Cervical cancer is a malignant neoplasm caused by human papillomavirus serotypes 16, 18, 33 and 35. In the Russian Federation, new cases of the disease are detected in 16.2 cases per 100 thousand population per year. The mortality rate from this type of tumor is 10.1 per 100,000 people per year. The organization of cytological screening allowed oncologists at the Yusupov Hospital to significantly reduce the morbidity and mortality from in situ cervical cancer.
The oncology clinic has created all the conditions for the treatment of patients diagnosed with cervical cancer and carcinoma in situ:
- Chambers of European comfort level;
- Use of the latest diagnostic procedures, which are performed using equipment from leading global manufacturers;
- Compliance with Russian recommendations and protocols ASCO, NCCN;
- An individual approach to the choice of treatment method for each patient, depending on age, the presence of concomitant pathology and the sensitivity of the tumor to treatment methods.
Severe cases of cervical cancer are discussed at a meeting of the Expert Council, in which professors and doctors of the highest category take part. Leading specialists in the field of oncology of the female reproductive system collectively develop patient management tactics. The medical staff is attentive to the wishes of patients and their relatives.
Causes
Among cancers in young women, cervical cancer has the highest mortality rates. This disease can be completely cured if detected in the early stages. Screening for cervical carcinoma in situ includes a Pap test (Papanicolaou test), which shows changes in the cervix and helps rule out the presence of human papillomavirus.
Most often, women aged 40–55 years are susceptible to cervical cancer. The following factors may influence the development of cervical cancer in situ:
- Early onset of sexual activity;
- Smoking;
- Sexually transmitted infections;
- Weakened immune system;
- Failure to maintain intimate hygiene;
- Chronic inflammatory processes of the cervix;
- The presence of dysplasia and erosion of the cervix, leukoplakia.
Identifying and eliminating risk factors for cervical development helps prevent the disease. Scientists have identified several features of the development of cervical cancer. Cancer in situ does not have blood vessels, which limits the growth of the tumor. Abnormal cells appear at the same rate as they die. For this reason, the size of the tumor does not increase. Cancer in situ affects the stratified squamous epithelium of the vaginal part of the cervix.
Causes
It is still impossible to say exactly why pathology occurs. It is believed that changes in individual genes (mutations) cause dysfunction of cells. Sometimes mutations occur naturally when DNA is replicated during cell division. There are environmental factors that can damage DNA and increase the likelihood of in situ cancer:
- substances contained in tobacco smoke
- ionizing radiation
- ultra-violet rays.
There are also chemicals that are considered carcinogens that provoke the development of tumors. It is not necessary that cancer will occur after contact with the substance; it depends on the time of exposure and the individual characteristics of the person. For example, the following are considered dangerous:
- arsenic
- asbestos
- benzene
- benzidine
- beryllium
- coal tar and soot
- crystalline silica
- ethylene oxide
- formaldehyde.
Symptoms
Carcinoma in situ of the cervix is asymptomatic. Cancer cells are detected during a cytological examination of a scraping from the cervix, which is performed during a routine examination. In the future, the following symptoms may occur:
- Leucorrhoea and spotting outside of menstruation, uterine bleeding;
- Pain in the lower abdomen, lower back, sacrum or when urinating;
- Feeling of heaviness in the pelvic area;
- Discomfort during intercourse, bleeding after coitus.
As the disease progresses, swelling of the lower extremities, external genitalia, disruption of the bladder and intestines, and urinary retention appear. If the lymph nodes are affected, swelling of the lower limb on one side may develop. General signs of a tumor process develop in the body: weight loss, dizziness, general weakness, decreased appetite, increased body temperature.
Stages of ductal carcinoma in situ
An international scale is used for tracking and evaluation, which determines how quickly cancer cells grow in relation to healthy ones. Depending on the stage of non-invasive ductal carcinoma, doctors can predict whether the breast cancer will return after treatment or whether it will progress to a more malignant process.
Types of cancer cells of non-invasive ductal carcinoma
When examining atypical cells under a microscope, they can be of different structures and have varying degrees of aggressiveness in comparison with healthy tissues, often turning into infiltrating ductal carcinoma.
Diagnostics
The method for early diagnosis of cervical carcinoma in situ is the Pap test. If the study shows minimal changes in CIN1, the woman is observed by gynecologists. Most often, this condition goes away without treatment. If the Pap test indicator is CIN2 or CIN3. Further diagnostics are being carried out.
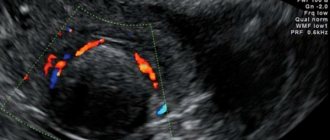
Also, cancer in situ of the cervix can be detected during a gynecological examination. If the gynecologist notices specific changes in the cervix, a biopsy is taken from the patient and a histological examination is performed. When histologists confirm the presence of cancer cells, the patient undergoes further diagnostics. To begin with, doctors at the oncology clinic determine the extent of cancer spread, for which they conduct an ultrasound examination and magnetic resonance imaging of the pelvic area. If there is a suspicion of metastasis of the disease, according to the collegial decision of oncologists, the patient undergoes a whole body computed tomography scan or PET-CT scan. At the Yusupov Hospital, these studies are performed using the latest generation equipment.
In order to timely establish the diagnosis of cervical carcinoma in situ and carry out timely treatment that improves the prognosis, gynecological oncologists use the following diagnostic algorithm:
- Standardized collection of cellular material from the cervix;
- Application of liquid-based cytology;
- Immunocytochemical study of the P16INK4α tumor marker.
In the absence of visible pathology, a scraping must be taken from the cervix for cytological examination. Material is collected from the entire surface of the cervix and from the cervical canal. Due to the fact that cancer most often develops at the junction of the squamous epithelium of the cervix with the columnar epithelium of the cervical canal, along the perimeter of the uterine pharynx, scraping for collecting material necessarily includes this area and the epithelium of the cervical canal. Of fundamental importance in this case is the use by doctors of the Yusupov Hospital of a special instrument, which guarantees the collection of material from all specified areas and ensures the information content of the drug. Oncologists at the clinic do not use adapted tools and means, since this leads to a decrease in the effectiveness of screening, up to zero results.
Morphologists at the Yusupov Hospital use a new technology for preparing cytological preparations, the so-called liquid cytology. An important technological feature of the method, which improves the quality of the study, is that the material being studied is taken into a special stabilizing solution. It ensures its safety without destruction and loss of cells. At the same time, the cellular material retains its immunocytochemical and morphological properties.
Immunocytochemical determination of p16 expression on smears prepared using liquid cytology allows one to reliably assess the potential of dysplasia in relation to the development of cervical cancer and choose more conservative or more aggressive treatment tactics, clarify the cytologist’s conclusions, and in many cases, reasonably refuse a biopsy.
Cancer in situ of the colon
Obligate intestinal precancer, that is, very often leading to the development of carcinoma in the rectum or transverse colon, is polyps. Not all polypous growths are capable of becoming a malignant tumor, but often in long-standing and “to the eye” completely benign formations of the mucous membrane more than 3 centimeters in size, tiny foci of intraepithelial neoplasia, usually adenocarcinoma in situ, are found. Therefore, such polypous growths must be identified and removed; small polyps of a certain cellular structure can be observed for a long time, if a biopsy does not reveal cancer foci “in situ,” but if they enlarge, they must be operated on; it turns out that the operation is simply postponed.
Treatment
Cervical carcinoma in situ is considered the earliest form of cancer, but doctors sometimes consider this tumor as a precancerous condition. This is due to the fact that atypical cells in in situ cancer are found only in the superficial layer of the cervix and do not spread to deep tissues.
Treatment for cervical carcinoma in situ is similar to other precancerous conditions. Oncologists at the Yusupov Hospital use cryosurgery, laser surgery, cryoconization and loop electroexcision procedures. Hysterectomy is usually performed for adenocarcinoma in situ. Conization of the cervix is carried out in those women who are planning a pregnancy. The patient is closely monitored, and the excised tissue sample should have “clean” edges. Hysterectomy is performed on patients who are no longer planning a pregnancy. One treatment option for in situ cervical cancer is a conventional hysterectomy.
Precancerous changes may reappear in the vagina or cervix, which is why medical supervision is so important. It includes regular vaginal examination with smears for oncocytology and, in some cases, colposcopy. The choice of treatment tactics largely depends on the individual characteristics of the woman’s body and on the diagnostic results.
If a woman is diagnosed with cervical in situ cancer, the prognosis is good with adequate timely treatment. For this reason, women should regularly visit a gynecologist and undergo a comprehensive examination of the whole body. If there are risk factors, they must be eliminated. Lifestyle is no less important. The risk of developing cervical carcinoma is reduced in women who have a relationship with a regular sexual partner, use barrier methods of contraception, play sports and do not have bad habits. In order to make an appointment with an oncologist-gynecologist, call the contact center of the Yusupov Hospital at any time convenient for you.
Author
Natalya Aleksandrovna Vyaznikova
Oncologist
Non-invasive tumor stage
The stage of a non-invasive tumor, when the tumor process, with preserved integrity of the basement membrane, is limited only to the epithelial layer, within which the cells have all the signs of cataplasia characteristic of cancer, is called “cancer in situ” - carcinoma in situ - and is distinguished into an independent morphogenetic form of the tumor, which is still called compensated cancer (Fig. 7.2 and 7.3).
The duration of this stage can reach 10 years or more. The term “carcinoma in situ” was proposed by A. Broders (1932) and in a broad sense means cancer that is not invasive (does not extend beyond the basal membrane of the epithelium). However, to this day, debate continues about whether carcinoma in situ is cancer or precancer.
And yet, in recent years, most oncologists have recognized that carcinoma in situ is a borderline stage of malignancy and is a cancer with all the attributes of cytological malignancy, with the exception of a formed tumor node, invasive growth into the underlying tissue and metastasis.
In recent years, the term “intraepithelial tumor” is more often used to characterize such transitional changes (for example, CIN - cervical intraepitelial neoplasia - for the epithelium of the vaginal portion of the cervix, or PIN - proctatic intraepitelial neoplasia - for the prostate glands, etc.).
Morphologically, the epithelial layer affected by carcinoma in situ is represented by anaplastic tumor cells and has all the features of polymorphism characteristic of cancer (violation of the vertical direction of the arrangement of cells in the layer, nuclear polymorphism, nuclear-cytoplasmic ratio in favor of the nucleus, increased mitotic activity, pathological mitoses) ( Fig. 7.2 and 7.3).
Rice. 7.2. Morphological characteristics of dysplasia of varying degrees of development and carcinoma in situ. BM - basement membrane. [Gantsev Sh.Kh., Khusnutdinov Sh.M., 2003]
Rice. 7.3. Morphological continuum. Diagrammatically shows changes from normal epithelium to invasive and metastatic cancer.
Although invasive growth is still absent, the process is already accompanied by lymphohistiocytic infiltration in the underlying subepithelial base.
Carcinoma in situ is most often diagnosed in the uterus, bladder, lungs, breast and oral mucosa, but can probably exist in all organs and tissues.
Thus, the term “carcinoma in situ” reflects the dynamic balance between oncogenic tendencies and the body’s defense reactions. It can easily be disrupted under the influence of modifying factors that are difficult to take into account in a specific situation.
However, in clinical oncology it is firmly established that carcinoma in situ, in contrast to precancerous diseases, is an irreversible carcinogenic process that inevitably sooner or later turns into classic cancer.
Clinical practice shows the correctness of the view of carcinoma in situ as a borderline form of cancer. In the latest ICD-O classification, pre-invasive cancer is included in the “neoplasms” category, and according to the TNM system it has a special designation - Tis.
During this period, the cancer does not yet show signs of invasive growth, but breakthrough of the basement membrane and metastasis can occur at any time. There is no guarantee that the lesion will be benign. Therefore, with the current standards of treatment, the interpretation of such changes as precancer (and not cancer) can lead to dire consequences.
Bibliography
- ICD-10 (International Classification of Diseases)
- Yusupov Hospital
- Cherenkov V. G. Clinical oncology. — 3rd ed. - M.: Medical book, 2010. - 434 p. — ISBN 978-5-91894-002-0.
- Shirokorad V.I., Makhson A.N., Yadykov O.A. The state of oncourological care in Moscow // Oncourology. - 2013. - No. 4. - P. 10-13.
- Volosyanko M.I. Traditional and natural methods of preventing and treating cancer, Aquarium, 1994
- John Niederhuber, James Armitage, James Doroshow, Michael Kastan, Joel Tepper Abeloff's Clinical Oncology - 5th Edition, eMEDICAL BOOKS, 2013