60%, third - 35%, fourth - 10%.
- Pulmonary malignant tumor. Survival rate in the first stage is up to 40%, in the second - from 15 to 30%, in the third - 10%.
- For skin carcinoma of the first, second and third stages, the survival rate is 60%, the fourth - 40%.
Carcinoma in the early stages is more treatable and the risk of relapse is much lower.
Kinds
Doctors divide this disease into 3 types:
- Exophytic. Defects caused by the disease are observed directly on the surface of the body.
- Endophytic. Defects form deeper in the epidermis rather than on the surface. This variety is more dangerous, because the likelihood of infection penetrating into the bones and glands is greater.
- Mixed. Infection occurs simultaneously on the surface and deeper in the tissues.
Regardless of the form of the disease, the general picture is the presence of cells growing in the deep dermal layers of the skin. Also distinguished:
- Squamous cell keratinizing carcinoma.
- Squamous cell non-keratinizing carcinoma.
The similarity between these two groups is the chaotic arrangement of flat epithelial cells that grow into the deep layers of the skin and into the subcutaneous tissues.
Squamous cell keratinization (highly differentiated) is less painful and is characterized by slow growth and spread. This tumor is most often single and has a flesh-colored, reddish color. The shape of the tumor can be oval or polygonal.
Non-keratinizing squamous cell carcinoma is characterized by a malignant course, grows faster and penetrates into deep tissues, bones and glands. This variety most often has the shape of a nest and is localized in closed areas of the skin. In this case, the tumor has a “fleshy” texture.
Men of retirement age are most susceptible to the disease!
Squamous cell skin cancer is classified into stages using the TNM classification depending on the degree of tumor penetration deep into the skin, tumor involvement of lymph nodes and the presence of distant metastases.
Based on their histological structure, the following types are distinguished:
- non-keratinizing cancer - constantly dividing cells without signs of keratinization;
- keratinizing cancer – there are areas of keratinization in the tumor layer;
- glandular squamous cell carcinoma – develops from the skin glands (sebaceous, sweat);
- Spindle cell carcinoma – The cells in this type of skin cancer resemble a spindle.
There are special types of squamous cell carcinoma:
- Bowen's disease is a small erythematous plaque or spot, often with scales on its surface. The tumor does not penetrate into the deep layers of the skin, but remains on the surface, involving the hair follicles and skin glands in the process.
- Scar carcinoma occurs on the surface of the scar as nodules, an area of chronic inflammation, or an ulcer.
- Verrucous carcinoma resembles a common wart and is localized primarily on the plantar part of the foot.
Possible complications
A large number of cancer patients die due to the late stage of detection of the cancer process. The diagnosis can cause the following complications:
- hemorrhage;
- peritonitis;
- pulmonary edema;
- respiratory and heart failure;
- metastases;
- depletion of the immune system;
- disruptions in the functioning of internal organs and intoxication.
For a healthy person, the best way to protect against cancer is to follow these rules:
- maintaining a healthy lifestyle - without taking alcohol, drugs and nicotine;
- good working conditions (in case of harmful emissions, appropriate protection must be used: special suits and masks with filters);
- life away from industrial facilities;
- physical activity and healthy food.
It is worth treating diseases that can provoke the appearance of a malignant tumor in a timely manner.
Squamous cell carcinoma, or squamous cell carcinoma, is a histological type of malignant tumor, such a diagnosis is made by the results of a biopsy after examining a sample of tumor tissue under a microscope. The neoplasm is formed from flat epidermal cells that look like scales. It can occur on the skin, in the oral cavity, in the larynx, trachea, bronchi, esophagus, genitals, and rectum.
At the European Oncology Clinic, the diagnosis and treatment of squamous cell carcinoma is carried out by expert doctors who have extensive experience working in leading oncology centers in Moscow. A team that includes oncologists, dermato-oncologists, surgeons, chemotherapists, radiotherapists and other specialists works with the patient. We use innovative treatment methods, the latest generation of drugs, and conduct antitumor therapy in accordance with leading international recommendations. The European Oncology Clinic is the first Russian private oncology center where you can receive effective palliative treatment in late stages, even in cases where the patient was abandoned in other clinics.
Clinical manifestations
There are two forms of growth of squamous cell carcinoma: exophytic and endophytic. Each of them is characterized by certain clinical manifestations.
Exophytic (papillary) form
The primary nodule in this type of tumor gradually increases in size and rises above the skin level. A large amount of horny mass accumulates on the surface of the lesion. Over time, its color becomes red or brownish with a large number of dilated vessels on the surface (telangiectasia). Sometimes retraction is detected in the center of formation.
The base of the neoplasm is wide. The lesion itself and the surrounding tissues are inactive due to tumor growth. In later stages, necrosis and ulceration occur.
A type of exophytic squamous cell skin cancer is its verrucous form, which is characterized by a yellow or red-brown color of the lesion, an uneven surface with warty growths. This type of tumor, in turn, also has several clinical variants depending on the location:
- Oral papillomatosis - neoplasms on the mucous membrane of the tongue, cheeks, and gums. Usually seen in people who chew tobacco.
- Anogenital carcinoma. It is located on the skin of the glans penis, scrotum, vulva, and perianal area.
- The plantar type is typical for older men.
- Squamous cell verrucous cancer of other areas of the skin (extremities, torso).
The verrucous form is characterized by slow growth and a low risk of metastasis. On the skin, this type of cancer forms most often in places that are subject to constant mechanical stress and may have the appearance of a cutaneous horn.
Book a consultation 24 hours a day
+7 (495) 151-14-53
Endophytic (ulcerative-infiltrative) form
With endophytic tumor growth, the primary element is a nodule, which over time turns into a dense node. The lesion is closely fused with the underlying tissues. After a few months, it ulcerates. The ulcer has an irregular shape, a dense bottom, a whitish film on the surface and crater-shaped edges. It may be covered with a brownish crust, which, when removed, releases a bloody exudate. The ulcer increases in depth and to the sides, quickly spreading to the underlying tissue. This form of squamous cell skin cancer is characterized by frequent recurrence and the formation of metastases.
Causes of squamous cell carcinoma
The causes of squamous cell carcinoma are the same as for other types of malignant tumors. Certain mutations occur in cells that lead to malignant degeneration. “Incorrect” cells lose the external features and functions of normal ones, begin to multiply uncontrollably, and acquire the ability to spread throughout the body.
The main risk factors for squamous cell carcinoma:
- On the skin, such tumors often arise due to the action of ultraviolet rays. Exposed areas of the body are the most vulnerable.
- Squamous cell carcinoma of the genitals, head and neck is caused by certain types of human papillomavirus.
- The risk of developing squamous cell carcinoma is increased in smokers and people who drink a lot of alcohol.
- The likelihood of developing cancer increases with age as mutations accumulate in the cells of the body.
- Scars, burns, chronic inflammation.
- Exposure to certain carcinogenic substances, for example, if a person works in an industrial environment and comes into contact with chemicals.
- Decreased immunity.
None of these factors is guaranteed to lead to the disease - each of them only increases the likelihood to a certain extent.
Squamous cell carcinoma - general characteristics, definition and mechanism of development
To understand the essence of squamous cell carcinoma, and also to imagine why this type of tumor grows very quickly and can affect any organ, you should know the meaning of the words “squamous cell” and “cancer” by scientists and practicing doctors. So, let's look at the main characteristics of squamous cell carcinoma and the concepts necessary to describe these characteristics.
Firstly, you should know that cancer is a rapidly growing tumor made up of degenerated cells that have been able to quickly and constantly divide, that is, multiply. It is this constant, uncontrolled and unstoppable division that ensures the rapid and continuous growth of a malignant tumor.
That is, the degenerated cells grow and multiply constantly, as a result of which they first form a compact tumor, which at a certain moment ceases to have enough space in the area of its localization, and then it simply begins to “grow” through the tissue, affecting everything in its path - blood vessels, neighboring organs, lymph nodes, etc.
The cells of a malignant tumor are constantly dividing, as a result of which new elements are continuously formed along its periphery, compressing normal cells of an organ or tissue, which simply die as a result of such aggressive influence. The space vacated by dead cells is quickly occupied by a tumor, since it grows incomparably faster than any normal tissue in the human body. As a result, normal cells in tissues and organs are gradually replaced by degenerated ones, and the malignant tumor itself grows in size.
At a certain point, individual cancer cells begin to detach from the tumor, which first enter the lymph nodes, forming the first metastases in them. After some time, with the flow of lymph, tumor cells spread throughout the body and enter other organs, where they also give rise to metastases. In the final stages, cancer cells that give rise to metastatic growth in various organs can spread through the bloodstream.
The key moment in the development of any malignant tumors is the moment of formation of the first cancer cell, which will give rise to the uncontrolled growth of the tumor. This cancer cell is also called degenerated, since it loses the properties of normal cellular structures and acquires a number of new ones, allowing it to give rise to and maintain the growth and existence of a malignant tumor.
Such a degenerated cancer cell always has an ancestor - some normal cellular structure, which, under the influence of various factors, has acquired the ability to divide uncontrollably. In relation to squamous cell carcinoma, any epithelial cell plays the role of such a tumor progenitor.
That is, a degenerated cell appears in the epithelium, which gives rise to a cancerous tumor. And since this cell looks flat in a microscope, a cancer tumor consisting of cellular structures of the same shape is called squamous cell carcinoma. Thus, the term “squamous cell carcinoma” means that this tumor developed from degenerated epithelial cells.
Since epithelium is very widespread in the human body, squamous cell tumors can form in almost any organ. Thus, there are two main types of epithelium - keratinizing and non-keratinizing. Non-keratinizing epithelium is all the mucous membranes of the human body (nose, oral cavity, throat, esophagus, stomach, intestines, vagina, vaginal part of the cervix, bronchi, etc.).
The keratinizing epithelium is a collection of skin coverings. Accordingly, squamous cell carcinoma can form on any mucous membrane or skin. In addition, in more rare cases, squamous cell carcinoma can form in other organs from cells that have undergone metaplasia, that is, turning first into epithelial-like cells and then into cancer.
Thus, it is obvious that the term “squamous cell carcinoma” most closely refers to the histological characteristics of a malignant tumor. Of course, determining the histological type of cancer is very important, since it helps to select the optimal treatment option taking into account the properties of the detected tumor.
Moreover, the most common is skin cancer, which develops in 90% of cases in open areas of the skin, such as the face, neck, hands, etc.
However, squamous cell carcinoma can also develop in other organs and tissues, such as the vulva, lips, lungs, colon, etc.
What are the types of squamous cell carcinoma?
Malignant neoplasms of this histological type are found on different parts of the body. Depending on the location, their properties, approaches to diagnosis and treatment, and prognosis for the patient may differ slightly.
Skin cancer
Malignant skin tumors are represented by squamous cell carcinoma in approximately 20% of cases. Much more often, patients suffer from basal cell carcinoma, which originates from cells located in the lower layer of the epidermis.
Squamous cell carcinoma is more aggressive than basal cell carcinoma. It is more likely to grow into the deeper layers of the skin and spread throughout the body with the formation of distant metastases. However, this happens quite rarely. Most often, the tumor can be detected and removed at an early stage.
As a rule, squamous cell carcinoma occurs on the skin of the face, ears, neck, back of the hands, and less commonly in the genital area. Often, a neoplasm develops where scars and chronic injuries are located.
Squamous cell carcinoma of the red border of the lips
Malignant lip tumors account for no more than 1–3% of all cancers. In most cases (95%) they are represented by squamous cell carcinoma, which comes in two types:
- Squamous cell keratinizing carcinoma does not behave as aggressively, grows slowly, and rarely forms distant metastases.
- Nonkeratinizing squamous cell carcinoma grows rapidly, ulcerates earlier, and metastasizes more often.
Research shows that this type of cancer is 3 to 13 times more common in men than in women. This is probably due to the fact that males are more often exposed to sunlight at work, and smoking and drinking alcohol are more common among them.
Oral cancer
Oral cancer is a malignant tumor that occurs on the mucous membrane of the lips, cheeks, gums, the anterior two-thirds of the tongue, the palate, and the floor of the mouth (located under the tongue). In 90% of cases they are represented by squamous cell carcinoma, of which 5% are keratinizing squamous cell carcinoma, which is less aggressive, less likely to grow into surrounding tissues, spread to lymph nodes and metastasize.
Esophageal carcinoma
The mucous membrane of the esophagus is lined with stratified squamous epithelium, and squamous cell carcinoma can develop from it. Most often, such tumors are located in the cervical esophagus and the upper two-thirds of the thoracic region. In the lower third of the organ, adenocarcinomas, malignant tumors of glandular cells, are more common.
Laryngeal cancer
In laryngeal cancer, the tumor almost always develops from squamous epithelium and is a squamous cell carcinoma. Typically, the appearance of a tumor is preceded by precancerous changes - dysplasia. The cells that are located in the lesion do not look like normal ones, but they also differ from cancer cells. In some cases, dysplasia does not lead to the development of cancer and even goes away on its own, especially if its cause is eliminated, for example, a person quits smoking. But in some people, precancerous changes lead to “cancer in situ” and then an invasive tumor.
Trachea and bronchus cancer
Squamous cell carcinoma is the most common type of malignant tumor in the trachea. It usually occurs in the lower part of the trachea, grows quite quickly, invades its wall, leading to ulceration and bleeding. This is a rare type of cancer and its main cause is smoking.
Reasons for the development of pathology
The main reason for the development of squamous cell skin cancer is considered to be genetic predisposition. It can be hereditary or acquired and is expressed in:
- Damage to cellular DNA under the influence of certain factors, resulting in a mutation of the “TP53” gene, which encodes the “p53” protein. The latter, as a regulator of the cell cycle, prevents tumor transformation of cells. "TP53" is one of the main genes involved in blocking the development of malignant tumors.
- Disorder of the functions of the immune system directed against tumor formations (antitumor immunity). Many cellular mutations constantly occur in the human body, which are recognized and destroyed by cells of the immune system - macrophages, T- and B-lymphocytes, natural killer cells. Certain genes are also responsible for the formation and functioning of these cells, mutations in which reduce the effectiveness of antitumor immunity and can be inherited.
- Disorders of carcinogenic metabolism. Its essence lies in the mutation of genes that regulate the intensity of the function of certain systems, which are aimed at neutralizing, destroying and quickly removing carcinogenic substances from the body.
Favorable background for the development of squamous cell skin cancer are:
- Age. The disease is extremely rare among children and young people. The percentage of cases increases sharply among people over 40 years of age, and after 65 years of age this pathology occurs quite often.
- Skin type. People with blue eyes, red and blond hair, and fair skin that is difficult to tan are more susceptible to the disease.
- Male gender. Among men, squamous cell carcinoma develops almost 2 times more often than in women.
- Skin defects. Cancer can also develop on clinically healthy skin, but much more often - against the background of freckles, telangiectasia and genital warts, precancerous diseases (Bowen's disease, Paget's disease, xeroderma pigmentosum), in the area of scars formed as a result of burns and radiation therapy, after which cancer can occur even after 30 or more years, post-traumatic scars, trophic changes in the skin (with varicose veins), openings of fistulous tracts with osteomyelitis of the bone (the frequency of metastasis is 20%), psoriasis, lichen planus, lesions with tuberculous and systemic lupus erythematosus, etc. d.
- Long-term decrease in general immunity.
Among the provoking factors, the main ones are:
- Ultraviolet radiation with intense, frequent and prolonged exposure - sunbathing, PUVA therapy with psoralen, carried out for the treatment of psoriasis and also desensitization for allergies to sunlight. UV rays cause a mutation in the TP53 gene and weaken the body's antitumor immunity.
- Ionizing and electromagnetic types of radiation.
- Prolonged exposure to high temperatures, burns, prolonged mechanical irritation and damage to the skin, precancerous dermatological diseases.
- Local exposure over a long period of time (due to the specifics of professional activity) of carcinogenic substances - aromatic hydrocarbons, soot, coal tar, paraffin, insecticides, mineral oils.
- General therapy with glucocorticoid drugs and immunosuppressants, local therapy with arsenic, mercury, chlormethyl.
- HIV and human papillomavirus infection types 16, 18, 31, 33, 35, 45.
- Irrational and unbalanced nutrition, chronic nicotine and alcohol intoxication of the body.
The prognosis without treatment is unfavorable - the incidence of metastases is on average 16%. In 85% of them, metastasis occurs in regional lymph nodes and in 15% - in the skeletal system and internal organs, most often in the lungs, which always ends in death. The greatest danger is from tumors of the head and facial skin (70% affected), especially squamous cell carcinoma of the skin of the nose (dorsum of the nose) and neoplasms localized in the forehead, nasolabial folds, periorbital areas, in the area of the external auditory canal, red border of the lips, especially the upper one, on the auricle and behind it. Tumors that arise in closed areas of the body, especially in the area of the external genitalia, of both women and men, are also highly aggressive in terms of metastasis.
Types of disease diagnosis
The oncologist prescribes certain types of diagnostics to the patient, depending on which organ the malignant tumor is located in:
Location of cancer
Skin, red border of lips- Examination by a dermatologist.
- Dermatoscopy.
- The European Oncology Clinic uses a modern dermoscopic device – PhotoFinder. It allows you to create a “mole map” and identify the smallest changes on the skin.
- Examination by an ENT doctor.
- Pharyngoscopy.
- Laryngoscopy.
- Bronchoscopy.
- Esophagoscopy.
- HPV testing.
- Endoscopic examination, including endosonography.
- X-ray with contrast enhancement.
- CT, MRI.
- Chest X-ray.
- Bronchoscopy.
- Examination by a gynecologist
- Examination by a gynecologist.
- Colposcopy.
- Examination by a proctologist.
- Proctoscopy.
- Colonoscopy.
- Fecal occult blood test.
In all cases where a pathological formation is detected, a biopsy is performed - a study during which a fragment of suspicious tissue is obtained and sent to the laboratory for histological and cytological examination. Biopsy is the most accurate method for diagnosing cancer. It helps not only to reliably establish a diagnosis, but also to determine the histological type of the tumor. In order to check the extent of cancer spread in the body and clarify the stage, the doctor may prescribe additional tests:
- computed tomography, MRI;
- X-ray of the chest, bones;
- PET scan;
- Ultrasound and endoscopic examination of organs into which cancer could have grown.
Diagnostic methods
To determine the presence of a malignant process in the body, it is necessary to take urine and blood tests.
It is important to conduct a timely examination to accurately determine the diagnosis, since squamous cell skin cancer is confused with benign formations on the skin of the face. Therefore, first the patient takes a blood and urine test. This allows us to detect the development of cancer in the body. To study tissue, a biopsy is performed. A more thorough examination is carried out using magnetic resonance imaging (MRI) and ultrasound (ultrasound).
Treatment of squamous cell carcinoma
Treatment depends on the location, stage of cancer, the general condition of the patient, the presence of concomitant diseases and other factors.
Radiation therapy
Ionizing radiation damages tumor and other rapidly multiplying cells. This type of treatment for squamous cell carcinoma can be prescribed before or after surgery, or in advanced stages for palliative purposes.
Surgery
Radical operations are possible if there are no metastases and the cancer has not grown strongly into surrounding tissues. In some cases, only surgical treatment is indicated for such patients, in others it is supplemented with antitumor drugs and radiation therapy - this helps reduce the risk of relapse.
For advanced squamous cell carcinoma, palliative surgery can be performed to eliminate symptoms and restore the patency and function of the affected organ.
Drug treatment of squamous cell carcinoma
Chemotherapy for squamous cell carcinoma can be adjuvant (after surgery), neoadjuvant (before surgery), or used as a stand-alone treatment in advanced stages.
If the tumor has certain molecular genetic characteristics, targeted therapy is prescribed. Targeted drugs target molecules that help cancer grow and maintain its vital functions.
Symptomatic treatment for squamous cell carcinoma
Treatment for squamous cell carcinoma and any other malignant neoplasms should be aimed not only at fighting the tumor itself, but also at relieving symptoms and improving the patient’s condition. At the European Oncology Clinic, the patient can receive all types of symptomatic therapy for cancer:
- Relief of pain syndrome in accordance with the WHO three-step scheme.
- Restoration of patency of the esophagus, intestines, and respiratory tract.
- Elimination of bleeding, if necessary, blood transfusion.
- Relief of nausea.
- Removing tumor compression of internal organs, nerves, and blood vessels.
- Treatment of emergency conditions in an intensive care unit equipped with modern equipment.
- Monitoring and correction of nutritional status.
- Maintenance therapy helps you comfortably endure chemotherapy and prevent and manage side effects.
Diagnosis and treatment of skin cancer
To eliminate squamous cell skin cancer, a complex of treatment procedures is used. The main impact that doctors have on the patient is surgical intervention. As a result of this procedure, the tumor is removed and the patient is rehabilitated.
Treatment methods can vary significantly depending on the characteristics of the patient: his condition, age, stage of the disease. Often, small tumors can be removed using radiation therapy or local chemotherapy.
If the tumor has affected the skin on the face, then photodynamic therapy is used. The patient is injected intravenously with a substance that spreads throughout the body. As soon as the drug reaches the infected areas, the tumor is exposed to special light radiation.
If the patient has distant metastases, the prognosis can worsen sharply.
With skin cancer, it is difficult to make a prognosis for the patient's life expectancy. Scientific literature states that everything depends on a person’s physical condition, his genetic predispositions, treatment methods and many other factors.
To detect cancer early, it is recommended to take some preventive actions. It is necessary to constantly monitor the skin of the body and if neoplasms appear, immediately contact a dermatologist. The use of ointments with 5-fluorouracil reduces the likelihood of skin cancer and also improves the appearance of the skin.
When treating squamous cell skin cancer, an integrated approach is used, which can combine several methods of therapy, the main of which is surgery. After surgery, which involves removing the tumor within healthy tissue, high-precision radiation therapy IMRT and electron therapy are used.
In some cases, patients are indicated for chemotherapy and/or targeted therapy. The choice of treatment for squamous cell skin cancer depends on the stage, location, extent of the process, the presence of metastases, age and general condition of the patient.
Electrocoagulation, curettage, and cryodestruction are more often used for small and multiple tumors, but the latter is not used when the tumor is located on the scalp. Treatment for squamous cell skin cancer is divided into several main options.
This can be: surgical treatment (including the Mohs method), radiation therapy, cryodestruction and photodynamic therapy.
Treatment for squamous cell skin cancer is carried out by an oncologist. Depending on the stage of the process and the growth characteristics of the tumor, one of the tumor treatment options is selected:
- Surgical removal of the formation is the leading method of treating the disease. The method is used when a tumor is detected on the skin of the torso or limbs. The formation is removed, including 1-2 cm of healthy tissue. Lymph nodes are removed if changes are detected in them.
- Cryogenic removal - destruction of the tumor using liquid nitrogen. It is performed to treat small tumors within the upper layers of the skin. The method allows you to remove the tumor while minimally affecting healthy tissue.
- Radiation therapy is the exposure of the tumor site to ionizing radiation. The method is effective especially in combination with cryogenic exposure, which increases the sensitivity of tumor cells to radiation exposure, or surgical removal of the tumor.
- Photodynamic therapy is based on the ability of a tumor to accumulate certain substances that initiate cell destruction under the influence of laser radiation. The method is relatively new, but one can already note its effectiveness and the possibility of using it to detect distant foci of tumor growth.
- Drug treatment is becoming increasingly important due to the spread of tumors that are resistant to radiation. Chemotherapy is used in combination with surgical methods for certain indications: the spread of the process to the lymph nodes and internal organs, resistance to radiation exposure, and others. Bleomycin, cisplatin, and 5-fluorouracil are used as antitumor drugs.
With a common process, a combination of several treatment methods is used: for example, surgical removal, radiation and chemotherapy.
— Examination by an oncologist, dermato-oncologist. During the examination, the presence of a neoplasm is revealed, its consistency, color, condition of the skin around it, the presence of formations in other localizations, examination and palpation examination of the lymph nodes. Anamnesis collection.
— Instrumental methods are used to clarify the presence of an oncological process, the degree of invasion into the underlying layers, the presence of metastatic changes in nearby lymph nodes, and the presence of distant metastases.
The following instrumental methods are used: confocal scanning microscopy (the ability to evaluate all layers of the epidermis), ultrasound of the OB (clarifies the presence of metastatic changes), MRI (determines the presence of a tumor, its shape, composition, the presence of metastases), X-ray and endoscopic methods (the presence of an oncological process of another localization, presence of distant metastases).
At the present stage, one of the best methods for visual inspection of the elements of the altered dermis is dermatoscopy or skin surface microscopy. This non-invasive technique allows, with different magnifications, to examine the morphological and subepidermal structures of the dermis. An optical device with a lens and illumination is used - a dermatoscope and immersion oil, which makes it possible to examine intradermal structures from 0.2 microns.
— Laboratory diagnostic methods: standard tests, identification of tumor markers, cytological examination allows you to determine the size, structure, shape, composition of tumor cells, biopsy is an opportunity to fully assess the type of tumor process, its cellular structure, and the degree of the oncological process. Biopsy is the “gold standard” for diagnosing cancer.
Based on the data obtained, subsequent therapeutic tactics are determined.
- surgical method;
- radiation therapy;
— cryodestruction;
- chemotherapy;
- symptomatic therapy.
Surgical treatment of squamous cell skin cancer is one of the most common and most effective methods of treating this pathology. It consists of surgical excision of the formation and nearby tissues at a distance of 2 cm. During the operation, a microscopic assessment of the tumor is carried out, which allows surgical treatment to be carried out as effectively as possible. If necessary, the affected muscles, bones, and organs are removed. If metastases are detected in the lymph nodes, the lymph nodes are removed.
In the surgery of squamous cell skin cancer, the main role is played by the Mohs method - this is micrographic surgery, which was created by Frederick Mohs. This technique provides layer-by-layer microscopic analysis of tissue during surgery and makes it possible to perform excision in the required volume. This method is expensive in terms of time, money, and personnel, but it is the most “thorough” method of excision of the formation.
If the defect is small in size (up to 2 cm) and is located in the upper layers of the epidermis, then to remove it it is permissible to use electrocoagulation in the area of unchanged tissue up to 10 mm, and cryodestruction involving healthy tissue up to 2.5 cm.
Radiation therapy is common, but not as effective as surgery. It is used as monotherapy when surgical treatment is not possible. More often it is combined with surgical removal of the tumor. Used as preparation for surgical treatment to limit the malignant process.
Chemotherapy is an additional treatment option. More often used in preparation for surgical removal, it reduces the tumor in size and slows down its growth. Also, if the tumor is inoperable, then chemotherapy is used in conjunction with radiation therapy. Basic drugs used: bleomycin, 5-fluorouracil, cisplatin.
Symptomatic therapy is aimed at improving the quality of life and correcting side effects caused by radiation or chemotherapy. Painkillers are used, including the use of narcotic analgesics, hemostatic drugs, enteral or parenteral nutrition to compensate for the lack of proteins, fats, carbohydrates, and the use of drugs for the treatment of concomitant pathologies.
The choice of treatment method is influenced by:
- Histological structure of the tumor.
- Its localization.
- The stage of the cancer process, taking into account the presence of metastases and their prevalence.
Surgical excision
A small tumor without metastases is surgically excised within the unaffected tissue, 1-2 cm away from its edges. If the operation is performed correctly, the cure rate over 5 years is on average 98%. Particularly good results are observed when the tumor is excised en bloc with subcutaneous tissue and fascia.
Radiation therapy
- A surgical operation during which the primary lesion and lymph nodes affected by metastases are removed;
- Radiotherapy (radiation therapy);
- Chemotherapy.
Survival prognosis for squamous cell carcinoma
The prognosis depends on where the cancer began to grow, at what stage the diagnosis was made and treatment started. For example, often the survival rate for cancer of the skin and red border of the lips tends to 100%, because such tumors, as a rule, can be detected early enough, and they are not very aggressive. If distant metastases appear, the chances of remission become extremely low. But such patients can still be helped: to slow down the progression of squamous cell carcinoma, prolong life, improve their general condition, and relieve painful symptoms.
How to cure squamous cell skin cancer?
After an accurate diagnosis, treatment is prescribed. And to determine the method of treatment, it is necessary to take into account factors such as the presence and number of metastases, the location of the tumor, the stage of development of the disease, as well as belonging to a specific age group and general health indicators of the patient.
Today there are several of the most effective ways to treat squamous cell carcinoma:
- cryodestruction;
- surgery;
- X-ray therapy;
- chemotherapy;
- laser cancer removal;
- use of photodynamic therapy.
Simultaneously with the above methods of cancer treatment, restorative procedures should be used that increase the patient’s immunity level and improve his overall health.
Surgery
This method of treatment assumes that the patient is in satisfactory condition and can undergo surgery. This method is used in the presence of large lesions of the skin, as well as in the last stages of cancer development.
Cryodestruction
This method, in combination with electrocoagulation, is used for numerous foci of infection, as well as relapses of the disease and for minor skin infections.
Chemotherapy
This method of treating the appearance of squamous cell formation is also one of the most effective combined. Used for extensive skin lesions and relapses. Chemotherapy makes it possible to preserve the most healthy surface of the body near the area of infection; the effect is directly on the tumor.
X-ray therapy
This method of exposure is used for cancer lesions of the face (the area around the lips, eyelids, mouth and nose). Also, an indication for the use of this method is the advanced age of the patient.
Prevention
Basic measures to prevent squamous cell carcinoma:
- Quitting smoking and drinking alcohol.
- Protecting your skin from ultraviolet rays is the most important measure for preventing skin cancer. You should not visit solariums or go to the beach from 10.00 to 16.00, when solar activity is highest. Clothes with long sleeves and trousers, a wide-brimmed hat, and sunglasses help protect yourself.
- Preventing infection with HPV, which leads to the development of cancer: you need to avoid promiscuity and use condoms. There is currently a vaccine against human papillomavirus infection. It is recommended that all adolescents be vaccinated before becoming sexually active.
Stages of progression
Squamous cell carcinoma in the uterus has the following stages of development:
- Initial. Atypical cells spread predominantly on the surface of the epithelium without growing into the underlying tissue. It is divided into the following periods: minimally invasive;
- invasive squamous cell carcinoma.
Main signs of the disease
Symptoms of carcinoma depend on many different factors: the location of the tumor, the presence of metastases, as well as the growth rate of the tumor and the severity of the disease.
The main signs characteristic of the manifestation of cancer can be described as follows:
- modification of the skin in a localized area in the form of an ever-increasing swelling with a rim of pronounced hyperemia of the skin;
- difficulty swallowing;
- voice change;
- dry spasmodic cough;
- difficulty passing food through the esophagus;
- pain in the abdomen or chest;
- a sharp decrease in appetite;
- severe weight loss;
- general weakness of the body not motivated by anything.
Other symptoms include increased body temperature, unpleasant taste and smell in the mouth, breast hardening, bloody discharge from the nipple, difficulty urinating, and bloody discharge from the bladder.
The clinical picture of the disease becomes most striking after the tumor has metastasized.
Causes and risk factors
Squamous cell carcinoma of the cervix is a malignant tumor that develops from the cells of the stratified squamous epithelium that covers the vaginal part of the cervix. This pathology is one of the most common malignant neoplasms among women aged 40–60 years.
Despite the general decrease in the structure of cancer incidence, the number of patients with the initial stages of this pathology has increased significantly, especially among women aged 30–40 years. The main role in provoking the disease is played by human papillomaviruses, of which subtypes 16 and 18 are considered to be oncogenic, and, much less frequently, subtypes 31 and 33.
Clinical diagnosis
Each cancer disease is characterized by the difficulty of diagnosis in the early stages. Thus, lung cancer is difficult to determine in the first two stages: manifestations that a person already has may indicate both pneumonia and tuberculosis, and in 15% of cases they are completely asymptomatic. The intensity of symptoms depends on the size of the tumor, its location and histological structure.
First of all, the patient’s medical history and complaints are collected, and a physical examination is performed. Objective instrumental diagnostic methods can help in detecting a tumor:
- radiography is the most common diagnostic method in pulmonology; it determines the shape and size of the tumor, the condition of the lymph nodes;
- computed tomography – analyzes the malignant formation layer by layer, which makes it possible to clarify its structure and nature;
- Bronchoscopy is necessary to examine the epithelium and mucous membrane of the airways and the extent of their damage, helps to find out whether the tumor is spreading;
- A blood test for tumor markers is a study of the composition of the blood to determine the presence of specific proteins that are produced by atypical cells. It can be used to determine the type of lung cancer.
- Cytological analysis of sputum and bronchoalveolar lavage also helps determine the type of cancer cells;
- Biopsy (histological examination): carried out in cases where there are difficulties in establishing a diagnosis. For study, a particle is removed from the tumor and nearby lymph nodes.
To make an accurate diagnosis and determine a treatment strategy, a set of diagnostic measures is prescribed.
Types of disease
In oncology, the following types of squamous cell carcinoma are distinguished:
- Plaque cancer, characterized by the formation of red plaques that have bleeding bumps on the surface. This type of cancer is characterized by rapid growth, damage to the surface of the skin, and the spread of metastases into the inner layer of the skin.
- Nodular cancer is caused by the formation of red nodes, which in appearance resemble cauliflower. Their surface is lumpy and their structure is dense.
- Ulcerative cancer, which is characterized by the appearance of ulcers on the skin with raised edges. These ulcers have an unpleasant odor and bleed constantly. They tend to penetrate inside the body, affecting tissues that are nearby.
Symptoms of pathology
In most cases, the symptoms that appear during the spread and development of the tumor process are similar to the symptoms of other chronic lung pathologies.
The main profile symptoms include:
- Cough of dry and wet nature.
- Shortness of breath (in the first stages appears after physical activity, over time it begins to occur at rest).
- Intense pain in the chest (often occurs in the form of cutting pain, especially severe when coughing).
The symptoms listed above in their initial manifestations may occur as a result of a common cold. Only those symptoms that progress over time and depend on the size of the tumor in the lung tissue can be differentiated from a tumor.
Other symptoms of pathology are not directly related to the respiratory system, but occur during the development of almost any oncological process. These include:
- Human chronic fatigue syndrome - with this pathology, work efficiency remains at a low level, the person feels tired even after a long rest.
- Loss of appetite – a person ceases to have interest in food, and the body becomes exhausted.
- Apathy is the inability to experience desires.
These symptoms are difficult to interpret when they appear alone in the patient's history. If these symptoms appear together, you must immediately seek diagnostic procedures and an examination by an oncologist.
As the size of the tumor increases, the symptomatic manifestations become more intense and intense. Hemoptysis occurs, and pain in the patient’s chest intensifies. With the development of the geography of distribution of secondary foci, the development of accompanying pathological processes occurs. Symptoms depend on which organ is affected by the secondary source of pathology. A characteristic symptom in this case is pain in the affected organ. From the moment the secondary lesion appears, the newly formed tumor invades the damaged organ, which causes pain.
Metastases that have spread from the original tumor are often found in the following organs and tissues:
- heart muscle;
- kidneys;
- bone structures;
- stomach;
- liver.
Multiple organ failure gradually develops. When secondary lesions enter the brain, the functionality of the central nervous system is inhibited. Confusion of consciousness to the point of loss, loss of spatial coordination is possible. A person develops a depressive state, regular mood swings, irritability, and aggressiveness. Memory functions are impaired.
Consequences of the disease
Oncological diseases, if promptly sought help from specialists, respond well to treatment and have a high chance of full recovery.
But in advanced stages, even after professional treatment, oncology is quite dangerous and entails unpleasant and serious consequences, which include:
- anatomical inferiority;
- disability;
- disturbances in the functioning of the immune system;
- dysfunction of the organ affected by the disease;
- infertility;
- psychological trauma;
- physical and emotional exhaustion of the entire human body.
In the initial stages, after cessation of treatment, patient survival is quite high. In the last stages of the disease, a stable remission usually occurs, during which the cancer enters the chronic stage, sometimes causing relapses that require prolongation of therapy. No one can predict when and how this will happen. In some cases, they even talk about spontaneous remission, when the tumor disappears on its own, without any treatment. But even with long-term remission, patients live a normal life, but once every six months they have to visit an oncologist and take tests to detect cancer cells.
Types of Lung Cancer
- Squamous cell nonkeratinizing lung cancer has all the classic signs of this pathology and is diagnosed by fluorographic examination. A darkened area will be visible in the photo. Differential diagnosis with esophageal cancer is necessary.
- Poorly differentiated lung cancer is characterized by rapid migration of pathological cells to other tissues of the body. The difficulty of detecting it lies in the fact that abnormal cells resemble healthy ones in structure. In most cases, it is diagnosed when metastases reach the organs of the digestive system, liver, kidneys, and brain. The right lung is affected more often than the left.
- Squamous cell keratinizing lung cancer (otherwise known as moderately differentiated squamous cell lung cancer) has a slow development. Squamous cell carcinoma of the bronchi and lung of this type is characterized by the formation of so-called cancer pearls. Malignant cells collect in reddish nodules, covered with scales, in the center of which keratinization is observed. If detected early, the prognosis is most favorable.
- Glandular-squamous type. Combines features of glandular tissue carcinoma and squamous cell lung cancer. Small peripheral bronchi are affected. It grows quickly and metastasizes to other organs. It is more typical for women.
- The disseminated form is characterized by multiple small foci of cancer cells located throughout the organ.
- Mediastinal form , in which metastases primarily affect the nearest lymph nodes.
Diagnosis of the pathological process and stage
When symptoms first appear, you should immediately consult a doctor for a diagnostic test. During the diagnostic process, the form of pathology, localization, and stage will be established.
The stage of the oncological process has a direct impact on the patient’s life prognosis. It is customary to distinguish 4 stages of cancer. There is also a precancerous stage, which is characterized by metaplasia of the lung tissue. In this condition, it is too early to talk about malignancy, but the presence of this pathology indicates a high risk of cancer in the near future.
The criteria for determining the stages of the oncology development process are given in the table:
| Stage No. | Characteristic |
| Stage 1 | The diameter of the tumor is less than 3 centimeters, has a clear localization within one lobe of the lung and there are no metastases. |
| Stage 2 | High probability of primary metastases in regional lymph nodes. The lobe of the lung cannot perform its functionality to the same extent. Respiratory function begins to become depressed. The diameter of the formation does not exceed 6 centimeters. |
| Stage 3 | The third stage is characterized by a tumor size of 6 to 8 centimeters in diameter. The increased danger lies in the active spread of metastases throughout the body. Vital organs begin to be damaged, which leads to the appearance of concomitant pathologies and deterioration in organ function. |
| Stage 4 | The scientific name is thermal stage. The size of the tumor is more than 8 centimeters. But the primary tumor poses the least danger compared to metastases. The whole body is affected. |
Depending on the stage, the chance of survival of patients decreases. The gradation of dependence is established in the table below:
| Stage | Survival percentage |
| Stage 1 | Survival rate 80 percent |
| Stage 2 | Survival rate 50 percent |
| Stage 3 | Survival rate 20 percent |
| Stage 4 | Survival rate 2 percent |
At stage 4, patients live no more than 2 years.
Survival requires detection of pathology at an early stage. Methods for diagnosing lung cancer include the following procedures:
- Fluorography is the study of pathology using x-rays.
- Bronchoscopy is a visual examination of the bronchi using an endoscope.
- Magnetic resonance imaging (MRI) is used to determine the presence of metastases.
- CT scan.
- PET method.
- Ultrasound of the chest organs.
- Biopsy.
- Analyzes of biomaterials of blood, urine and feces.
After conducting a set of diagnostic studies, the doctor prescribes treatment in accordance with the data obtained from clinical studies.
Course of the disease
The course and development of cancer can be divided into several stages:
- zero or initial stage, which is characterized by the absence of a primary tumor and metastasis;
- first stage - characterized by the presence of a tumor up to five centimeters in size and the absence of metastases;
- second stage – there are still no metastases, the tumor increases in size and can grow into nearby organs;
- third stage – characterized by the presence of metastases in the lymph nodes and a primary tumor of any size;
- the fourth or last stage, which is characterized by the presence of metastases in other internal organs, while metastasis in the lymph nodes may be absent, and the tumor itself can be of any size and grow into neighboring tissues.
The early stage of the disease usually goes unnoticed. It is characterized by modification and uncontrolled cell division, their gradual transformation into cancer cells. The chance of cure in the early stages of the disease is usually ninety to one hundred percent.
As the disease progresses, the patient's chances of recovery decrease significantly. Severe stages of oncology are characterized by a predominance of metastases in the lymph nodes and other organs, tumor growth into nearby tissues and organs. Cancer at the last stage is almost impossible to cure. In such cases, a successful operation to destroy the primary tumor does not provide any guarantees to the patient, since distant metastases will gradually burn the person drop by drop.
Even the third stage of such a disease already has scanty chances of success. The life expectancy of a patient with stage 3 carcinoma depends entirely on the degree of damage caused by the tumor.
With stage IV cancer, even after removal of the primary malignant tumor, the patient’s death occurs in almost one hundred percent of cases. They die in the last stages of cancer within a few years.
Survival
In many countries, mortality from cancer, in particular from lung cancer, ranks first. This disease mainly affects the male part of the population, but recently there has been a tendency towards an increase in mortality from lung cancer among women.
This is due to environmental degradation, consumption of low-quality food, as well as an increase in the number of smokers, which has a detrimental effect on the health of both men and women.
How long do patients with lung cancer live?
The survival prognosis for patients with squamous cell lung cancer is disappointing, since the development of a malignant tumor is almost always accompanied by the appearance of metastases. On average, given overall rates, the survival rate among 15% of the population is only about 5 years.
As a result of recent studies, a prognosis can be made taking into account the stages of the disease, since everything depends on many external factors and the individual characteristics of the patient himself.
Survival:
- at stage 1 cancer - 60-80% per 100 people;
- at stage 2 cancer - 40-50% per 100 people;
- at stage 3 cancer - 20-25% per 100 people;
- at stage 4 cancer - less than 10% per 100 people.
The fight for health and, often, life depends on time, because early diagnosis allows you to fight the disease, and therefore preserve the main asset of a person - his life.
Source: rak.hvatit-bolet.ru
Types of disease
Squamous cell carcinoma is divided into types according to the work of malignant epithelial cells (depending on their differentiation), tumor growth and location of formation.
Differentiation
This type of cancer can be differentiated or undifferentiated. The two types of cancer are called keratinizing and non-keratinizing cancer NOS (not otherwise specified).
- An undifferentiated type of squamous cell carcinoma occurs without the accumulation of keratin in malignant cells, so horny tissue does not form and the cells do not die. Because of this, the tumor spreads quickly and aggressively. A pathology is formed (the spinous layer of the epithelium is affected, a tumor develops), capturing other layers and organs - invasive cancer develops without keratinization.
- Differentiated squamous cell carcinoma progresses more slowly as dying cells accumulate keratin and die, forming keratinizing fragments. The process goes faster than normal keratinization.
- There is a poorly differentiated type of squamous cell carcinoma, consisting of spindle cells and similar to the formation of sarcoma. This is the most aggressive form of cancer, since the cells are as far apart in structure as possible from healthy cells. If a highly differentiated cancer is diagnosed, the disease progresses more slowly, and the cells partially retain their previous structure.
Squamous cell skin cancer
Sometimes the degree of differentiation of the disease is determined. Using special designations, five degrees of cancer differentiation are distinguished:
- Gx is a disease state where differentiation cannot be distinguished.
- G1 – well-differentiated cancer.
- G2 – moderately differentiated tumor (medium differentiation tumor).
- G3 – low-grade oncological process.
- G4 is an undifferentiated type of cancer.
Tumor growth
Malignant neoplasms develop and grow in different ways. Squamous cell malignant keratinizing tumors form in the epithelium, so any organ that has this tissue can become the primary site of disease in this type of cancer. The disease can follow three scenarios: a tumor type of cancer, an ulcerative infiltrate, or a mixed form that combines the qualities of a tumor and ulcers in the epithelium is formed.
- Exophytic cancer involves the formation of a tumor. Initially, a dense node forms in the epithelium, possibly with keratinization. As it grows, it elongates in height rather than spreading in width. Immobile, penetrates deep under the epithelial layer. Covered with scales, but as the disease progresses, it becomes covered with ulcers.
- Endophytic cancer immediately begins with a node covered with ulcers. Soon secondary, daughter nodes are formed around, gradually merging with the main one. This is how the disease invades new epithelial spaces.
- The mixed form involves keratinization of the skin, the development of ulcers, and tumor formation as parallel processes.
Localization
Based on the place of formation, cancer is divided into many subtypes. Most common:
- malignant neoplasm of the skin;
- lip border cancer;
- neoplasms in the oral cavity, esophagus and larynx - upper gastrointestinal tract;
- malignant process of the trachea and bronchi - upper respiratory tract;
- squamous cell carcinoma of the cervix.
The location of cancer formation determines the symptoms of the disease and affects the speed and methods of diagnosing the formation.
Endometrial cancer of the uterus - symptoms and signs
When endometrial cancer develops, symptoms of the pathology appear after a long time. Most patients do not complain at the time of detection of the tumor. This explains the frequent accidental diagnosis of the disease during the search for the causes of disorders of the reproductive system. The main symptom indicating cancer is uterine bleeding.
These discharges have no connection with menstrual discharge. They are not abundant and are often accompanied by slight pain, which misleads patients. Women themselves mistake the symptoms for extraordinary periods and consult a doctor only when they recur several times. Carrying out differential diagnosis helps to establish the true cause of bleeding - endometrial cancer.
As the pathology progresses, the symptoms also increase. Among other signs of a disease such as endometrial cancer, it is necessary to highlight:
- The appearance of leucorrhoea
is a pathological discharge from the genital tract. Occurs when a tumor grows. The accumulation of such secretions in the uterine cavity causes painful sensations in the lower abdomen of a pulling nature. - Purulent vaginal discharge.
Violation of the outflow of leucorrhoea can cause infection and provoke the formation of pyometra - an accumulation of pus in the uterine cavity. At the same time, the woman notes the appearance of bursting pain, an increase in body temperature, and a deterioration in general well-being. - Pain syndrome
- appears when the pathological process spreads, infiltrative changes in the pelvic cavity. With the rapid growth of the tumor, compression of the ureter occurs, and pain appears in the lumbar region. - Disturbance in the process of urination and defecation.
Large sizes of the primary tumor provoke the appearance of additional symptoms (pain during urination, defecation, tenesmus - a false, painful urge to defecate). - Irregularities in the menstrual cycle
– lengthening, shortening, increasing the volume of menstrual blood. Often associated with hormonal changes in the patient’s body.
Endometrial cancer - stages
Depending on the clinical manifestations and degree of impairment, the following stages of uterine endometrial cancer are distinguished, according to the classification of the International Federation of Obstetricians and Gynecologists (FIGO):
1. Stage zero (0) – atypical endometrial hyperplasia is observed, which is the initial stage of oncology.
2. The first stage – the tumor does not extend beyond the body of the uterus (IA-C). It is customary to distinguish:
- Stage IA – the tumor does not grow inwards and is limited to the epithelial layer;
- Stage IV – the muscle layer is involved in the pathological process, but does not reach its middle;
- Stage ІС – carcinoma grows half of the muscular layer and deeper, but does not reach the serous membrane.
2. The second stage is divided into:
- IIA – exclusively glands are involved;
- Stage II – the stroma is affected.
3. Third stage - endometrial cancer leaves the boundaries of the organ, but does not go beyond the pelvis. Depending on the clinical features, this stage is divided into:
- IIIA – carcinoma invades the serous membrane or affects the appendages;
- IIIC – characterized by the appearance of metastases in nearby lymph nodes.
4. Fourth stage:
- the tumor grows into the bladder or rectum - IVA.
- the appearance of distant metastases outside the pelvis – IVB.
Carcinoma and its varieties
Carcinoma is a malignant neoplasm that affects cells of the mucous membranes, skin and internal organs. All malignant tumors are formed according to the same principle. The layers of epithelium covering the internal organs and skin are constantly renewed, that is, continuous cell division occurs. Any, even the most minor, failure in this process can lead to mutation at the genetic level. Next, a new growth may arise from the mutated cells, growing dynamically, occupying all available space and affecting healthy tissue.
At the next stage, the mutated epithelium spreads through the blood and lymph to other internal organs and the formation of new tumor foci there, largely distant from the primary source - metastasis.
A malignant tumor grows much faster than a benign one and can significantly increase in volume in a short time.
Carcinoma is considered one of the most common cancers. And the criteria for its danger directly depend on the type of tumor, stage of development and a number of other reasons.
Carcinoma is classified depending on which structural cellular elements it developed from. When cells in contact with the external environment mutate, squamous or cellular carcinoma occurs - a tumor that consists of multilayered epithelium. In turn, squamous cell carcinoma can be keratinizing, in which the affected cells die, forming a characteristic yellow crust on the surface of the tumor, and non-keratinizing.
Non-keratinizing cancer, or carcinoma without keratinization, is an accumulation of undifferentiated tissue, which leads to rapid tumor development, aggressive course of the disease and active metastasis. This form of cancer is considered the most malignant of all squamous cell oncologies.
Carcinoma that developed from the epithelial layers of glandular tissues (breast, salivary, bronchial glands, prostate) was called adenocarcinoma or glandular cancer.
There is also transitional cell carcinoma, a tumor that develops from transitional epithelial cells.
The tumor classification according to the degree of differentiation is as follows:
- highly differentiated (G1);
- moderately differentiated (G2);
- low-grade (G3);
- undifferentiated (G4);
The most dangerous of them are undifferentiated formations, since it is almost impossible to identify whether a tumor belongs to any tissue. They have a high degree of malignancy, in other words, this means that such formations have the ability to quickly form metastases.
These include trabecular type cancer, most often called solid cancer and is a form of undifferentiated carcinoma with pronounced cell atypia.
Glandular squamous cell oncology develops on those organs that, in addition to the mucous membrane, also have a glandular network. This tumor most often affects the uterine or pulmonary tissues of the body, progresses rapidly and rarely has a favorable prognosis.
There are also invasive and intraepithelial forms of cancer. Invasive cancer is distinguished from other types by the active and rapid growth of a tumor that affects neighboring organs, tissues and lymph nodes. With the intraepithelial variety, the lesion is localized in one of the organs without affecting other tissues.
Based on their structure, the following types of cancer are distinguished:
- medullary carcinoma, which is characterized by a predominance of cancer cells in the tumor - parenchyma;
- fibrous carcinoma, in which connective tissue cells predominate - stroma;
- simple carcinoma, where stroma and parenchyma are in extremely equal proportions.
Squamous carcinoma is a type of squamous cell carcinoma, which is characterized by the development of a tumor process in the upper layers of the epithelium, caused by prolonged exposure to direct sunlight or in a solarium. That is, in most cases, such cancer is formed due to excessive exposure of skin cells to ultraviolet radiation.
There are other types of carcinomas:
- odontogenic – developing from the epithelium that forms tooth enamel;
- verrucous - developing from epithelial cells of the upper epidermis;
- mucoepidermoid - developing from the epithelial cells of the excretory ducts of the salivary glands;
- mucinous – primary carcinoma of the sweat glands.
The above classification does not cover all possible types of carcinomas. Many of them are divided into several types, depending on the characteristic features, location of the tumor, degree of malignancy and other indicators.
Oncology treatment
Depending on the size of the cancer tumor, its location, and the age of the patient, individual treatment for squamous cell skin cancer is developed. The important point here is to remove the affected tissue as early as possible.
Note! Timely treatment increases the patient's chances of survival.
Often the cancerous tumor is removed surgically. During the operation, the surgeon removes the primary tumor, as well as lymph nodes if metastases are detected in them. After removal of the tumor, X-ray therapy is used. It can also be used when a tumor is located in any part of the face, as well as when treating elderly people if surgery is contraindicated for them. During the operation, not only the tumor is removed, but also all the structures into which it has grown. In some cases, it may be necessary to amputate a limb or remove an internal organ that has been affected.
In addition to surgery, the doctor may prescribe cryodestruction, in which the tumor is frozen with liquid nitrogen by spraying it with special equipment. This method is used for small tumors; it does not leave scars after the procedure. But this technique is never used when the scalp is affected.
After surgery, cancer treatment usually involves the use of chemotherapy to eliminate the remaining cancer cells. This treatment method is quite effective; in 99% of cases the disease has a favorable prognosis.
If there is a large tumor, a course of radiation therapy is first given to reduce its size. After this, the patient undergoes chemotherapy. Most often, these two treatments are sufficient to cure the patient. Radiation therapy is used in the presence of cancerous tumors of any location. In most cases, this method treats the disease in the initial stages of development. In the case of late-stage squamous cell carcinoma, radiation therapy is used before surgery, after which the tumor is completely removed. Treatment of highly differentiated cancer requires a long period of time and fairly high doses of radiation. If a relapse develops, this treatment method is not used again.
During all medical procedures, symptomatic treatment is carried out, the purpose of which is to reduce pain, stop bleeding, eliminate infections, and treat concomitant pathologies.
What is squamous cell carcinoma and how is it different from others?
The process of human breathing is simpler than it might seem at first glance:
- a person takes a breath - the intercostal muscles and diaphragm relax;
- through the trachea, through the bronchi, through the bronchioles, air enters the alveoli;
- the alveoli are covered with a thin network of capillaries and through their thin walls oxygen enters the blood, and carbon dioxide enters them from the blood;
- carbon dioxide leaves the alveoli through the bronchioles, bronchi and trachea;
- The intercostal muscles and diaphragm tense - the person exhales.
In the process, dust, dirt, pathogenic microorganisms enter the lungs along with the air, despite all the cleaning that it undergoes in the upper respiratory tract, and settle on the mucous membrane. Immediately, the cilia located on the ciliated epithelium lining the lungs from the inside begin to move. Together with a small amount of mucus, they push everything unnecessary into the trachea, from there into the pharynx - phlegm comes out.
But:
- if carcinogens, that is, poisons, get inside, the eyelashes begin to die;
- where they have died, the ciliated epithelium is replaced by squamous epithelium, which is characteristic of completely different organs - for example, the esophagus and larynx;
- The flat epithelium can do nothing to interfere with foreign elements - they settle on it without hindrance.
Stagnant mucus plus carcinogens, plus dust and dirt - all this forms an ideal environment for the development of pathological processes . Squamous cell lung cancer is one of them.
Classification by tumor location
Localization is the place of primary formation of the oncological process of tumor appearance. Based on location, the following types are distinguished:
| Name | Localization |
| Central cancer | The main large bronchi become the site of damage. |
| Peripheral cancer | Occurs in the area of the alveoli and small bronchi. |
| Mediastinal cancer | It is characterized by damage to the lymph nodes at the beginning of the oncological process (detects the most unfavorable prognosis in terms of survival). |
| Disseminated cancer | With this type of cancer, the formation of several small foci that are not connected with each other at the initial stage of cancer development occurs. It can form simultaneously in the cavity of the right and left lungs. |
| Massive cancer | The oncological process damages the large and small bronchi of the patient. |
Lung sarcoma
Main types of lung cancer
The diagnosis of squamous cell lung cancer combines several types of malignant lesions - distinguished by the form of the course, symptoms, and treatment tactics.
Depending on the structures of the respiratory system in which the tumor has formed, experts distinguish the following types of cancer:
- With the localization of the focus in the main or intermediate part of the bronchi - the central form of the oncological process. It is detected in 2/3 of patients during differential diagnosis with a prolonged course of pneumonia. Symptoms are most often blurred and implicit.
- With the formation of a tumor process in the segmental region of the bronchi or in their lobes - a peripheral variant of cancer. Concomitant diseases make timely diagnosis difficult. A characteristic clinical picture will be visible already at the stage of metastasis.
- Depending on the variant of the atypical process in the cells, it is also customary to distinguish squamous cell keratinizing or small cell cancer of the pulmonary structures.
The prognosis and treatment will be determined individually by a specialist, based on the above classification.
Factors predisposing to cancer development
If the ciliated epithelium is replaced by flat epithelium, this is not at all a guarantee that a person will develop a malignant tumor - everyone knows examples of smokers who lived to a very old age.
But the chance becomes much higher. The probability increases:
- Smoking. Most people suffering from squamous cell lung cancer are smokers or relatives of smokers . Over the years of active or passive smoking, the ciliated epithelium is burned out by the tars and toxic compounds contained in tobacco smoke.
- Heredity. If three people in your family have died from squamous cell lung cancer, this significantly increases the risk of its development in the patient.
- Ecology. Tars and poisons contained in the atmosphere in disadvantaged regions have no less impact on the lungs than constant smoking of tobacco.
- Work in hazardous production. Even if you never put a cigarette in your mouth and live in an ecologically clean area, working in a factory, working with dust, gases and paints can have an impact on the likelihood of squamous cell lung cancer.
- Chronic lung diseases and tuberculosis . They also lead to the death of the ciliated epithelium, which means they increase the likelihood of developing the disease.
It is interesting to note that the right lung is more often affected than the left. This is due to the fact that its bronchus is located at a smaller angle to the trachea and, accordingly, more dirt gets inside, as well as more smoke when smoking.
Complications and metastases
At advanced stages of uterine cancer pathology, there is a high probability of developing the following complications:
- genitourinary system - due to pressure from the formation on the ureter, the system does not function fully, urine stagnates, congestion forms in the organ, which threatens purulent infection;
- liver - the organ is not able to process too high a concentration of toxins, which leads to its partial dysfunction;
- kidneys – accompanied by fistulas of internal canals against the background of actively occurring metastasis of the organ;
- damage to the lymphatic system, first of nearby nodes, then of the whole body.
Stages of the disease
| Stage | Substage | Description and size |
| 0 Stage | Precancerous or preinvasive form | Squamous cell carcinoma of the cervix affects only the epithelial layer. |
| Stage 1 | Primary | The body of the uterus is not affected. Primary germination into nearby tissues occurs. |
| 1A | The tumor can only be detected with a biopsy due to its small size. | |
| 1A1 | The horizontal lesion is at least 7 mm. The depth of the lesion is up to 3 mm. | |
| 1A2 | The lesion is 7-8 mm horizontally and 3 mm deep. | |
| 1B | The depth of the lesion reaches 5 mm | |
| 1B1 | The tumor reaches a size of 4 cm | |
| 1B2 | The tumor is larger than 4 cm. | |
| Stage 2 | Cancer affects the walls of the uterus. | |
| 2A | Involves the pelvic walls. | |
| 2B | Affects parametric tissue. | |
| Stage 3 | It compresses the ureteral canal and affects most of the vaginal walls. | |
| 3A | The lesion goes deep into the vagina. | |
| 3B | Hydronephrotic kidney failure. | |
| Stage 4 | The malignancy grows into the walls of the bladder, grows into the walls of the intestines and can affect the ovaries. | |
| 4A | Tumor growth into neighboring organs. | |
| 4B | Metastases through the lymphatic or circulatory system reach distant organs: lungs, liver, brain, abdominal cavity, mammary gland. |
There are four stages of uterine cancer:
- The first is that cancer is found only in the uterus.
- The second is that the cancer has spread not only to the uterus, but also to the cervix.
- Third, the cancer has affected the walls of the pelvis and part of the vagina from below.
- The fourth is the most dangerous and advanced stage. Cancer has already affected the organs that are nearby. Metastases went to the rectum or bladder. Cancer can affect the bone marrow and lungs.
In squamous cell carcinoma, changes occur at the DNA level in squamous epithelial cells. Human papilloma virus, inflammatory processes in the uterus, erosion, and the presence of contraceptive devices contribute to the degeneration of human papilloma cells. This effect on the epithelium leads to its traumatization. As a result, the DNA structure is disrupted, and immature cancer cells are born, which do not perform the function of squamous epithelium, but simply multiply, become keratinized, and subsequently the entire cervix does not perform its function, and this process is called carcinoma.
Carcinoma develops in the uterine epithelium layer. Like all diseases, squamous cell carcinoma has its own stages:
- Poorly differentiated;
- Differentiated;
- Poorly differentiated.
Squamous cell keratinized cervical cancer produces a lot of keratin and cancerous pearls in the very center of the tumor, this can be seen under a microscope. This type of cancer has large nuclei and eosinophilic cytoplasm. In the tumor stroma, inflammatory infiltration and multinucleated cells are visible.
Squamous cell non-keratinized cervical cancer (poorly differentiated) is the most common neoplasm. It has oval cell nuclei, poorly distinguishable cytoplasm, a large number of mitoses, unclear boundaries, visible areas of tumor tissue decay, different sizes of nuclei, and no cancer pearls.
To determine the stage and severity of the pathological process of squamous cell carcinoma of any location, the TNM classification is used, in which each letter denotes one of the characteristics of the tumor. In this classification, the letter T is used to indicate the size of the tumor and the extent of its spread to surrounding tissue.
The letter N is used to indicate the extent of lymph node metastasis. And the letter M reflects the presence of metastases to distant organs. For each tumor, its size, the presence of metastases in lymph nodes and other organs are determined, and all this information is recorded in the form of an alphanumeric code.
The numbers and letters of the TNM classification mean the following:
- Tx – no data on the tumor;
- T0 – no primary tumor;
- Тis – cancer in situ;
- T1 – tumor less than 2 cm;
- T2 – tumor from 2 to 5 cm;
- T3 – tumor more than 5 cm;
- T4 – the tumor has grown into neighboring tissues;
- N0 – lymph nodes are not affected by metastases;
- N1 – lymph nodes affected by metastases;
- M0 – no metastases to other organs;
- M1 – there are metastases to other organs.
Stage 0 – Т0N0М0;
Stage I – T1N0M0 or T2N0M0;
Stage II – T3N0M0 or T4N0M0;
Stage III – T1N1M0, T2N1M0, T3N1M0, T4N1M0 or T1-4N2M0;
Stage IV – T1-4N1-2M1.